Journal of caring sciences. 12(2):116-122.
doi: 10.34172/jcs.2023.30120
Original Article
The Effect of Aromatherapy with Citrus aurantium Aroma on Pain after Orthopedic Surgery: A Randomized Clinical Trial
Sepideh Bargi Methodology, Project administration, Validation, Visualization, Writing – original draft, Writing – review & editing, 1 
Nasrin Bahraminejad Funding acquisition, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing, 2, *
Samineh Jafari Methodology, Validation, Visualization, Writing – original draft, Writing – review & editing, 3
Ramezan Fallah Methodology, Project administration, Validation, Visualization, Writing – original draft, Writing – review & editing, 4
Author information:
1Department of Nursing, School of Nursing and Midwifery, Zanjan University of Medical Sciences, Zanjan, Iran
2Social Determinant of Health Research Center, School of Nursing and Midwifery, Zanjan University of Medical Science, Zanjan, Iran
3Department of Pharmacognosy, School of Pharmacy, Zanjan University of Medical Sciences, Zanjan, Iran
4Department of Biostatistics and Epidemiology, School of Medicine, Zanjan University of Medical Sciences, Zanjan, Iran
Abstract
Introduction:
Postoperative pain is one of the most common physiological and psychological stress in patients that disrupts body function and can endanger patients’ health. This study aims to determine the effect of aromatherapy with Citrus aurantium essential on pain after orthopedic surgery.
Methods:
This randomized clinical trial was performed on 60 candidates for orthopedic surgery. Patients were selected through convenience sampling and divided into intervention and control groups through randomized block allocation. If the visual analogue scale (VAS) score was above 3, patients in the intervention group received aromatherapy with C. aurantium essential and the patients in the control group received a placebo (almond oil). VAS was used to measure pain. Data analysis was performed using independent t test, paired t test, and analysis of variance with repeated measures using SPSS software version 13.
Results:
Mean (SD) of pain intensity after intervention in experimental and control groups within 4, 8, and 12 hours after surgery was 7.30 (1.23) vs. 7.90 (0.99), 5.30 (0.98) versus 5.53 (0.68) and 2.53 (0.9) vs. 3.60 (0.77) respectively. The findings indicated that there was a significant difference in mean pain intensity between the experimental and control groups at 4 and 12 hours after surgery. Use of analysis of variance with repeated measures test with taking into account the interaction of time and group also showed a significant difference in mean pain intensity between the two experimental and control groups.
Conclusion:
Aromatherapy with Citrus aurantium essential can be effective in reducing mild to moderate pain after orthopedic surgery. Further studies are recommended to confirm this finding.
Keywords: Pain, Aromatherapy, Orthopedic surgery, Citrus aurantium
Copyright and License Information
© 2023 The Author(s).
This work is published by Journal of Caring Sciences as an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by-nc/4.0/). Non-commercial uses of the work are permitted, provided the original work is properly cited.
Introduction
The management of acute postoperative pain remains a significant challenge for physicians and nurses, especially in low- and middle-income countries.1 Postoperative pain can cause physiological and psychological complications such as fear, anxiety and feelings of helplessness.2 Failure to control postoperative pain can activate the sympathetic nervous system and increase myocardial work and oxygen demand.3 Thereby contributing to ischemia, myocardial infarction, increasing morbidity and mortality of the patients. Ineffective postoperative pain control can also lead to economic and medical problems, including the increase in hospitalization time, the need for hospital re-admission, and patients’ dissatisfaction with medical care.4 Therefore, assessment of pain intensity after surgery, its effective control and treating pain complications are of great importance.
Despite new advance in measures have been taken to control postoperative pain but the pain is an unresolved health-care challenge after surgery.5Based mostly on in hospital evidence, 86% of patients experience pain after surgery.6In non-western countries data are scared but prevalence goes up 73% to 96.66 %, which was shown in Tanzania and India.7,8In a study by Hadavi et al 40% of patients were dissatisfied with postoperative pain control in Iran.9
Orthopedic surgery results in moderate to severe pain in a majority of patients.10 Dissatisfaction with pain management in patients undergoing orthopedic surgery is common.11 Whiles, patient satisfaction is a valuable criterion in health care outcomes process and is used to improve the provided quality of care.12 According to the standards of the Commission for the Approval of Health Services Providers, pain is considered to be the fifth vital sign and should be assessed regularly from the time of admission to the discharge of the patients.13 Pharmacological interventions used to relieve postoperative pain are mainly focused on the prescription of opiate and non-steroidal anti-inflammatory drug (NSAID).14 Opioids are used as the first line of treatment for postoperative pain relief.15 Morphine is a common opiate pain reliever used to treat pain.16 Overall, systemic opioid use has been associated with complications such as nausea, vomiting, constipation, itching, and respiratory depression.17 NSAIDs can also cause skin reactions, renal complications including analgesic nephropathy and gastrointestinal complications such as peptic ulcers.18
In the last two decades, concerns about narcotics complications,19 the inability to optimally relieve pain5, increase in medical costs, and the length of hospital stay20 have led to the use of non-pharmacological approaches including music,21massage,22and aromatherapy.23 The effect of different fragrances on pain has been studied by different researchers.24,25 One of the aromatic volatile oils that is widely used in aromatherapy, is oil extracted from Citrus aurantium plant. C. aurantium is native to tropical Asia but it also grows in all tropical and subtropical regions.26 The constituents of C. aurantium essential oil are more than ten, most of which are linalool, neryl acetate, limonen, beta-pinene, myrcene and alpha-terpinylacetate.27 The myrcene is a monoterpene composition and has analgesic, sodium channel blocking and muscle relaxant effects.28 Limonene in C. aurantium essential oil inhibits the activity of prostaglandins by controlling cyclooxygenase I and II and thus is effective in reducing pain.29 No specific side effects related to the use of C. aurantium essential oil has been reported through studies.30
Namazi et al through an experimental study used the effect of C. aurantium essential oil on pain intensity of the active phase of labor in nulliparous women. The results of the study showed that mean pain was significantly decreased in the group treated with C. aurantium essential oil compared to the control group.31 In another study, Sharifipour et al used the effect of C. aurantium essential oil on anxiety after the cesarean section on 80 women undergoing surgery. The results of this study also showed a significant decrease in anxiety in the intervention group compared with the control group.23 A study conducted by Chen and Xie in China also showed that postoperative aromatherapy with C. aurantium was effective in relieving pain in patients undergoing gastrectomy.32So considering the importance of postoperative pain relief and easy and cost-effective availability of C. aurantium essential oil and few studies about the effect of C. aurantium essential oil on postoperative acute pain, this study was developed to investigate the effect of aromatherapy with C. aurantium aroma on pain after orthopedic surgery.
Materials and Methods
The current study was a double-blind clinical trial (registration code: IRCT20140304016843N13). The study was carried out on 60 patients undergoing elective orthopedic lower limb surgery (femur or tibia) referring to Ayatollah Mousavi Hospital, Zanjan, Iran between October 29, 2018, and February 9, 2019). The sample size was determined according to a confidence interval of 95% and test power of 80% and according to a similar study33 and considering the probability of sample loss in the experimental group (n = 30) and control group (n=30). The patients chosen by convenience sampling were divided by random allocation method into experimental and control groups. The sequence of sample allocation in the two groups was determined as follows: First, the letters A and B were assigned to each of the two groups under study, and then the size of the blocks (4, twice the number of groups) was determined. To avoid bias - the choice of the block size was not mentioned with the aid of research assistants. After itemizing approximately all modes of 4 blocks (AABB, ABAB, BABA, BBAA, ABBA, BAAB) and assigning a number to each one, based on a random number table, 15 blocks were selected to increase the number of samples to 60 patients (30 patients in the experimental group, 30 patients in the control group). It should be noted that the rooms of patients treated with the aroma of orange spring were separated from the rooms of patients treated with a placebo (sweet almond oil) in order to avoid mixing the aroma of spring orange and sweet almond oil, which inadvertently leads to contamination of samples in the control group.
Blinding was performed for patients who participate in the study and the researcher assistant who performed the intervention in the study, namely patients in the experimental and control groups were in separate rooms without any contact, and C. aurantium was introduced to them as drug A and almond oil as drug B. Though, the fragrance of C. aurantium may have been familiar to them. But none of the patients knew they were in the experimental or control group. Also, for the researcher assistant who performed the intervention, C. aurantium was again introduced as drug A and almond oil as drug B. To avoid researcher bias, pain measurement after the intervention was performed with the help of another researcher assistant.
Those patients who met all the inclusion criteria were included in this study. The inclusion criteria were as follow: having orthopedic surgery, no surgical history, full alertness, and postoperative co-operation, self-reported a normal sense of smell and visual state to see the visual analogue scale (VAS) for pain intensity; being 15 years old and over; having no history of herbal allergies, psychological disorder, coagulation disorders, diabetes, and respiratory problems, and addiction according to the patient record. Exclusion criteria included having postoperative complications (such as hemorrhage, and hematoma at the site of operation), the need for postoperative oxygen therapy, and the patient’s unwillingness to participate after performing the first intervention. Before surgery, patients selected for the experimental group was evaluated for allergy to C. aurantium. To do this, a drop of C. aurantium essential oil was poured into the patient’s wrist, and it was immediately dressed to reduce inhalation. After two minutes the dressing was removed. None of the participants showed allergic reactions. During the intervention phase, in the experimental group, if the patients who underwent lower orthopedic surgery, their pain score by using the VAS instrument was more than 3 after 4,8,12 hours after surgery, 4 drops of C. aurantium essential oil was poured on a cotton ball and the patient was asked to inhale it for 5 minutes at a distance of 20 cm. Then, after 20 minutes, the pain intensity was measured again on the VAS. In the control group, similar to the intervention group at 4, 8 12 hours after surgery, the severity of pain was assessed using the VAS instrument. If their postoperative pain score was more than 3, they were treated with sweet almond oil and then 20 minutes later, similar to the experimental group; their pain intensity was assessed and recorded. Patients in both groups also received routine medications to relieve pain. C. aurantium essential oil 10% and sweet almond oil (as a placebo) were supplied from the Ayat essence company, Iran. The amount of essential oil was based on a literature review34 and consultation with an herbalist.
The instrument used for data collection comprises two parts: The first part consists of demographic data and contextual variables such as age, sex, marital status, educational level, occupation, place of residence, and underlying diseases such as sinusitis and allergy was completed by interview. The second part consisted of the VAS tool. Studies in Iran and outside Iran confirmed the validity and reliability of the VAS tool.35,36
Analyzing data was carried out by employing SPSS version 13. An independent t-test was used to compare the pain intensity between the experimental and control groups before the intervention. An analysis of variance with repeated measures was used to compare the pain intensity before and after the intervention in both experimental and control groups (during three stages of intervention). Generalized estimating equations models were used to evaluate the effect of intervention time and the interaction effect of intervention time on pain intensity changes in the experimental and control groups. The level of statistical significance was set at P<0.05) (Figure 1).
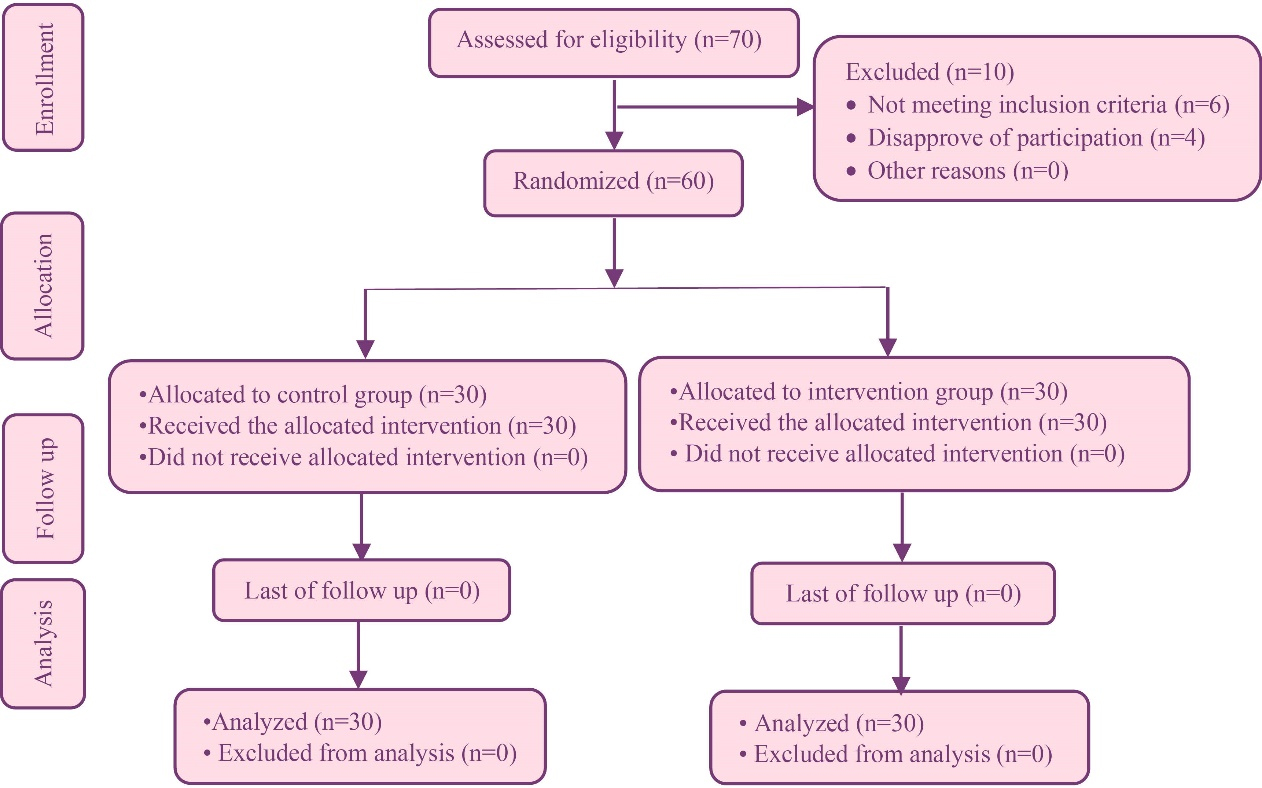
Figure 1.
Flow chart of the study
.
Flow chart of the study
Results
The mean (SD) age of the participants in the experimental and control groups was 38.73 and 42.83 years, respectively. Most of the patients were married in the experimental group 60 (18) and in the control group 70 (21). The majority of patients in the experimental group 70 (21) and the control group 63.3 (19) had no history of hospitalization. In addition, concerning the type of surgery, the majority 83.3 (25) underwent surgery in the femur area.
As Table 1 shows, participants in the experimental and control groups did not have significant differences in terms of contextual and demographic variables. According to the results the mean of pain in both experimental and control groups before intervention in each the three stages of 4, 8, and 12 hours after the operation was not significant. However, the mean of pain after intervention in all three stages decreased in the experimental group compared to the control group. So that, the mean (SD) of pain intensity in the first 4 hours after surgery in the experimental group compared to the control group was 7.30 (1.23) vs. 7.90 (0.99), at 8 hours after surgery was 5.30 (0.98) versus 5.53 (0.68) and at 12 hours after surgery was 2.53 (0.9) vs. 3.60 (0.77). Moreover, there was a significant difference in mean pain intensity between the two groups at 4 and 12 hours after surgery (Table 2). Use of repeated measurement test with taking into account the interaction of time and group also showed a significant difference in mean pain intensity between two experimental and control groups.
Table 1.
Demographic and contextual variable of participant in the experimental and control group
|
Variables
|
Mean (SD)
|
P
value
a
|
|
Experimental group (n=30)
|
Control group (n=30)
|
| Habitat |
| Urban |
22 (73.7) |
19 (63.3) |
0.58 |
| Rural |
8 (26.7) |
11 (36.7) |
| Surgical site |
| Femur |
25 (83.3) |
5 (16.7) |
0.99 |
| Tibia |
25 (83.3) |
5 (16.7) |
| Health insurance |
| Yes |
24 (80) |
26 (86.7) |
0.73 |
| No |
6 (20) |
4 (13.3) |
| Income |
| Relatively adequate |
8 (26.7) |
7 (23.5) |
0.99 |
| Inadequate |
22 (73.3) |
23 (76.7) |
| Surgeon |
| A |
23 (76.7) |
22 (73.3) |
0.76 |
| B |
7 (23.3) |
8 (26.7) |
| History of hospitalization |
| Yes |
9 (30) |
11 (36.7) |
0.58 |
| No |
21 (70) |
19 (63.3) |
| Type of analgesic |
| Morphine |
10 (33.3) |
12 (40) |
0.59 |
| Pethidine |
20 (66.7) |
18 (60) |
Table 2.
The mean and standard deviation in experimental and control groups in terms of time measurement
|
Time
|
Group
|
Group
|
Time
|
Hour
|
|
Experimental group (n=30)
|
Control group (n=30)
|
|
Before intervention
|
After intervention
|
Before intervention
|
After intervention
|
|
Mean (SD)
|
CV%
|
Mean (SD)
|
CV%
|
Mean (SD)
|
CV%
|
Mean (SD)
|
CV%
|
F
|
Df
|
P
|
F
|
Df
|
P
|
F
|
Df
|
P
|
| 4 hours after surgery |
8.23(0.89) |
10.9 |
7.30(1.23) |
16.9 |
8.10(1.09) |
13.5 |
7.90(0.99) |
12.6 |
8.15 |
1 |
0.005 |
56.84 |
1 |
0.001 |
61.70 |
2 |
0.001 |
| 8hours after surgery |
5.77(0.81) |
14.2 |
5.30(0.98) |
18.6 |
5.7(0.70) |
12.3 |
5.53(0.68) |
12.3 |
| 12 hours after surgery |
4.40(0.72) |
16.5 |
2.53(0.90) |
35.5 |
4.37(0.49) |
11.2 |
3.60(0.77) |
12.4 |
Discussion
This study aimed to evaluate the effect of aromatherapy with C. aurantium on postoperative orthopedic (lower limb) pain. The findings of the study indicated that aromatherapy with C. aurantium had a significant effect on postoperative pain reduction of the patients. Of course according to the findings, the highest reduction in pain score was related to 12 hours after surgery (1.87 in the experimental group compared to 0.77 in control group). Based on these findings, the use of aromatherapy with C. aurantium seems to be more effective when the pain intensity is mild and moderate. The study by Sharifipour et al on the effects of aromatherapy with C. aurantium and Salvia officinalis oil on the pain after cesarean section at 4, 8 and 12 hours after surgery showed that aromatherapy with both C. aurantium and S. officinalis had significant and equal effects on pain relief after cesarean section which is in line with the results of the present study.34 Namazi et al study on the effect of C. aurantium on pain intensity of active phase of labor also showed that the use of C. aurantium essential oils in women reduced the intensity of labor pain at different stages of labor.31 Yip and Tam in their study showed that massage with combined aromatherapy of C. aurantium and ginger essential oils was effective in relieving moderate to intensive knee pain.37
The antinociceptive activities of C. aurantium can be explained in two ways. First, the aroma-induced odor appears to stimulate the olfactory nerve cells and subsequently the limbic system. Depending on the type of aroma, the neurons release different neurotransmitters. These neurotransmitters include enkephalin, endorphin, noradrenaline, and serotonin which are capable of altering the feelings in humans through odors. On the other hand, myrcene present in C. aurantium is a monoterpene compound which is antinociceptive, sodium channel blocking and muscle relaxant. Also, limonene in C. aurantium essential oil restrains the activity of prostaglandins by inhibiting cyclooxygenase I and II and by this way, it is effective in reducing pain.28,29
As the findings showed, the pain reduction was more significant in the experimental group but the changes in pain intensity in the control group were also significant at 12 hours after surgery. One of the causes of pain reduction in the control group can be due to the passage of time. On the other hand, pain reduction in the control group, including the effects of placebo on pain relief, is due to the role of psychological factors in pain relief. However, the present study confirms the results of previous studies on the effect of C. aurantium on acute pain.32,34 Based on the definition of acceptable effect size to consider the anti-nociceptive effect of any treatment that is equivalent to a 30% reduction in pain severity,38 it can be said, though the use of C. aurantium caused a significant difference in pain intensity in the experimental group compared to the control group, but the anti-nociceptive effects were not clinically significant in the first 4 and 8 hours postoperatively, and the most anti-nociceptive effect occurred at 12 hours postoperatively (when the patient’s pain was mild to moderate). Therefore, due to the acceptable size effect on pain relief, the therapeutic effects of C. aurantium especially during the first 4 and 8 hours after surgery were not significant. The therapeutic methods of anti-nociceptive effects of C. aurantium especially in the first 4 and 8 hours after the operation were not significant and it can be said that aromatherapy with C. aurantium has been used to reduce pain along with other medication interventions, and most when the intensity of pain is at a moderate or moderate level.
One of the advantages of this study is that C. aurantium has public acceptance, and another advantage compare with similar studies is that the current study determined the pain intensity level affected by C. aurantium. While other studies nearly deems general nociceptive effect of C. aurantium.
Considering the impact of gender (participants were only men) and age on pain experience, the results of this study cannot be generalized to all types of acute pain, female gender, all age groups, and cultures. Further studies on the anti-nociceptive effects of C. aurantium in other patients and chronic pain and cancer pain are recommended.
Conclusion
Aromatherapy with C. aurantium aroma had positive effect on reducing orthopedic postoperative pain mainly in mild to moderate pain. Therefore, this intervention can be applied by nurses to decrease postoperative pain along with other medication interventions.
Acknowledgments
The present study is based on a master thesis in nursing. We would like to express our deep sense of gratitude to the Vice Chancellor for Research and Technology of Zanjan University of Medical Sciences, the staff of Ayatollah Mousavi Hospital and the participants in this study.
Author’s Contribution
Conceptualization: Sepideh Bargi, Nasrin Bahraminejad, Samineh Jafari, Ramezan Fallah.
Data curation: Sepideh Bargi.
Formal analysis: Sepideh Bargi, Nasrin Bahraminejad, Ramezan Fallah.
Funding acquisition: Nasrin Bahraminejad.
Investigation: Nasrin Bahraminejad.
Methodology: Sepideh Bargi, Nasrin Bahraminejad, Samineh Jafari, Ramezan Fallah.
Project administration: Nasrin Bahraminejad Sepideh Bargi.
Software: Ramezan Fallah.
Supervision: Nasrin Bahraminejad, Samineh Jafari.
Validation: Sepideh Bargi, Nasrin Bahraminejad, Samineh Jafari, Ramezan Fallah.
Visualization: Sepideh Bargi, Nasrin Bahraminejad, Samineh Jafari, Ramezan Fallah.
Writing–original draft: Sepideh Bargi, Nasrin Bahraminejad, Samineh Jafari, Ramezan Fallah.
Writing–review & editing: Sepideh Bargi, Nasrin Bahraminejad, Samineh Jafari, Ramezan Fallah.
COI-statement
The authors declared no conflict of interest in this study.
Data Availability
The datasets are available from the corresponding author on reasonable request.
Ethical Approval
The present study has been extracted from master degree dissertation. The ethical permission for the study was obtained by the Ethics Committee of the Zanjan University of Medical Sciences (ethics code: IR.ZUMS.REC.1397.14). In this way, the researcher first provided the participants with the necessary information about the study, its aims, the right to leave the study at any stage of the intervention, and the confidentiality of their personal data, and after they met the inclusion criteria, written informed consent was obtained from them before initiation of the study.
Funding
This study was funded by Zanjan University of Medical Sciences, Zanjan, Iran.
Research Highlights
What is the current knowledge?
What is new here?
-
Aromatherapy with the aroma of Citrus aurantium was effective in reducing postoperative pain.
-
To improve postoperative pain management, aromatherapy with Citrus aurantium can be used along with drug treatments after orthopedic surgery.
References
- Eshete MT, Baeumler PI, Siebeck M, Tesfaye M, Wonde D, Haileamlak A. The views of patients, healthcare professionals and hospital officials on barriers to and facilitators of quality pain management in Ethiopian hospitals: a qualitative study. PLoS One 2019; 14(3):e0213644. doi: 10.1371/journal.pone.0213644 [Crossref] [ Google Scholar]
- Baratta JL, Schwenk ES, Viscusi ER. Clinical consequences of inadequate pain relief: barriers to optimal pain management. Plast Reconstr Surg 2014; 134(4 Suppl 2):15S-21S. doi: 10.1097/prs.0000000000000681 [Crossref] [ Google Scholar]
- Ledowski T, Reimer M, Chavez V, Kapoor V, Wenk M. Effects of acute postoperative pain on catecholamine plasma levels, hemodynamic parameters, and cardiac autonomic control. Pain 2012; 153(4):759-64. doi: 10.1016/j.pain.2011.11.002 [Crossref] [ Google Scholar]
- Garimella V, Cellini C. Postoperative pain control. Clin Colon Rectal Surg 2013; 26(3):191-6. doi: 10.1055/s-0033-1351138 [Crossref] [ Google Scholar]
- Gan TJ. Poorly controlled postoperative pain: prevalence, consequences, and prevention. J Pain Res 2017; 10:2287-98. doi: 10.2147/jpr.s144066 [Crossref] [ Google Scholar]
- Gan TJ, Habib AS, Miller TE, White W, Apfelbaum JL. Incidence, patient satisfaction, and perceptions of post-surgical pain: results from a US national survey. Curr Med Res Opin 2014; 30(1):149-60. doi: 10.1185/03007995.2013.860019 [Crossref] [ Google Scholar]
- Ndebea AS, van den Heuvel SAS, Temu R, Kaino MM, van Boekel RLM, Steegers MAH. Prevalence and risk factors for acute postoperative pain after elective orthopedic and general surgery at a tertiary referral hospital in Tanzania. J Pain Res 2020; 13:3005-11. doi: 10.2147/jpr.s258954 [Crossref] [ Google Scholar]
- Singh PK, Saikia P, Lahakar M. Prevalence of acute post-operative pain in patients in adult age-group undergoing inpatient abdominal surgery and correlation of intensity of pain and satisfaction with analgesic management: a cross-sectional single institute-based study. Indian J Anaesth 2016; 60(10):737-43. doi: 10.4103/0019-5049.191686 [Crossref] [ Google Scholar]
- Hadavi M, Hosseinkhani Z, Saghafi Z. Patient satisfaction from postoperative pain relief in Ali-Ebne-Abitaleb hospital in Rafsanjan - 2012. Community Health Journal 2017; 7(1): 1-8. [Persian].
- Maheshwari AV, Blum YC, Shekhar L, Ranawat AS, Ranawat CS. Multimodal pain management after total hip and knee arthroplasty at the Ranawat Orthopaedic Center. Clin Orthop Relat Res 2009; 467(6):1418-23. doi: 10.1007/s11999-009-0728-7 [Crossref] [ Google Scholar]
- Jacobs CA, Christensen CP. Factors influencing patient satisfaction two to five years after primary total knee arthroplasty. J Arthroplasty 2014; 29(6):1189-91. doi: 10.1016/j.arth.2014.01.008 [Crossref] [ Google Scholar]
- Kolivand P, Ali Hakami M, Eghbali F, Monjamed Z, Sharifi F. Patient satisfaction of the quality of patient teaching in Khatam Alanbia hospital. Neurosci J Shefaye Khatam 2015; 3(3):25-31. doi: 10.18869/acadpub.shefa.3.3.25 [Crossref] [ Google Scholar]
- Berry PH, Dahl JL. The new JCAHO pain standards: implications for pain management nurses. Pain Manag Nurs 2000; 1(1):3-12. doi: 10.1053/jpmn.2000.5833 [Crossref] [ Google Scholar]
- Gupta A, Kaur K, Sharma S, Goyal S, Arora S, Murthy RS. Clinical aspects of acute post-operative pain management & its assessment. J Adv Pharm Technol Res 2010; 1(2):97-108. [ Google Scholar]
- Woldehaimanot TE, Eshetie TC, Kerie MW. Postoperative pain management among surgically treated patients in an Ethiopian hospital. PLoS One 2014; 9(7):e102835. doi: 10.1371/journal.pone.0102835 [Crossref] [ Google Scholar]
- Wiffen PJ, Wee B, Moore RA. Oral morphine for cancer pain. Cochrane Database Syst Rev 2016; 4(4):CD003868. doi: 10.1002/14651858.CD003868.pub4 [Crossref] [ Google Scholar]
- Baldini A, Von Korff M, Lin EH. A review of potential adverse effects of long-term opioid therapy: a practitioner’s guide. Prim Care Companion CNS Disord 2012; 14(3): PCC.11m01326. 10.4088/PCC.11m01326
- Negro S, Martín A, Azuara L, Sánchez Y, Barcia E. Compatibility and stability of ternary admixtures of tramadol, haloperidol, and hyoscine N-butyl bromide: retrospective clinical evaluation. J Palliat Med 2010; 13(3):273-7. doi: 10.1089/jpm.2009.0187 [Crossref] [ Google Scholar]
- Overdyk FJ. Postoperative opioids remain a serious patient safety threat. Anesthesiology 2010; 113(1):259-60. doi: 10.1097/ALN.0b013e3181e2c1d9 [Crossref] [ Google Scholar]
- Dusek JA, Griffin KH, Finch MD, Rivard RL, Watson D. Cost savings from reducing pain through the delivery of integrative medicine program to hospitalized patients. J Altern Complement Med 2018; 24(6):557-63. doi: 10.1089/acm.2017.0203 [Crossref] [ Google Scholar]
- Ganesan P, Manjini KJ, Bathala Vedagiri SC. Effect of music on pain, anxiety and physiological parameters among postoperative sternotomy patients: a randomized controlled trial. J Caring Sci 2022; 11(3):139-47. doi: 10.34172/jcs.2022.18 [Crossref] [ Google Scholar]
- Khalili E, Molavynejad S, Adineh M, Haghighizadeh MH. The effect of Thai massage on the severity of pain in patients with unstable angina: a randomized controlled clinical trial. J Caring Sci 2023; 12(1):73-8. doi: 10.34172/jcs.2023.30150 [Crossref] [ Google Scholar]
- Sharifipour F, Bakhteh A, Mirmohammad Ali M. Effects of Citrus aurantium aroma on post-cesarean anxiety. Iran J Obstet Gynecol Infertil 2015; 18(169):12-20. doi: 10.22038/ijogi.2015.6131 [Crossref] [ Google Scholar]
- Arjmand GR, Bahraminezhad N, Jafari S, Faghihzadeh S, Lotfinia I, Shimia M. The effect of inhalation of aromatherapy lavender (essential oil) on post-operative discectomy pain J Adv Med Biomed Res 2017; 25(110): 83-93. [Persian].
- Amini A, Bahraminejad N, Jafari S, Kamali K. The effect of aromatherapy with Rosa damascena essence on postoperative pain in inguinal hernia repair: a randomized clinical trial. Nurs Midwifery Stud 2020; 9(3):117-23. doi: 10.4103/nms.nms_103_19 [Crossref] [ Google Scholar]
- Saonere Suryawanshi JA. An overview of Citrus aurantium used in treatment of various diseases. Afr J Plant Sci 2011; 5(7):390-5. [ Google Scholar]
- Suntar I, Khan H, Patel S, Celano R, Rastrelli L. Suntar I, Khan H, Patel S, Celano R, Rastrelli LAn overview on Citrus aurantium L: its functions as food ingredient and therapeutic agent. Oxid Med Cell Longev 2018; 2018:7864269. doi: 10.1155/2018/7864269 [Crossref] [ Google Scholar]
- Abbasnejad, M, Keramat B, Esmaili Mahani, S, Rezaeezade-Roukerd M. Effect of hydro-methanolic extract of sour orange flowers, Citrus aurantium, on pentylentetrazole induced seizure in male rats. J Babol Univ Med Sci 2012; 14(5): 20-8. [Persian].
- Cheraghi J, Valadi A. Effects of anti-nociceptive and anti-inflammatory component of limonene in herbal drugs. Iran J Med Aromat Plants Res 2010; 26(3):415-22. doi: 10.22092/ijmapr.2010.6803 [Crossref] [ Google Scholar]
- Bent S, Padula A, Neuhaus J. Safety and efficacy of Citrus aurantium for weight loss. Am J Cardiol 2004; 94(10):1359-61. doi: 10.1016/j.amjcard.2004.07.137 [Crossref] [ Google Scholar]
- Namazi M, Amiraliakbari S, Mojab F, Talebi A, Alavi Majd H, Jannesari S. Investigating the effect of Citrus aurantium aroma on severity of labor pain during active phase of labor. Complementary Medicine Journal 2014; 4(1): 733-44. [Persian].
- Chen L, Xie T. Effect of Citrus aurantium on pain intensity and blood pressure in gastrectomy. Indian J Pharm Sci 2022; 84(2):174-79. doi: 10.36468/pharmaceutical-sciences.spl.471 [Crossref] [ Google Scholar]
- Olapour A, Behaeen K, Akhondzadeh R, Soltani F, Razavi FA, Bekhradi R. The effect of inhalation of aromatherapy blend containing lavender essential oil on cesarean postoperative pain. Anesth Pain Med 2013; 3(1):203-7. doi: 10.5812/aapm.9570 [Crossref] [ Google Scholar]
- Sharifipour F, Mirmohammad Ali M, Hashemzadeh M. Comparison of the effect of Citrus aurantium and Salvia officinalis aroma on post-cesarean section pain. Iran J Obstet Gynecol Infertil 2017; 20(2):41-9. doi: 10.22038/ijogi.2017.8713 [Crossref] [ Google Scholar]
- Mudgalkar N, Bele SD, Valsangkar S, Bodhare TN, Gorre M. Utility of numerical and visual analog scales for evaluating the post-operative pain in rural patients. Indian J Anaesth 2012; 56(6):553-7. doi: 10.4103/0019-5049.104573 [Crossref] [ Google Scholar]
- Fadaizadeh L, Emami H, Samii K. Comparison of visual analogue scale and faces rating scale in measuring acute postoperative pain. Arch Iran Med 2009; 12(1):73-5. [ Google Scholar]
- Yip YB, Tam AC. An experimental study on the effectiveness of massage with aromatic ginger and orange essential oil for moderate-to-severe knee pain among the elderly in Hong Kong. Complement Ther Med 2008; 16(3):131-8. doi: 10.1016/j.ctim.2007.12.003 [Crossref] [ Google Scholar]
- Younger J, McCue R, Mackey S. Pain outcomes: a brief review of instruments and techniques. Curr Pain Headache Rep 2009; 13(1):39-43. doi: 10.1007/s11916-009-0009-x [Crossref] [ Google Scholar]