Journal of caring sciences. 12(1):73-78.
doi: 10.34172/jcs.2023.30150
Original Article
The Effect of Thai Massage on the Severity of Pain in Patients with Unstable Angina: A Randomized Controlled Clinical Trial
Elahe Khalili Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Validation, Visualization, Writing – original draft, Writing – review & editing, 1 
Shahram Molavynejad Conceptualization, Funding acquisition, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing, 1, *
Mohammad Adineh Conceptualization, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing, 1
Mohammad Hosein Haghighizadeh Conceptualization, Data curation, Formal analysis, Methodology, Project administration, Validation, Visualization, Writing – original draft, Writing – review & editing, 2
Author information:
1Nursing Care Research Center in Chronic Diseases, School of Nursing and Midwifery, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
2Department of Biostatistics, School of Health, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
Abstract
Introduction: Chest pain is an unpleasant and the most common symptom in patients suffering from unstable angina. This study was implemented to investigate the effect of Thai massage on severity of pain in patients with unstable angina.
Methods: This study was a randomized controlled clinical trial that carried out on 70 patients with unstable angina who had been hospitalized in hospital affiliated to Ahvaz Jundishapur University of Medical sciences, Ahvaz, Iran. The participants were allocated randomly to either the intervention (n=35) or control group (n=35) between August 1, 2016 and April 30, 2017. The patients in the intervention group received routine care beside and Thai massage with the duration of 30 minutes in two consecutive days. The patients in the control group received routine care. The intensity of pain was assessed by using the numeric rating scale, five minutes before and immediately, 15, 30 and 60 minutes after the intervention. The independent t-test and repeated measures analysis of variance (ANOVA) were used to analysis data through SPSS 13.
Results: After the intervention, the severity of pain was significantly diminished by about four measurement points (P=0.001) with the linear pattern of pain reduction. Nonetheless, in the control group, no statistically significant difference in the intensity of pain was found.
Conclusion: This study showed that Thai massage as non-invasive approach, concomitant with standard nursing care, has the potential to decrease chest pain. Nurses should be taught about pain relief methods for improving the quality of patient care.
Keywords: Thai massage, Pain, Unstable angina, Cardiovascular diseases
Copyright and License Information
© 2023 The Author(s).
This work is published by Journal of Caring Sciences as an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/). Non-commercial uses of the work are permitted, provided the original work is properly cited
Introduction
Cardiovascular diseases as the leading cause of death across the world are responsible for 16 million death per year.1 Unstable angina is a subset of acute coronary syndrome.2 Chest pain is unpleasant and the most common symptom in patients suffering from unstable angina admitted to the cardiac care unit (CCU).3 Pain can cause physical dysfunctions, changes in the blood pressure, pulse rate, hyper coagulation, and inability to cough and make deep breathing, low oxygen saturation, sleep disturbances, ineffective self-care, immune system disorder and persistent catabolism.4,5
One of the most important duties of nurses is to assess and control pain.6 Effective and appropriate pain management reduces morbidity, speeds up recovery, accelerates discharge from the hospital and improves the quality of life.7 Inappropriate pain management entails physiological, psychological, economic and social consequences for the patient, family and society.8 Also a failure to relief pain reduces the patient confidence to healthcare providers and increases the costs of care.9 Nowadays, pharmacological methods are used for relieving pain among patients with angina pectoris. For instance, morphine as a commonly used drug causes respiratory depression, nausea, vomiting, ileus, longtime hospitalization and additional hospital costs.10 Another medicinal method for the reduction of pain is complementary therapies including massage therapy. Massage therapy is a therapeutic complementary technique that defined as a systematic soft tissues manipulation by rhythmic and mild pressure in order to attainment or preservation the health.11,12 It can offer several neuromuscular, and physiological advantages to the body, including a raise in blood circulation, a decrease in neurological excitability and muscle tension, a reduction in muscle tenderness, an improvement in flexibility, and a boost in well-being.13 It is considered to ease the pain via several pathways, such as enhancing the pain threshold by discharging endorphins and relieving pain at the spinal cord level.12
Massage is an easy, safe, non-invasion and relatively inexpensive nursing intervention.14 Massage effects have been evaluated in divers’ diseases. Massage improved outcomes include reduced pain, fatigue and improved sleep quality15; reduced anxiety16; improved blood pressure and heart rate17,18 and improved lumbago.19 Various massage types, including classic massage (e.g. Swedish massage) and acupressure (e.g. traditional Thai massage), apply distinct approaches and methods.12 Thai massage technique is on the basis of energy balance theory of health and recovery. Deep tissue massage with pressure medicine have accomplished in this method. Thai massage concentrated on energy lines that flowing in body and recognized as sen sib. Palming and thumbing are used to enhance energy currency along the line.12
As far as we are aware, thus far no investigation has taken care of the impact of Thai massage on distress relief in patients with angina pectoris. In addition, lack of knowledge and expertise in the field of complementary medicine, lack of adequate support and time as barriers to the use of complementary medicine in clinical settings.20 Therefore, due to the importance of pain control in patients with angina pectoris, and the role of complementary medicine in healthcare interventions, this study was intended to examine the effect of Thai massage on chest pain in patients with unstable angina.
In Iran, nurses do not usually use complementary medicine in general and massage in particular for their self-care goals.15 One reason for this is the lack of complementary medicine course in their curriculum for bachelor program and they graduated without any awareness about this field of medicine. Also in-service education courses in this scope are poorly established.21 Nurses shortage and their excess workload are another reason that nurses have not adequate time to participate and they merely have paid to routine measures.22 According to these points, increasing nurses’ knowledge in this regard is of paramount importance. If positive effects of massage therapy in cardiac patients can be demonstrated, massage therapy could be included in the nurses’ undergraduate educational curricula so that the newly-graduated nurses are aware of such methods and utilize them at the beginning of their career.
Materials and Methods
This randomized controlled trial was conducted on 84 patients with unstable angina hospitalized in two CCUs of Golestan hospital affiliated with the Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran between August 1, 2016 and April 30, 2017. Golestan Hospital is a referral hospital for patients with cardiovascular diseases. To calculate the sample size, a test power of 90%, sample attrition of 20%, α=0.05 and a confidence interval (CI) of 95% were considered. After screening 118 potential participants, a convenience sample of 84 patients was enrolled in the study. Participants were allocated to an intervention (n=42) and a control (n=42) group through permuted block randomization and a table of random permutations. Block size was 4. During the study, seven participants from the intervention group and seven from the control group left the intervention due to changes in hemodynamic conditions. Finally, 35 participants remained in each group (Figure 1). Randomization was performed by a computer-generated order, hidden in consecutive numbers, locked, with unclear covering, and held by a neutral person in the study.
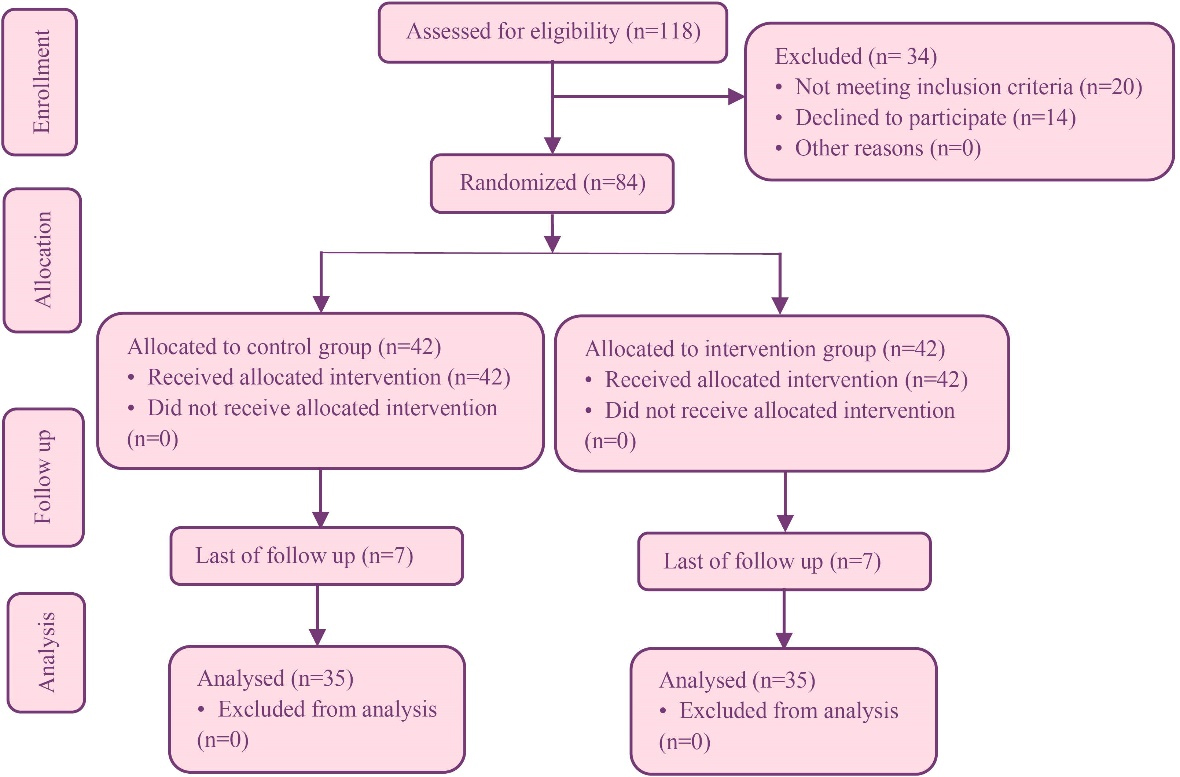
Figure 1.
The flowchart of the study
.
The flowchart of the study
Those patients who met the inclusion criteria were included in this study based on their admission time to CCU. The inclusion criteria were as follow: aged 18-70 years old; the score of pain between 1to 7 based on the Numeric Rating Scale (NRS); being diagnosed with unstable angina; willingness to participate in this study; orientation to time, place and person; not using narcotics in the last four hours; no history of nervous, neurovascular and psychiatric disturbances; having no severe dyspnea, fever and cardiac pacemaker; pulse rate above 60 beat per min; having no mental disorders, amputation in limbs infectious diseases and coagulation disorders. The reduction of consciousness level and instability in hemodynamic status were considered exclusion criteria.
The patients (both intervention and control group) received their regular treatments. In the intervention group, massage therapy was performed by two nurses who received the required professional training for 4 months under the supervision of a massage specialist and acquired a related certificate. They conducted the massage therapy intervention with study participants under the supervision of a cardiology specialist. The setting of the location of the Thai massage was a single room with low light, appropriate temperature, and no environmental stimulus. Massage therapy was done in 30 minutes in two subsequent days.
There was no conversation during the intervention. Massage was performed on the patients’ chest, abdomen, arms and fingers of two hands, palm, femur, legs, feet fingers, metatarsus, back, lumbar section and shoulders. The massage steps were: 1) The goal and term of massage were described to the patient; 2) The confidentiality and safety of the participants were noted i.e. just the investigator and the participant were in the massage chamber; 3) followed by a sitting position on the massage chair and inclination of the head toward the pillow; 4) Prior to the initiation of the massage, the investigator heated her hands by friction. Lubrication of the massage surface with almond oil was performed to inhibit any harm to the case’s skin; 5) The classical Thai Massage technique was composed of various movements, including applying pressure and stroke (effleurage), knead (petrissage), massaging with quick strokes, knocking (percussion), and massaging with high strokes (friction) on a couple of lines on the right side of participants, named Pingkhala and on a couple of lines on the left side of participants named Ittha. The application of pressure used in traditional Thai massage (TTM) employs the body mass of the massage therapist to use soft, progressively raising pressure via the therapist’s fingers, thumb or palm.23
The severity of pain was measured and recorded immediately, 5 minutes, 30 minutes and 60 minutes after massage. The patients in the control group were in their own multiple bed room. In addition, throughout the intervention period, a nurse massage therapist remained with the patients in the control group, to keep their status and to take good care of them (social attention) and support them to convey their concerns and impressions regarding hospitalization. The examiner who gathered output data was obscured to the group task.
The data collection tool was consisted of a demographic data form with questions about the patients’ age, gender, the marital status, nationality and level of education. Also, the NRS was used for measuring the severity of pain. The NRS relies on the patient self-report. “No pain” and “the worst possible pain” were equivalent to the scores of 0 and 10. The scores of 1-3 indicated mild pain, 4-6 moderate pain, 7-9 severe pain and 10 represented intolerable pain.24 In this study, the reliability of this tool (Cronbach’s α) was 0.90. Also, a demographic characteristics and disease-related data form were used for data collection.
Descriptive and inferential statistics were used for data analysis via the SPSS software v. 21 for windows. The independent t test and repeated measures analysis of variance (ANOVA) were used to compare the groups. P<0.05 was considered statistically significant.
Results
The final samples were consisted of 35 male (50%) and 35 female (50%) patients. The mean (SD) age of the patients in the intervention and control groups was 59.28 (7.11) and 60.25 (7.52) years. The patients in the intervention and control group had the elementary education level (40% and 31.4%, respectively). Before the intervention, no statistically significant differences were observed between the two groups in terms of the demographic characteristics such as age, gender, the level of education and marital status (Table 1).
Table 1.
Demographic characteristics between groups
|
Variable
|
Control group (n=35)
|
Intervention group (n=35)
|
P
value
a
|
|
No. (%)
|
No. (%)
|
| Gender |
| Male |
17 (48.6) |
18 (51.4) |
0.81 |
| Female |
18 (51.4) |
17 (48.6) |
| Age (year) |
| 30-50 |
7 (20) |
9 (25.8) |
0.78 |
| 50-70 |
28 (80) |
26 (74.2) |
| Marital status |
| Single |
2 (5.8) |
0 (0) |
0.75 |
| Married |
33 (94.2) |
35 (100) |
| Education |
| Illiterate |
14 (40) |
7 (20) |
0.46 |
| Elementary |
11 (31.4) |
14 (40) |
| Middle school |
2 (5.7) |
4 (11.5) |
| High school |
8 (22.9) |
10 (28.5) |
| Ethnicity |
| Lore |
13 (37.1) |
13 (37.1) |
0.60 |
| Arab |
14 (40) |
18 (51.4) |
| Fars |
6 (17.1) |
3 (8.6) |
| Others |
2 (5.7) |
1 (2.9) |
The patients in the intervention and control groups were Arab (51.4% and 40%, respectively).
The results of the repeated measure ANOVA test showed statistically significant reductions in the mean score of intensity of pain in the intervention group immediately, 15, 30 and 60 minutes after the intervention compared with before the intervention (P = 0.001). On the other hand, no statistically significant differences were observed in the mean score of intensity of pain in the control group before the intervention (Tables 2 and 3). The intensity of pain at different times was different between the intervention and control groups indicating the effectiveness of massage therapy. Also, the patients in the intervention group on the second day experienced less pain (Table 3).
Table 2.
The comparison of the intensity of pain between the groups in the first day
|
Groups
|
Control groups (n=35)
|
Intervention groups (n=35)
|
|
Mean (SD)
|
Mean (SD)
|
| 5 Minutes before the intervention |
5.17 (1.65) |
5.68 (1.18) |
| Immediately after the intervention |
5.37 (1.61) |
4.34 (1.28) |
| 15 Minutes after the intervention |
5.34 (1.62) |
4.20 (1.36) |
| 30 Minutes after the intervention |
5.42 (1.48) |
3.71 (1.38) |
| 60 Minutes after the intervention |
5.51 (1.44) |
3.25 (1.24) |
|
P
|
0.001b |
0.34a |
aChi-squared test, bRepeated-measures analysis of variance.
Table 3.
The comparison of the intensity of pain in the groups in the second day
|
Groups
|
Intervention groups (n=35)
|
Control groups (n=35)
|
|
Mean (SD)
|
Mean (SD)
|
| 5 Minutes before the intervention |
2.17(0.74) |
3.54(1.29) |
| Immediately after the intervention |
1.28(0.75) |
3.71(1.31) |
| 15 Minutes after the intervention |
1(0.68) |
3.57(1.35) |
| 30 Minutes after the intervention |
0.71(0.78) |
3.57(1.33) |
| 60 Minutes after the intervention |
0.56(0.65) |
3.48(1.37) |
|
P
|
0.11a |
0.00b |
aChi-squared test, bRepeated-measures analysis of variance.
Discussion
It was found that Thai massage reduced chest pain in patients with unstable angina. A few studies examined the effects of massage on chest pain in patients with angina pectoris. Due to lake of studies on the effects of massage on patients with angina pectoris, we had to compare our results with those of studies conducted on patients with other disease. Najafi et al studied the effect of Thai massage on pain after coronary artery bypass surgery and found that massage reduced pain after the surgery.25 Cutshall et al studied the effect of massage on pain, anxiety and stress in patients after the cardiac surgery. The patients received 20 minutes massage in the second to the fifth day after the surgery. They found that massage was a safe method and reduced patients’ pain, anxiety and stress.26 Dion et al in a study on the effect of massage on pain management in thoracic surgery patients reported the positive effects of massage on pain management.27 Han and Lee studied the effect of massage on patients’ pain after the gastrostomy surgery and found a significant reduction in their pain.28 Field et al studied the effect of massage on hand pain, which resulted in the reduction of pain.29 Babajani et al found that reflex massage reduced foot pain during the pulling of chest tube after the open heart surgery. The anterior part of patients’ right feet was given deep massage by two thumbs for ten minutes without causing uncomfortable feelings. It also showed a reduction in pain after massage therapy.30 Anderson and Downey studied the effect of foot reflexology massage on pain for inpatients with cancer and found that foot reflexology massage reduced pain.31 Miladinia et al showed that massage ameliorated the symptoms of adult patients with acute leukemia, in a survey with the goal of examining the impact of quick stroke back massage on symptom collection.15
Nurse’s knowledge of pain and pain relief has significant effects on the reduction of patients’ intensity of pain. Also nurse act as educators to the patient and family about how to use palliative treatment methods at home.32 It is suggested that massage therapy is educated to nursing students with the aim of improving the quality of patients’ life during hospitalization. It can also improve patients’ satisfaction by improving their life quality and reduce re-admission rates. A few studies examined the effect of massage on pain in cardiac patients. A pain management program is needed to be designed for relieving patients’ pain with the less use of sedative drugs, reducing the length of stay in the hospital and treatment costs.33 It is crucial to keep in mind to stay open-minded regarding diversity in ideology, and concerning what the issue is and the root causes. Rectifying a client or patient’s diverse ideology concerning their status may result in withholding prospective opinions and intervening with the development of mutual trust. Taking care of patients respectfully and permitting them to directly speak about disparities in health opinion allows them to disclose their health record and indications so that you can contribute to the precise treatment plan and they willingly follow your guidance.34
Cultural factors influence beliefs, behaviour, perceptions and emotions, all of which have important implications on health and health care. Knowledge of a patient’s culture may provide valuable information regarding likely beliefs about the cause(s) of and coping mechanisms for pain, both of which will inform the management and or prognosis.35
As the limitations of this study, the limited number of the sample size and conducting the intervention in one hospital may impact the generalizability of our findings.
Conclusion
The findings of this study suggest that applying massage therapy intervention is effective in mitigating pain in patients with unstable angina. Future research is required to test the impacts of massage on pain severity using a larger sample size.
Acknowledgments
This article is the result of the MSc thesis by the first author (EK), which is financially supported by Ahvaz Jundishapur University of Medical Sciences (CDCRC-9414). We sincerely acknowledge the authorities of Ahvaz University of Medical Sciences, nurses, patients and their families who helped to conduct this study.
Authors’ Contribution
Conceptualization: Elahe Khalili, Shahram Molavynejad, Mohammad Adineh, Mohammad Hosein Haghighizadeh.
Data curation: Elahe Khalili.
Formal Analysis: Elahe Khalili, Mohammad Hosein Haghighizadeh.
Funding acquisition: Shahram Molavynejad.
Investigation: Elahe Khalili.
Methodology: Elahe Khalili, Shahram Molavynejad, Mohammad Adineh, Mohammad Hosein Haghighizadeh.
Project administration: Shahram Molavynejad, Mohammad Adineh.
Software: Mohammad Hosein Haghighizadeh.
Supervision: Shahram Molavynejad, Mohammad Adineh.
Validation: Elahe Khalili, Shahram Molavynejad, Mohammad Adineh, Mohammad Hosein Haghighizadeh.
Visualization: Elahe Khalili, Shahram Molavynejad, Mohammad Adineh, Mohammad Hosein Haghighizadeh.
Writing – original draft: Elahe Khalili, Shahram Molavynejad, Mohammad Adineh, Mohammad Hosein Haghighizadeh.
Writing – review & editi: Elahe Khalili, Shahram Molavynejad, Mohammad Adineh, Mohammad Hosein Haghighizadeh.
COI-statement
The authors declare no conflicts of interest.
Data Accessibility
The datasets are available from the corresponding author on reasonable request.
Ethical Approval
This study was approved by the ethics committee of the Ahvaz Jundishapour University of Medical Sciences, Iran (decree code: IR.AJUMS.REC.1394.713). Study goals were described to patients, and they were free to raise any questions. Patients’ hazards and rights were also elucidated. Written consent with full knowledge was acquired from all patients. Massages on female and male cases were done by a gender-matched investigator. This study was registered in the website of Registry of Clinical Trials with the following code: IRCT2016060728314N1.
Funding
This study was funded by Ahvaz Jundishapour University of Medical Sciences, Iran.
Research Highlights
What is the current knowledge?
In many countries, massage has presently been applied as an easy tool to alleviate pain via mental and physical leisure.
What is new here?
The present study demonstrated that the Thai massage is a quite affordable tool that can be easily integrated into the support plans of cases with unstable angina at the hospital.
References
- Grey C, Jackson R, Schmidt M, Ezzati M, Asaria P, Exeter DJ. One in four major ischaemic heart disease events are fatal and 60% are pre-hospital deaths: a national data-linkage study (ANZACS-QI 8). Eur Heart J 2017; 38(3):172-80. doi: 10.1093/eurheartj/ehv524 [Crossref] [ Google Scholar]
- Silva FM, Pesaro AE, Franken M, Wajngarten M. Acute management of unstable angina and non-ST segment elevation myocardial infarction. Einstein (Sao Paulo) 2015; 13(3):454-61. doi: 10.1590/s1679-45082015rw3172 [Crossref] [ Google Scholar]
- Prachanukool T, Aramvanitch K, Sawanyawisuth K, Sitthichanbuncha Y. Acute chest pain fast track at the emergency department: who was misdiagnosed for acute coronary syndrome? Open Access Emerg Med 2016; 8: 111-6. who was misdiagnosed for acute coronary syndrome? Open Access Emerg Med 2016; 8:who was misdiagnosed for acute coronary syndrome? Open Access Emerg Med 2016; 8. doi: 10.2147/oaem.s112903 [Crossref] [ Google Scholar]
- Alcántara C, Peacock J, Davidson KW, Hiti D, Edmondson D. The association of short sleep after acute coronary syndrome with recurrent cardiac events and mortality. Int J Cardiol 2014; 171(2):e11-2. doi: 10.1016/j.ijcard.2013.11.135 [Crossref] [ Google Scholar]
- Chanques G, Jaber S, Barbotte E, Violet S, Sebbane M, Perrigault PF. Impact of systematic evaluation of pain and agitation in an intensive care unit. Crit Care Med 2006; 34(6):1691-9. doi: 10.1097/01.ccm.0000218416.62457.56 [Crossref] [ Google Scholar]
- Cano Romero MD, Muñoz Sastre MT, Quintard B, Sorum PC, Mullet E. The ethics of postoperative pain management: Mapping nurses’ views. Int J Nurs Pract 2017; 23(2):e12514. doi: 10.1111/ijn.12514 [Crossref] [ Google Scholar]
- Dong W, An B, Wang Y, Cui X, Gan J. Effect of multimodal analgesia on gynecological cancer patients after radical resection. Am J Transl Res 2021; 13(4):2686-93. [ Google Scholar]
- Brennan F, Carr DB, Cousins M. Pain management: a fundamental human right. Anesth Analg 2007; 105(1):205-21. doi: 10.1213/01.ane.0000268145.52345.55 [Crossref] [ Google Scholar]
- Ben-Yehuda O, Kazi DS, Bonafede M, Wade SW, Machacz SF, Stephens LA. Angina and associated healthcare costs following percutaneous coronary intervention: a real-world analysis from a multi-payer database. Catheter Cardiovasc Interv 2016; 88(7):1017-24. doi: 10.1002/ccd.26365 [Crossref] [ Google Scholar]
- Chandrababu R, Nayak BS, Pai VB, N R, George LS, Devi ES. Effects of foot massage and patient education in patients undergoing coronary artery bypass graft surgery: a randomized controlled trial. Complement Ther Clin Pract 2020; 40:101215. doi: 10.1016/j.ctcp.2020.101215 [Crossref] [ Google Scholar]
- Karagozoglu S, Kahve E. Effects of back massage on chemotherapy-related fatigue and anxiety: supportive care and therapeutic touch in cancer nursing. Appl Nurs Res 2013; 26(4):210-7. doi: 10.1016/j.apnr.2013.07.002 [Crossref] [ Google Scholar]
- Netchanok S, Wendy M, Marie C, Siobhan O. The effectiveness of Swedish massage and traditional Thai massage in treating chronic low back pain: a review of the literature. Complement Ther Clin Pract 2012; 18(4):227-34. doi: 10.1016/j.ctcp.2012.07.001 [Crossref] [ Google Scholar]
- Hongsuwan C, Eungpinichpong W, Chatchawan U, Yamauchi J. Effects of Thai massage on physical fitness in soccer players. J Phys Ther Sci 2015; 27(2):505-8. doi: 10.1589/jpts.27.505 [Crossref] [ Google Scholar]
- Essner B, Hajduk J, Lavigne J, Krodel D, Shah R, Svigos F. Effectiveness of massage therapy consultation for pediatric chronic pain. J Pain 2016; 17(4):S113. doi: 10.1016/j.jpain.2016.01.463 [Crossref] [ Google Scholar]
- Miladinia M, Baraz S, Shariati A, Malehi AS. Effects of slow-stroke back massage on symptom cluster in adult patients with acute leukemia: supportive care in cancer nursing. Cancer Nurs 2017; 40(1):31-8. doi: 10.1097/ncc.0000000000000353 [Crossref] [ Google Scholar]
- Dunn C, Sleep J, Collett D. Sensing an improvement: an experimental study to evaluate the use of aromatherapy, massage and periods of rest in an intensive care unit. J Adv Nurs 1995; 21(1):34-40. doi: 10.1046/j.1365-2648.1995.21010034.x [Crossref] [ Google Scholar]
- Albert NM, Gillinov AM, Lytle BW, Feng J, Cwynar R, Blackstone EH. A randomized trial of massage therapy after heart surgery. Heart Lung 2009; 38(6):480-90. doi: 10.1016/j.hrtlng.2009.03.001 [Crossref] [ Google Scholar]
- Kim IH, Kim TY, Ko YW. The effect of a scalp massage on stress hormone, blood pressure, and heart rate of healthy female. J Phys Ther Sci 2016; 28(10):2703-7. doi: 10.1589/jpts.28.2703 [Crossref] [ Google Scholar]
- Kumar S, Rampp T, Kessler C, Jeitler M, Dobos GJ, Lüdtke R. Effectiveness of Ayurvedic massage (Sahacharadi taila) in patients with chronic low back pain: a randomized controlled trial. J Altern Complement Med 2017; 23(2):109-15. doi: 10.1089/acm.2015.0272 [Crossref] [ Google Scholar]
- Leach MJ, Gillham D. Are complementary medicine practitioners implementing evidence based practice? Complement Ther Med 2011; 19(3): 128-36. Are complementary medicine practitioners implementing evidence based practice? Complement Ther Med 2011; 19(3):128-36. doi: 10.1016/j.ctim.2011.04.002 [Crossref] [ Google Scholar]
- Miladinia M, Baraz S, Zarea K, Mousavi Nouri E. Massage therapy in patients with cancer pain: a review on palliative care. Jundishapur J Chronic Dis Care 2017; 6(1):e37356. doi: 10.17795/jjcdc-37356 [Crossref] [ Google Scholar]
- Adib Hajbaghery M, Salsali M. A model for empowerment of nursing in Iran. BMC Health Serv Res 2005; 5(1):24. doi: 10.1186/1472-6963-5-24 [Crossref] [ Google Scholar]
- Buttagat V, Eungpinichpong W, Chatchawan U, Kharmwan S. The immediate effects of traditional Thai massage on heart rate variability and stress-related parameters in patients with back pain associated with myofascial trigger points. J Bodyw Mov Ther 2011; 15(1):15-23. doi: 10.1016/j.jbmt.2009.06.005 [Crossref] [ Google Scholar]
- Kwekkeboom KL, Abbott-Anderson K, Cherwin C, Roiland R, Serlin RC, Ward SE. Pilot randomized controlled trial of a patient-controlled cognitive-behavioral intervention for the pain, fatigue, and sleep disturbance symptom cluster in cancer. J Pain Symptom Manage 2012; 44(6):810-22. doi: 10.1016/j.jpainsymman.2011.12.281 [Crossref] [ Google Scholar]
- Najafi SS, Rast F, Momennasab M, Ghazinoor M, Dehghanrad F, Mousavizadeh SA. The effect of massage therapy by patients’ companions on severity of pain in the patients undergoing post coronary artery bypass graft surgery: a single-blind randomized clinical trial. Int J Community Based Nurs Midwifery 2014; 2(3):128-35. [ Google Scholar]
- Cutshall SM, Wentworth LJ, Engen D, Sundt TM, Kelly RF, Bauer BA. Effect of massage therapy on pain, anxiety, and tension in cardiac surgical patients: a pilot study. Complement Ther Clin Pract 2010; 16(2):92-5. doi: 10.1016/j.ctcp.2009.10.006 [Crossref] [ Google Scholar]
- Dion L, Rodgers N, Cutshall SM, Cordes ME, Bauer B, Cassivi SD. Effect of massage on pain management for thoracic surgery patients. Int J Ther Massage Bodywork 2011; 4(2):2-6. doi: 10.3822/ijtmb.v4i2.100 [Crossref] [ Google Scholar]
- Han MS, Lee KY. The effect of back massage on degree of pain, state anxiety and quality of sleep of postoperative patients with gastrectomy. Asian Oncol Nurs 2012; 12(1):69-76. doi: 10.5388/aon.2012.12.1.69 [Crossref] [ Google Scholar]
- Field T, Diego M, Delgado J, Garcia D, Funk CG. Hand pain is reduced by massage therapy. Complement Ther Clin Pract 2011; 17(4):226-9. doi: 10.1016/j.ctcp.2011.02.006 [Crossref] [ Google Scholar]
- Babajani S, Babatabar Darzi H, Ebadi A, Mahmoudi H, Nasiri E. The effect of foot reflexology massage on the level of pain during chest tube removal after open heart surgery. Iran J Crit Care Nurs 2014; 7(1):15-22. [ Google Scholar]
- Anderson KD, Downey M. Foot reflexology: an intervention for pain and nausea among inpatients with cancer. Clin J Oncol Nurs 2021; 25(5):539-45. doi: 10.1188/21.cjon.539-545 [Crossref] [ Google Scholar]
- Musavi M, Jahani S, Asadizaker M, Maraghi E, Razmjoo S. The effect of pain self-management education on pain severity and quality of life in metastatic cancer patients. Asia Pac J Oncol Nurs 2021; 8(4):419-26. doi: 10.4103/apjon.apjon-2097 [Crossref] [ Google Scholar]
- Zare M, Kalroozi F, Nezamzadeh M, Zareiyan A. Comparison of the effect of using back massage with hand and warm towel on muscle pain and pulmonary function of patients undergoing open heart surgery hospitalized in selected military hospital in Shiraz. Mil Caring Sci 2021; 8(3): 274-87. [Persian].
- Hasnain-Wynia R, Baker DW. Obtaining data on patient race, ethnicity, and primary language in health care organizations: current challenges and proposed solutions. Health Serv Res 2006; 41(4 Pt 1):1501-18. doi: 10.1111/j.1475-6773.2006.00552.x [Crossref] [ Google Scholar]
- Sharma S, Abbott JH, Jensen MP. Why clinicians should consider the role of culture in chronic pain. Braz J Phys Ther 2018; 22(5):345-6. doi: 10.1016/j.bjpt.2018.07.002 [Crossref] [ Google Scholar]