Journal of caring sciences, 9(3), 133-139; DOI:10.34172/jcs.2020.020
Original Article
The Effect of Supportive-Training Intervention on the Burnout of Mothers with Disabled Child: A Randomized Clinical Trial
Zohreh Masoumi1, Fatemeh Abdoli2,3, Shayesteh Esmaeilzadeh4, Tabandeh Sadeghi5 ,6,*
1
Department of Medical Surgical Nursing, Student Research Committee, School of Nursing and Midwifery, Rafsanjan University of Medical Sciences, Rafsanjan, Iran
2
Geriatric Care Research Center, Rafsanjan University of Medical Sciences, Rafsanjan, Iran
3
Departmen of Community Health Nursing, School of Nursing and Midwifery, Rafsanjan University of Medical Sciences, Rafsanjan, Iran
4
Department of Midwifery, School of Nursing and Midwifery, Rafsanjan University of Medical Sciences, Rafsanjan, Iran
5
Non-Communicable Diseases Research Center, Rafsanjan University of Medical Sciences, Rafsanjan, Iran
6
Department of Pediatric Nursing, School of Nursing and Midwifery, Rafsanjan University of Medical Sciences, Rafsanjan, Iran
Email: t.b_sadeghi@yahoo.com
© 2020 The Author(s).
Abstract
Introduction: Mothers with a disabled child experience excessive stress, fatigue, frustration, and depression. Failure of mothers to effectively deal with these symptoms can lead to chronic fatigue and, in the long run, burnout. The objective of the present study was to determine the effect of supportive-training intervention on the burnout of mothers with disabled children.
Methods: In this randomized controlled trial, 70 mothers with disabled children studying in special schools were selected in one of the urban areas of Iran. They were divided into two groups of intervention and control, using Minimization Random Method. In the intervention group, mothers participated in supportive-training sessions once a week for a period of 6 weeks. The control group did not receive any special interventions. The data collection tool was a demographic data form and Shirom-Melamed Burnout Questionnaire (SMBQ). Burnout was evaluated as primary outcome at the beginning of the study and one month after the end of the intervention. The data were analyzed by SPSS software version 18.
Results: Based on the results, there was no significant difference between the mean score of burnout in the intervention and control groups before the intervention. However, after the intervention, the mean score of burnout in the intervention group was significantly lower than that of the control group.
Conclusion: Considering the positive effect of supportive-training intervention on the burnout of mothers of disabled children, this intervention is recommended by nurses and other health care providers in special schools, health centers, and supportive institutions.
Keywords: Burnout, Supportive-Training intervention, Mothers, Disabled child
Introduction
From the World Health Organization (WHO) point of view, disability is a disturbance in the relationship between oneself and the environment.1 Intellectual disability is not a new subject and in every period and time there have been people in the society with abnormal mental activities.2 According to the definition by the American Association on Intellectual and Developmental Disabilities (AAIDD), intellectual disability should be classified based on the downfall of intelligence performance, strength and weakness in some adaptive skills of the child with the real world; however, this condition must start before the age of 18. According to the WHO, around 10% of the world’s population (650 million) suffer from a certain type of disability, and the UNICEF estimated the number of disabled children to be 150 million in 2005.1 Intellectual disability, deafness, and blindness are among the most important causes of disability in children.3 In the 2006 census in Iran, 1 012 222 people were estimated to have disabilities, 14% of whom were under 15 years of age.4
A child’s disability has a profound effect on the entire family system and its various functions. It can damage the family’s coherence and structure, the consequence of which may change the roles, performance, and family adaptation.5 Parents, especially the mothers, experience more stress than the other members of the family, due to their special role in pregnancy, childbirth, and children upbringing.6 The results of the study by Brandon, indicated that mothers of children with intellectual disability have less time to engage in enjoyable activities, recreations, and occupations. Therefore, they are more vulnerable due to the limited time they allocate to themselves.7 Parents of children with intellectual disability could also have psychological and social problems; however, mothers had comparatively more problems due to multiple roles they usually play in the family structure.6 Atefvahid et al., also demonstrated that mothers of children who are blind and deaf or have intellectual and movement disabilities have the highest rates of parental stress.8
Mothers of disabled children experience excessive stress, fatigue, frustration, depression, and other psychological problems. Failure of mothers to effectively deal with these symptoms can lead to chronic fatigue and, in the long run, burnout.9
Burnout syndrome includes a set of symptoms of physical, emotional, and cognitive fatigues due to long-term stress exposure.10 The symptoms of burnout in mothers of intellectually disabled children are far more common than in mothers of healthy children.11 Based on the results of the study by Norberg, titled “Burnout in the parents of brain tumor survivors”, which was performed on 24 mothers and 20 fathers in Stockholm, more than half of the mothers and about 20% of the fathers had burnout symptoms.12 According to the results of a study by Lindstrom et al.,13 parents of children with chronic diseases, compared to parents of healthy children, revealed more burnout symptoms (36% vs. 20%). Basaran et al., note that caregivers of children with cerebral palsy had poorer quality of life, lower mental health, and higher burnout levels compared to the control group.14
In order to help families to deal with high levels of stress and, consequently, burnout, providing a training program regarding disabled child care can be effective. Bilgin and Gozum reported a reduction in the burnout level experienced by mothers of intellectually disabled children when they attended educational programs designed for this purpose.9 Lindstrom et al., reported that 56.3% of parents of children with chronic diseases (diabetes mellitus type 1 and inflammatory bowel disease) reported that group intervention led to their better knowledge of burnout and 43.8% of the participants reported a dramatic increase in their knowledge of burnout.10
Various studies have also been conducted in Iran on the issue of burnout. For example, Aliakbarzadeh-Arani et al., revealed the positive effect of education based on the adaptation model on social adjustment of the mothers of intellectually disabled children.15 Along the same line, Parvinian et al., indicated that the designed supportive program could be an effective way to improve the mental health of mothers of children with cerebral palsy.16 Concerning spiritual and religious interventions, one can also refer to the studies by Zafarian et al.,17 and Beheshtipour et al.,18 both of whom have underscored the positive effects of religious-spiritual interventions on stress, anxiety and depression,17 and burnout18 of parents and careers of children with cancer. However, we did not manage to find a study on the burnout of mothers with disabled children to have been conducted in Iran, combining supportive-training interventions on burnout. Therefore, in view of this gap and considering the fact that there comparatively few facilities in this particular urban area with is no specific educational and supportive program for these mothers, this study aimed to determine the effect of supportive-training intervention on the burnout of mothers with disabled children.
Materials and Methods
The research population were mothers of disabled children studying in special schools in one of the urban areas of Iran. The sample size was calculated, including the standard deviation (0.68 vs 0.56) for the burnout score based on the previous study 18 and the effect size of 0.5, 0.9 power of test, 95% confidence, and considering the sample drop for each group, 35 subjects and a total of 70 subjects were estimated.
The sampling method was convenience. Random allocation was conducted by random stratified sampling, using the method of minimization in two groups of intervention and control. In this method, the strata were first formed based on the important variables of the research, which included the burnout score and occupation. Afterwards, from the mothers who met the inclusion criteria, the first participants (20%) were placed in one of the groups by random number table and the other participants were allocated to another group with a lower total of variables (burnout score and occupation). In case of equality, we repeated the random allocation.19 This process was performed by the first author in word software.
The inclusion criteria were burnout score above 2.75, signing a written consent form, not being in another counseling program at the same time with the study, no experience of crisis such as divorce, death of a loved one, or a factor affecting burnout during the last 6 months. Not attending the training courses for more than one session was the exclusion criterion from the study. The study process from recruitment to analysis is shown in Consolidated Standards of Reporting Trials (CONSORT) flow diagram (Figure 1).
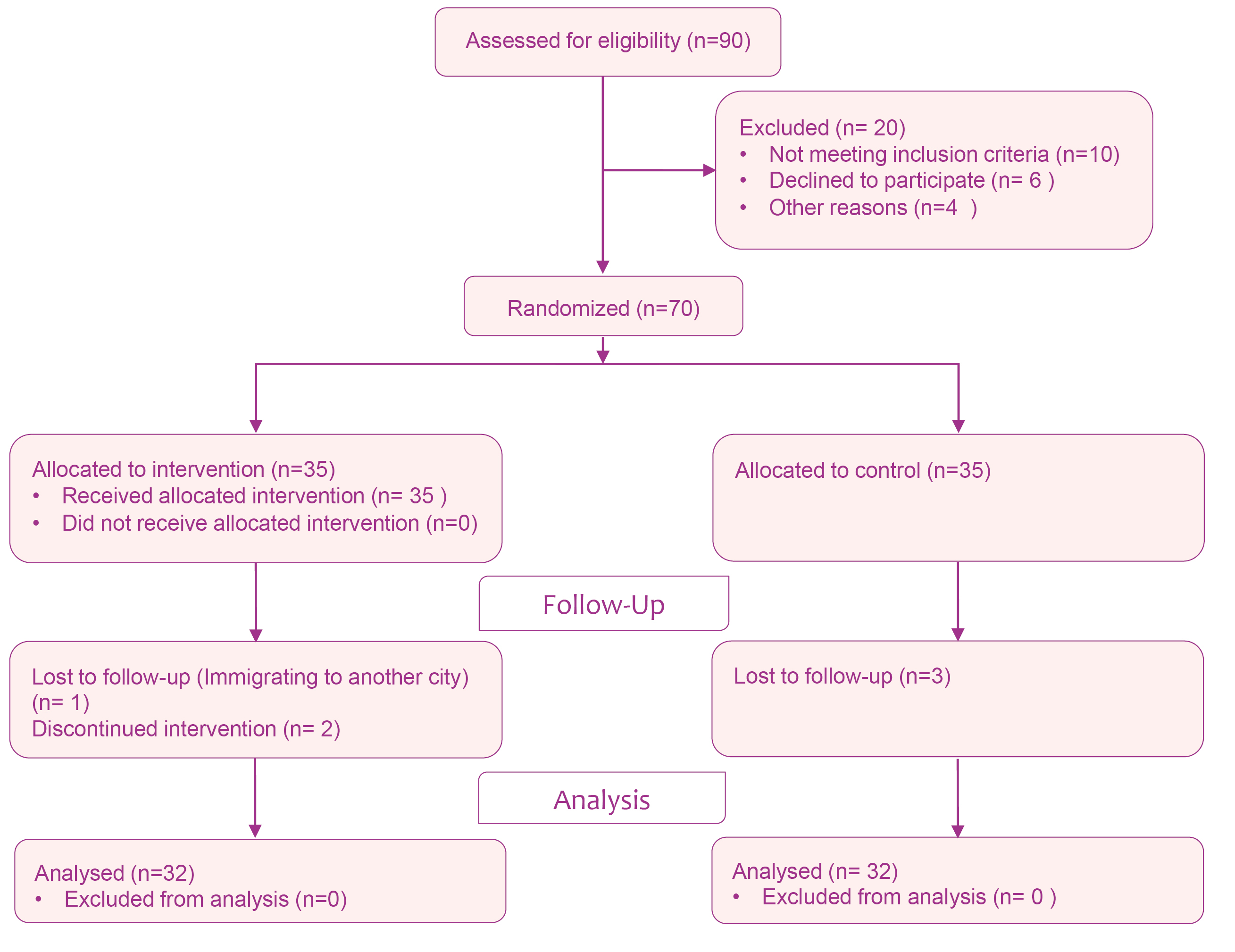
Figure 1. Flowchart of the study.
The data collection tool was a form of demographic information on mothers (age, level of education, occupation, income level, age of the child, etc.) and Shirom-Melamed Burnout Questionnaire (SMBQ). The SMBQ was developed by Shirom and Melamed in Sweden in 1989. This questionnaire was translated into Persian by Beheshtipour et al.,18 in 2013. In this study18 the reliability of the research tool was 0.91 according to Cronbach’s alpha and its validity was confirmed through content and face validity. The content validity was also approved by the experts in the present study.
The SMBQ questionnaire includes 22 questions in 4 areas of physical fatigue, cognitive weariness, tension, and listlessness. Physical fatigue included 8 questions (questions number 1-2-3-4-6-8-9-10), cognitive weariness included 6 questions (questions 17-18-19-20-21-22), tension
included 4 questions (questions 13-14-15-16), and listlessness included 4 questions (questions 5-7-11-12). Each question has 7 choices to answer, and the answer intensity to each question during the day is from choice 1 (hardly ever) to choice 7 (always), with the person filling in the questionnaire choosing from choice 1 to 7. Five questions in the questionnaire (questions 2, 14 and 5-7-11) had reverse scores. To analyze the scores in each area, the total scores of each area, were divided by the number of the questions. The range of the score remains between 1 and 7.18
First, the demographic data form and the SMBQ was completed by the mothers. Then, samples that had a burnout score above 2.75 were included in the study and were assigned to the intervention and control groups. In the intervention group mothers attended the training sessions organized by the research team at the children’s school once a week for 45 minutes for 6 weeks. The content of the session was designed based on the studies by Beheshtipour et al.,18 and Bilgin & Gozum.9 A psychologist and a spiritual counselor also helped to hold meetings. The control group did not receive any trainings. One month following the intervention, the burnout scores in both groups were evaluated using the SMBQ.
Obtaining written consents, assuring the samples of their confidentiality of the information, obtaining a license from the Research Deputy of Rafsanjan University of Medical Sciences and obtaining a license from the Rafsanjan Education and Training Deputy and School Administration were the ethical considerations observed in the study. Also, after the study was completed, the educational materials were prepared in the form of a pamphlet and given to the control group in view of its positive effects.
Supportive-training program in six weeks and related controls were as follow:
Introduction, obtaining inform consent from research units, expressing the research objectives, and educational discussions about the characteristics and care of disabled children.
Educational discussion about children and skills on establishing an appropriate relationship with the disabled children.
Spiritual discussion by spiritual counselor about the role of pain and suffering in life and its constructive effect on the growth and development of moral virtues, trust and resort, patience, prayer, thanksgiving, etc.
The presence of a psychologist and responding to the questions of mothers and discussing the necessity of using adaptation mechanisms.
Expressing memories and experiences in the field of supporting resources used in case of problems and experiences in this field.
A recreational program in the presence of mothers of the intervention group in the park and summarizing the contents.
The data were analyzed by SPSS software version 18, using descriptive (mean and standard deviation) and inferential statistics (Kolmogorov–Smirnov test, independent t-test, paired t-test, chi-square). P < 0.05 was considered as the significance level.
Results
In this study, the eligibility criteria of 90 mothers were assessed. Out of these, 70 eligible mothers were included and 64 of them finished the program. Therefore, data analyzed related to 32 patients in each group. Demographic results indicate that the mean age of mothers in the intervention group was 39.22 (7.22) and in the control group was 38.50 (7.11) and the mean age of the disabled children in the intervention group was 9.72 (2.99) and in the control group was 10.44 (2.95). The majority of the mothers in the two groups were housewives and were almost the same in terms of demographic characteristics (Table 1).
|
Table 1.Comparison demographic characteristics of mothers in intervention (n=32) and control groups (n=32)
|
|
Demographic characteristics
|
Intervention group No. (%)
|
Control group
No. (%)
|
P
value
a
|
| Job |
|
|
|
0.49 |
|
Housewife |
32 (100) |
30 (93.8) |
|
|
Employed |
0 (0) |
2(6.2) |
|
| Mother's age (year) |
|
|
|
0.51 |
|
25-35 |
11 (34.4) |
15 (46.9) |
|
|
36-45 |
13 (40.6) |
12 (37.5) |
|
|
>45 |
8 (25.0) |
5 (15.6) |
|
| Education level |
|
|
|
0.12 |
|
Below diploma |
23 (71.9) |
16 (50.0) |
|
|
Diploma and higher |
9 (28.1) |
16 (50.0) |
|
| Economic situation |
|
|
|
0.74 |
|
Good |
4 (12.5) |
6 (18.8) |
|
|
Medium |
17 (53.1) |
17 (53.1) |
|
|
Weak |
11 (34.4) |
9 (28.1) |
|
| Age of disabled child (year) |
0.44 |
|
<10 |
21 (65.6) |
18 (56.3) |
|
|
>10 |
11 (34.4) |
14 (43.8) |
|
| Number of disabled child |
0.49 |
|
1 |
32 (100.0) |
30 (93.8) |
|
|
2 |
0 (0) |
2 (6.2) |
|
|
aChi-square test.
|
The normal distribution of the data was confirmed, using Kolmogorov–Smirnov test (P >0.05). Based on the results, the mean score of burnout before the intervention was 3.82 (0.66) in the intervention group and 3.75 (0.91) in the control group and did not have a significant difference from each other (independent t test; P = 0.71). After the intervention, the mean score of burnout in the intervention group was 3.25 (0.95), which was significantly lower than that of the control group 4.05 (0.99) (independent t test; P = 0.002). Intra-group comparison revealed no significant difference in the mean score of burnout before and after the intervention (P = 0.07) in the control group; however, in the intervention group, the mean score of burnout after the intervention was significantly lower than that before the intervention (paired t; P = 0.001)
Based on the results, before the intervention, the two groups were homogeneous in terms of different dimensions of burnout, but after the intervention, independent t-test indicated a significant statistical difference between the mean score of physical fatigue, cognitive weariness, and the mean score of stress between the two groups while this difference was not significant between the two groups in terms of listlessness (Table 2).
|
Table 2. Comparison mean and standard deviation of burnout dimensions in mothers between intervention (N=32) and control groups (N=32) before and after intervention
|
|
Time
|
Variables
|
Intervention group
n=32
Mean (SD)
a
|
Control group
n=32
Mean (SD)
a
|
MD (95% CI)
b
|
P
value
c
|
| Before intervention |
|
|
|
|
|
|
Physical fatigue |
3.81(0.94) |
3.82(1.11) |
-0.53(0.51) |
0.95 |
|
Cognitive weariness |
4.02(1.18) |
3.83(1.32) |
-0.44(0.81) |
0.55 |
|
Tension |
3.71(0.84) |
3.47(1.06) |
-0.23(0.72) |
0.31 |
|
Listlessness |
3.67(1.06) |
3.75(1.11) |
-0.62(0.46) |
0.77 |
| After intervention |
|
|
|
|
|
|
Physical fatigue |
3.35(1.13) |
4.24(1.24) |
-1.49(-0.29) |
0.004* |
|
Cognitive weariness |
3.08(1.08) |
4.24(1.41) |
-1.81(-0.54) |
0.001* |
|
Tension |
3.18 (0.92) |
3.94 (1.25) |
-1.31(-0.21) |
0.008* |
|
Listlessness |
3.36(1.31) |
3.46(0.98) |
-0.67(0.48) |
0.74 |
|
aMean (Standard Deviation), bMean Difference (95% confidence interval),cIndependent t-test, *Statistically significant
|
Paired t test demonstrated a significant difference between the mean score of physical fatigue, cognitive weariness, and the mean score of stress in the intervention group before and after the intervention while this difference was not significant in terms of listlessness. In the control group, the mean scores of physical fatigue and stress were significant and increased compared to before the intervention. There was no significant difference in the dimensions of cognitive weariness and listlessness compared to before the study (Table 3).
|
Table 3. Comparison mean and standard deviation of burnout dimensions in mothers in two groups of intervention and control before and after intervention
|
|
Groups
|
Variables
|
Before intervention
Mean(SD)
a
|
After the intervention
Mean(SD)
a
|
P
b
|
| Intervention |
|
|
|
|
|
Physical fatigue |
3.81 (0.94) |
3.35 (1.13) |
0.04* |
|
Cognitive weariness |
4.02(1.18) |
3.08(1.08) |
0.001* |
|
Tension |
3.71(0.84) |
3.18(0.92) |
0.01* |
|
Listlessness |
3.67 (1.06) |
3.36(1.31) |
0.12 |
| Control |
|
|
|
|
|
Physical fatigue |
3.82(1.11) |
4.24(1.24) |
0.04* |
|
Cognitive weariness |
3.83(1.32) |
4.26(1.41) |
0.11 |
|
Tension |
3.47(1.06) |
3.94(1.25) |
0.03* |
|
Listlessness |
3.75(1.11) |
3.46(0.98) |
0.25 |
|
aMean (standard deviation), bPaired t-test, *Statistically significant.
|
Discussion
Based on the results of the current study, after 6 weeks of supportive-training intervention, the mean score of burnout in the intervention group was significantly lower than that of the control group. Paired comparison indicated that there was no significant difference in the mean score of burnout before and after the intervention in the control group; however, in the intervention group, the mean burnout score after the intervention was significantly less than that before the intervention. In this regard, the results of the study by Beheshtipour et al., consistent with the present study, indicated that training-spiritual intervention was effective in reducing burnout score immediately after and one month after the intervention in parents of children with cancer.18 It can be stated that families with strong religious beliefs have a better adaptability to their child’s illness. These people receive emotional and psychological support from their beliefs. They believed that God provided them with help and support and participation in religious ceremonies calmed them down. Thus, the use of spiritual intervention is recommended for better adaptation of these families.
The results of the study by Bilgin and Gozum, consistent with the present study, indicated that attending the nursing training program for two weeks every day, reduced the levels of burnout experienced by mothers of intellectually disabled children.9 According to the results of the study by Lindstrom et al., in line with the current study, 56.3% of the parents of children with chronic diseases reported that the group intervention led to their better knowledge of burnout, and 43.8% reported a dramatic increase in their knowledge of burnout.10 In Iran, the results of the study by Parvinian et al.,16 also indicated the positive effect of family training and supportive programs on the psychological and mental health of parents with intellectually disabled children. In this regard, according to the results of the current study and above mentioned studies, it can be stated, mothers who are faced with stressful situations, like having a child with chronic diseases, seek information from the health care workers that help them determine their position. Therefore, it can be concluded that providing suitable and adequate information and emotional support to reduce the stress of these mothers is helpful and recommended.
Based on the results, there was a significant difference between the mean score of physical fatigue, cognitive weariness, and tension between the two groups after the intervention while the difference between the two groups was not significant in terms of listlessness. There was a statistically significant decrease for the mean score of physical fatigue, cognitive weariness, and tension in the intervention group after the intervention. In the control group, the mean score of physical fatigue and tension were significant and increased compared to before the intervention.
Concerning the issue of fatigue, Giallo et al., indicated that the mothers of children with autism spectrum disorder experience more fatigue compared to mothers of children with normal growth.20 The results of the study by Garip et al., demonstrated that the fatigue levels of mothers of children with cerebral palsy were higher than those of mothers of healthy children; this can be relevant with depression and deterioration of quality of life regarding physical, social and emotional performance.21 In this study, physical fatigue increased in the control group where no intervention occurred; therefore, various interventions were proposed to reduce this issue in these mothers.
Regarding the aspect of tension, Kaboudi et al., revealed that mothers who were trained in resilience skills progressed significantly in increasing the coping style and decreasing tension compared to mothers in the control group.22 Therefore, conducting the studies and the use of interventions to reduce tension in these mothers are among the other recommendations.
Performing the study in a small urban area, the limited time of the intervention and the differences in age and educational level of mothers were among the limitations of the present study; therefore, it is recommended that similar studies be conducted in larger communities more similar in age and educational level with longer intervention times.
Conclusion
Based on the findings of the current study, it can be concluded that supportive-training intervention is effective in decreasing the burnout of mothers of disabled children who are studying and can be used as a training program by nurses and other health care providers in health centers and supportive institutions.
Acknowledgments
This article was the result of a nursing MSc dissertation approved by Rafsanjan University of Medical Sciences (Project number: 31/20/1/96133). Thus, special thanks and appreciation should go to the authorities of the university, and Ms. Hassani, Ms. Afarand, Mr. Abedi and all the mothers, the head and staff of Zohreh- Shamsaei School who kindly helped us throughout this study.
Ethical Issues
This randomized controlled trial was approved by the ethics committee of Rafsanjan University of Medical Sciences (IR.RUMS.REC.1396.163) and registered on IRCT.ir (identifier: IRCT20180206038642N1).
Conflict of Interest
The authors have no conflicts of interest to declare.
Author’s Contributions
Conception and design: ZM, FA, ShE and TS; Acquisition of data: ZM; Analysis and interpretation of data: TS; Drafting the article: ZM, FA, ShE and TS; Review of article and final approval: ZM, TS, FA, ShE
Research Highlights
|
|
What is the current knowledge?
The symptoms of burnout in mothers of disabled children are far more common than in mothers of healthy children.
What is new here?
Supportive-training intervention is effective in decreasing the burnout of mothers with disabled children.
|
References
- Hockenberry MJ, Wilson D, Rodgers CC. Wong’s essentials of pediatric nursing. 10th ed. United States: Mosby; 2016.
- Meidatuzzahra D, Kuswanto H, Pech N, Etchegaray A. Population analysis of disabled children by departments in France. J Phys Conf Ser 2017; 855(1): 012025. doi: 10.1088/1742-6596/855/1/012025. [Crossref]
- Izadi-Mazidi M, Riahi F, Khajeddin N. Effect of cognitive behavior group therapy on parenting stress in mothers of children with autism. Iran J Psychiatry Behav Sci 2015; 9(3): e1900. doi: 10.17795/ijpbs-1900. [Crossref]
- Sajjadi H, Zanjari N. Disability in Iran: prevalence, characteristics, and socio-economic correlates. Archives of Rehabilitation 2015; 16(1): 36-47. [Persian].
- Basir Kia SM, Mareashian FS. Examining the effectiveness of aggression control training with cognitive-behavioral approach on marital burnout in mothers with mentally retarded children in Ahvaz. Int J Humanit Cult Stud 2016; 1(1): 1531-8.
- Yamaoka Y, Tamiya N, Izumida N, Kawamura A, Takahashi H, Noguchi H. The relationship between raising a child with a disability and the mental health of mothers compared to raising a child without disability in japan. SSM Popul Health 2016; 2: 542-8. doi: 10.1016/j.ssmph.2016.08.001. [Crossref]
- Brandon P. Time away from “smelling the roses”: where do mothers raising children with disabilities find the time to work? Soc Sci Med 2007; 65(4): 667-79. doi: 10.1016/j.socscimed.2007.04.007. [Crossref]
- Atefvahid MK, Habibi Asgarabad M, Ashouri A, Sayed Alitabar SH. Parenting stress in mothers of mentally retarded, blind, deaf and physically disabled children. Community Health 2016; 3(4): 330-40. [Persian].
- Bilgin S, Gozum S. Reducing burnout in mothers with an intellectually disabled child: an education programme. J Adv Nurs 2009; 65(12): 2552-61. doi: 10.1111/j.1365-2648.2009.05163.x. [Crossref]
- Lindström C, Åman J, Anderzén-Carlsson A, Lindahl Norberg A. Group intervention for burnout in parents of chronically ill children - a small-scale study. Scand J Caring Sci 2016; 30(4): 678-86. doi: 10.1111/scs.12287. [Crossref]
- Weiss MJ. Harrdiness and social support as predictors of stress in mothers of typical children, children with autism, and children with mental retardation. Autism 2002; 6(1): 115-30. doi: 10.1177/1362361302006001009. [Crossref]
- Norberg AL. Burnout in mothers and fathers of children surviving brain tumour. J Clin Psychol Med Settings 2007; 14(2): 130-7. doi:10.1007/s10880-007-9063-x. [Crossref]
- Lindström C, Aman J, Norberg AL. Increased prevalence of burnout symptoms in parents of chronically ill children. Acta Paediatr 2010; 99(3): 427-32. doi: 10.1111/j.1651-2227.2009.01586.x. [Crossref]
- Basaran A, Karadavut KI, Uneri SO, Balbaloglu O, Atasoy N. The effect of having a children with cerebral palsy on quality of life, burn-out, depression and anxiety scores: a comparative study. Eur J Phys Rehabil Med 2013; 49(6): 815-22.
- Aliakbarzadeh-Arani Z, Taghavi T, Sharifi N, Noghani F, Faghihzade S, Khari-Arani M. Impact of training on social adaptation in mothers of educable mentally- retarded children based on Roy adaptation theory. Feyz Journal of Kashan University of Medical Sciences 2012; 16(2): 128-34. [Persian].
- Parvinian AM, Mohammad Khan Kermanshahi S, Sajedi F. The effect of a supportive program on mental health of mothers of children with cerebral palsy. Evidence Based Care 2012; 2(3): 23-32. doi: 10.22038/ebcj.2012.407. [Crossref]
- Zafarian Moghaddam E, Behnam Vashani HR, Reihani T, Namazi Zadegan S. The effect of spiritual education on depression, anxiety and stress of caregivers of children with leukemia. Journal of Torbat Heydariyeh University of Medical Sciences 2016; 4(1): 1-7. [Persian].
- Beheshtipour N, Nasirpour P, Yektatalab S, Karimi M, Zare N. The effect of educational-spiritual intervention on the burnout of the parents of school age children with cancer: a randomized controlled clinical trial. Int J Community Based Nurs Midwifery 2016; 4(1): 90-7.
- Pandis N. Randomization. part 2: minimization. Am J Orthod Dentofacial Orthop 2011; 140(6): 902-4. doi: 10.1016/j.ajodo.2011.08.016. [Crossref]
- Giallo R, Wood CE, Jellett R, Porter R. Fatigue, wellbeing and parental self-efficacy in mothers of children with an autism spectrum disorder. Autism 2013; 17(4): 465-80. doi: 10.1177/1362361311416830. [Crossref]
- Garip Y, Ozel S, Tuncer OB, Kilinc G, Seckin F, Arasil T. Fatigue in the mothers of children with cerebral palsy. Disabil Rehabil 2017; 39(8): 757-62. doi: 10.3109/09638288.2016.1161837. [Crossref]
- Kaboudi M, Abbasi P, Heidarisharaf P, Dehghan F, Ziapour A. The effect of resilience training on the condition of style of coping and parental stress in mothers of children with leukemia. Int J Pediatr 2018; 6(3): 7299-310. doi: 10.22038/ijp.2018.29245.2559. [Crossref]