Journal of caring sciences. 12(2):94-102.
doi: 10.34172/jcs.2023.30726
Review Article
Psychosocial Interventions by Nurses for Patients with HIV/ AIDS: A Systematic Review
Malihe Davoudi Conceptualization, Data curation, Formal analysis, Methodology, Writing – original draft, 1 
Abbas Heydari Conceptualization, Funding acquisition, Methodology, Project administration, Supervision, Writing – review & editing, 2
Zahra Sadat Manzari Conceptualization, Formal analysis, Methodology, Supervision, Writing – review & editing, 2, *
Author information:
1Student Research Committee, School of Nursing and Midwifery, Mashhad University of Medical Sciences, Mashhad, Iran
2Department of Medical-Surgical Nursing, School of Nursing and Midwifery, Mashhad University of Medical Sciences, Mashhad, Iran
Abstract
Introduction:
Providing psychological support is one of the traditional roles of nurses for patients with HIV/AIDS. Searching the literature showed that various psychological interventions have been performed by nurses to support HIV/AIDS patients; however, no summary of these interventions is available. We aimed to systematically review the interventional studies which investigated the effectiveness of psychosocial interventions delivered by nurses to HIV/AIDS patients.
Methods:
This systematic review was performed based on Cochrane’s handbook of systematic reviews of interventional studies. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement were used in this study. The databases of PubMed, Web of Science, Cochrane, Scopus and World Health Organization were searched from January 2009 to December 2022. Based on inclusion criteria, nine studies included in this systematic review. Cochrane data extraction form was used for the systematic review and the article’s information was summarized using the modified Jadad scale.
Results:
The interventions provided by the nurses included: virtual and face-to-face educational programs, written information resources, palliative care, motivational interview, case management, home visit, and care services, along with face-to-face and telephone follow-up. These interventions have a significant positive effect on the quality of life and management of high-risk behaviors, disease management, symptoms and complications, adherence to treatment, immune function, and mental health in patients with HIV/AIDS.
Conclusion:
The results of the present study show that despite the fact that the interventions have a purely psychological content and can be done with various methods, they are able to have positive consequences in physical, psychological, behavioral, and laboratory health in HIV/AIDS patients.
Keywords: HIV/AIDS, Nurses, Psychology, Systematic review
Copyright and License Information
© 2023 The Author(s).
This work is published by Journal of Caring Sciences as an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by-nc/4.0/). Non-commercial uses of the work are permitted, provided the original work is properly cited.
Introduction
Despite the ongoing attempts to cure and prevent AIDS/HIV, this disease remains one of the major health challenges worldwide.1 AIDS/HIV affects all aspects of a person’s quality of life, including physical, psychological, social, and spiritual aspects.2Patients with HIV/AIDS experience significant medically and psychologically suffering.3 There is a two-way and complex relationship between psychological health and the problems of these patients. HIV and associated infections can cause nerve damage.4 On the other hand, psychological health problems can be caused by antiviral treatment or the social stigma, stress, and economic and social consequences associated with treatment process.5 Psychological problems can negatively affect the adherence to antiviral treatment and development of AIDS and consequently poorer health outcomes.6 HIV patients compared to the general population are more likely to develop psychological health disorders such as depression, anxiety, suicide, and drug abuse.7 So, performing psychological interventions is needed.8
Since nurses are more firmly and continuously connected to the patients, they have the main role in the care of patients with AIDS/HIV.9,10 Therefore, their performance may affect the patients’ treatment and satisfaction.11One of the traditional roles and responsibilities of nurses is to provide psychological support. In holistic nursing care, psychological support is essential for healing of patients.12 Psychological support includes any support to help them improve their psychological, cognitive, emotional, and behavioral well-being. Psychological support is provided by a wide range of professional groups, peers, and informal providers, both in the clinical setting and in the community.13 Psychological support helps patients make informed decisions, better cope with disease, and better deal with discrimination. Moreover, psychological support improves the quality of life of patients with HIV and prevents further transmission of HIV infection. Besides, this type of support is important for patients with AIDS/HIV to follow antiretroviral therapy and ongoing counseling to strengthen adherence to treatment regimens.2
Searching the literature showed that various psychological interventions have been performed by nurses to support patients with AIDS/HIV, but no summary of these interventions is available. The implications of these interventions are also unclear. Therefore, this study was performed aimed to review and summarize the psychological interventions provided by nurses to patients with AIDS/HIV. This study increases our knowledge of the psychological interventions which nurses can directly provide to patients with AIDS/HIV. The present study also increases nurses’ awareness of the primary and secondary consequences of these interventions. Moreover, by knowing the possible consequences of each intervention, nurses can choose the appropriate intervention according to the available options and the patients’ preferences. The novelty and innovative aspects of this study is that, to the best of our knowledge, this is the first systematic review which summarizes and highlights the outcomes of psychological interventions performed by nurses on various aspects of the lives of patients with AIDS/HIV. This study also distinguished the types of psychological intervention approaches which are commonly used by nurses. Moreover, the results of psychological interventions were summarized. Our conclusions from the collected data provide positive strategies and new practical evidence for psychological support of patients with AIDS/HIV that can be applied in clinical practice. This review was a comprehensive, detailed, and systematic search of the literature. This study aimed to systematically review the interventional studies which investigated the effectiveness of psychosocial interventions delivered by nurses to patients with HIV/AIDS.
Material and Methods
This systematic review was performed based on Cochrane’s handbook of systematic reviews of interventional studies.14 The PRISMA statement (Preferred Reporting Items for Systematic Reviews and Meta-analysis) was used in this study.15
Search strategy was based on PICO (Participants, intervention, comparison, and outcomes). The participants were patients with HIV/AIDS, the intervention was psychological interventions, comparisons were routine management (i.e., routine care and standard medical care) or no intervention, and outcomes were the effects of the intervention on the physical, psychological, social, and other dimensions of the life of patients with AIDS/HIV. Literature searches were performed in the databases of PubMed, Web of Science, Scopus, Cochrane, and the World Health Organization clinical trials registration system) from 2009 to December 2022. The seminars, conferences,congresses, and journals were more searched. If needed, the researcher contacted the corresponding author for access to the full text of the article. Keywords were based on the mesh that included: Psychological intervention, Mental intervention, Nursing, HIV, AIDS, acquired immune deficiency syndrome, and Human immunodeficiency virus and combination of them using Boolean operators (OR, NOT, AND) (Table 1).
Table 1.
An example of a database search strategy
|
Database
|
Search strategy
|
| Web of science |
Search field; title; search term ("psychological intervention" or "mental intervention") AND ("HIV" OR "AIDS" OR "Human immunodeficiency virus" OR "acquired immune deficiency syndrome")
Limits; restricted to articles, nursing, English, open access |
| PubMed |
Search: ("psychological intervention"[Title/Abstract] OR "mental intervention"[Title/Abstract]) AND nurse*[Title/Abstract] AND (HIV[Title/Abstract] OR AIDS[Title/Abstract] OR "Human immunodeficiency virus"[Title/Abstract] OR "acquired immune deficiency syndrome"[Title/Abstract] ")
Limits: restricted to Randomized Controlled Trial, Controlled Clinical Trial, Clinical Trial, pragmatic Controlled Trial Congress, full text, English |
| Scopus |
Article title, abstract, keyword; ("psychological intervention" OR "mental intervention") AND (HIV OR "Human immunodeficiency virus") OR ("AIDS OR "acquired immune deficiency syndrome")
Limits; nursing, psychology, social science, article, English, open access |
| Cochran |
Title/abstract, keyword: ("psychological intervention" OR "mental intervention") AND nurse AND ("("HIV" OR "AIDS" OR "Human immunodeficiency virus" OR "acquired immune deficiency syndrome")
Limited; trials |
Other citations from the original articles and systematic reviews were also searched and evaluated. After the initial evaluation, duplicate studies were excluded. Then, the abstracts of the articles were reviewed and those which did not coincide with the inclusion criteria were excluded. The full text of the remaining studies was re-evaluated. Finally, nine studies were analyzed (Table 2).
Table 2.
Characteristics of included studies
Author (year),
Country
|
Total sample size
|
Type of intervention in the experimental group
|
Type of intervention in the control group
|
Finding
|
|
|
|
Details
|
Duration of intervention
|
Blank et al16 (2011),
USA |
238 |
Providing counseling and coordination of home and mental health services |
12 months |
Routine care |
Significant reduction in viral load |
Blank et al17 (2014),
USA |
238 |
Home care services and coordination between services |
12 months |
Routine care |
|
Côté et al18 (2015),
Canada |
179 |
Virtual training and follow-up (motivational skills, emotion recognition, and management skills, problem solving, and communication with others) |
8 weeks (4 sessions of 20-30 minutes) |
In-person counseling (providing a list of drug-related websites and side effects) |
-
Improve adherence to treatment
-
Increase self-efficacy
-
Reducing stress
-
Increasing positive attitude
-
Average increase in the level of social support
-
Reducing the discomfort associated with the symptoms of the disease
|
Eller et al19 (2013),
South Africa |
222 |
Symptom management training with practical training |
A 30-minute session |
Nutrition and supportive care training |
-
Reducing the number of depression symptoms, severity and its effects
-
Positive change in the use of self-care and self-management strategies
|
Hanrahan et al20 (2011)
United States American |
238 |
An advanced nursing care model for face-to-face and telephone case management at home |
12 months |
Routine care |
-
Improvement of symptoms of depression, mental problems
-
Improving the quality of life related to health in the physical dimension
|
Holstad et al21 (2011),
USA |
203 |
Motivational group interview |
8 sessions |
Training sessions (Nutrition and stress control and health complications) |
|
Lowther et al22 (2015),
Africa |
120 |
Palliative care intervention including physical, emotional and spiritual |
6 sessions over 4 months |
Routine care |
-
Reduction of pain (in the dimension of ability to share feelings and feeling valuable in life, feeling relaxed)
-
Reducing psychological complications
-
Reduce worries
-
Enhancing the family's ability to plan for the future
-
Increasing the quality of life in the mental dimension
-
Increasing the quality of life in the physical dimension
|
Madhombiro23 (2020),
Africa |
235 |
Motivational Interviewing blended with brief Cognitive Behavioral Therapy |
8 to 10 sessions |
four Enhanced Usual Care sessions based on the alcohol treatment module
from the World Health Organization MH GAP intervention guide) |
|
Nkhoma et al24 (2015),
Southeastern Africa |
182 |
Educational intervention includes face-to-face training, pamphlet presentation, instruction booklet, and telephone follow-up |
A 30-minute session |
Pain medication control training |
-
Decreased pain intensity
-
Better pain management
-
Reducing pain interference with daily life.
-
Increase patient and family knowledge about pain management
-
Increasing the motivation of the family to manage the patient's pain
-
Improving the quality of life
|
Wang et al25 (2010),
China |
116 |
Home visit and telephone contact by a nurse |
8 months |
Routine care |
|
The inclusion criteria were: Original articles with psychological interventions delivered directly by the nurse, English articles published in between 2009 and 2022, randomized clinical trial, experimental or Semi-experimental study, and access to the full-text file. Also, the exclusion criteria were: pilot study, articles published in several sources, articles in the low-quality source, letters to the editor, articles without abstract, studies that were not conducted on patients with HIV/AIDS, and a study in which psychological interventions were not implemented directly by nurses. In this review, all studies have been conducted based on 4 stages of PRISMA (Figure 1).
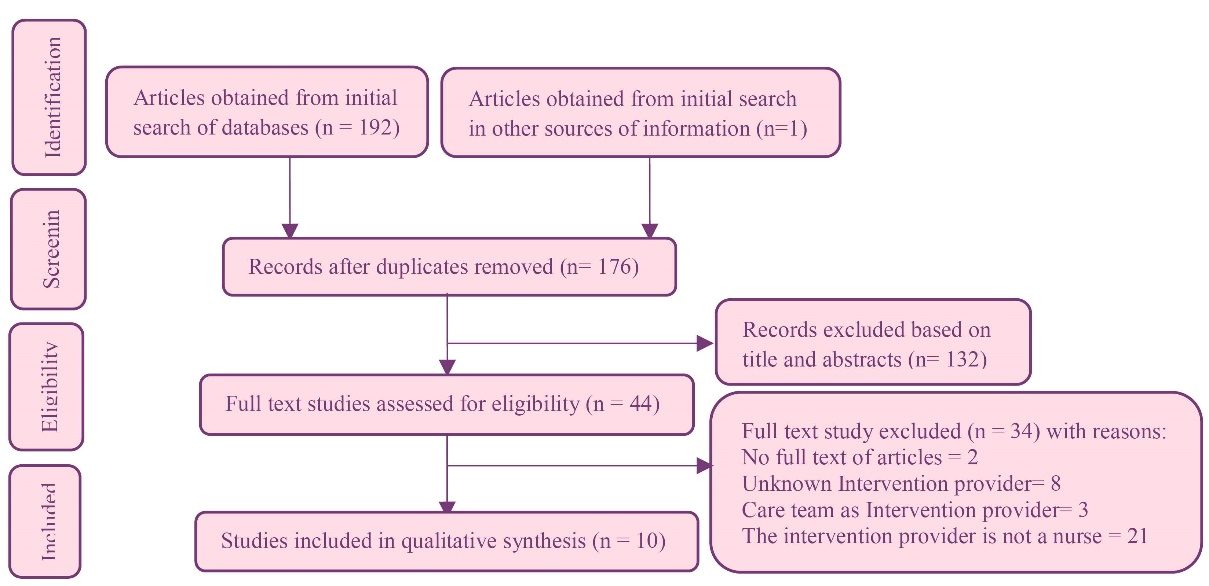
Figure 1.
Preferred reporting items systemic review (PRISMA) flowchart
.
Preferred reporting items systemic review (PRISMA) flowchart
Eight RCTarticles, one semi-experimental and one cluster randomized clinical trial (cRCT) study were found. Four interventions were implemented in the patients’ home and five interventions in health care settings.
Cochrane data extraction form was used. The two authors independently extracted the article information and agreed upon it after discussion. This form included the author’s first name, year of publication, research location, interventional measures and study findings. Initially, several sessions were held to match the rating of the two evaluators. Before the study, the kappa coefficient of agreement between the two evaluators was calculated which was 0.87. In the case of a difference of opinion between the two evaluators, the opinion of third evaluator was used. Two reviewers independently evaluated the quality of the articles and analyzed abstracts and limitations of the studies. Before reviewing the articles, the names of the authors and journals were eliminated. The article information was summarized using the modified JADAD tool. This checklist includes 8 questions assessing different sections of the article. A score of 0 to 4 was considered as weak study, 4 to 6 as moderate, and scores of ≥ 6 as strong study26 (Table 3). Then, a summary of the articles was presented in multidimensional tables. Also, the mean score and P value were evaluated and compared.
Table 3.
Evaluating and scoring the quality of reviewed articles
|
Author
|
Pointing to being random
|
Proper randomization
|
A blind investigation
|
Blinding (single blind=0.5 double blind=1)
|
Refers to trial interruptions and crashes
|
Refer to the inclusion and exclusion criteria
|
Reference to the method of investigating & unwanted side effects
|
Reference to the statistical analysis method
|
Total points
|
Quality level
|
Yes
1
|
No
0
|
Yes
1
|
No
-1
|
Not mentioned 0
|
Yes
1
|
No
0
|
Yes
1
|
No
-1
|
Not mentioned 0
|
Yes
1
|
No
0
|
Yes
1
|
No
0
|
Yes
1
|
No 0
|
Yes
1
|
No
0
|
|
|
| Blank et al16 |
* |
|
* |
|
|
* |
|
0.5 |
|
|
* |
|
* |
|
|
* |
* |
|
7.5 |
H |
| Blank et al17 |
* |
|
* |
|
|
* |
|
0.5 |
|
|
* |
|
* |
|
|
* |
* |
|
7.5 |
H |
| Côté et al18 |
* |
|
|
* |
|
|
* |
|
|
* |
* |
|
* |
|
* |
|
* |
|
4 |
M |
| Eller et al19 |
* |
|
* |
|
|
* |
|
0.5 |
|
|
* |
|
* |
|
|
* |
* |
|
5.5 |
M |
| Hanrahan et al20 |
* |
|
* |
|
|
* |
|
0.5 |
|
|
* |
|
* |
|
|
* |
* |
|
6.5 |
H |
| Holstad et al21 |
* |
|
* |
|
|
|
* |
|
* |
|
* |
|
* |
|
* |
|
* |
|
5 |
H |
| Lowther et al22 |
* |
|
* |
|
|
|
* |
|
* |
|
* |
|
* |
|
|
* |
* |
|
4 |
M |
| Madhombiro et al 23 |
* |
|
* |
|
|
* |
|
0.5 |
|
|
|
* |
* |
|
|
* |
* |
|
5.5 |
M |
| Nkhoma et al24 |
* |
|
* |
|
|
* |
|
* |
|
|
* |
|
* |
|
* |
|
* |
|
8 |
H |
| Wang et al25 |
* |
|
* |
|
|
|
* |
|
|
* |
* |
|
* |
|
* |
|
* |
|
6 |
H |
Quality level: H=High; M=Moderate.
Results
Since psychological support for patients with AIDS/HIV includes any support provided to help HIV/AIDS patients improve psychological, cognitive, emotional, and behavioral well-being, the results of the studies which performed the interventions according to this definition are explained in this section. Accordingly, a total of 1975 participants started interventions and 1687 included in the analyses at the final follow-up, however, the numbers were sometimes unclearly reported. Participants included adults of any age diagnosed with HIV/AIDS. One study involved only women.21The sample size varied from 11625 to 23816,17,20 participants. Women involved 41.77% of the total population. The mean age of the participants was 42/49 years. Also, 40% of these studies were conducted in America, 40% in Africa, 10% in Europe and 10% in Asia. The articles were evaluated by the modified Jadad scale. The assessment included the effect of randomization, appropriate randomization, blind study, appropriate blinding, inclusion and exclusion criteria, adverse complications, and statistical analysis.26 Of the 10 studies extracted, 1 was a quasi-experimental study, 8 were randomized clinical trials, and 1 was cluster randomized clinical trial. Also, 40% (n=4) had moderate quality and 60% (n=6) had high quality (Table 3).
Nurses’ interventions in the above mentioned studies included virtual intervention and training of emotional management skills, communication skills, motivational and problem-solving skills, home care and counseling services, symptom and side effects management services, palliative care services, case management, and motivational interviewing with cognitive behavioral therapy.
The patients were followed-up by phone or in-person. The duration of Interventions varied from one training session to 12 months. The duration of follow-up varied from 8 weeks to 24 months. In six studies, the effects of the designed psychological intervention were compared with routine care group.16,17,20,22,23,25 in other studies, the effects of two designed interventions were compared compared.18,19,21,24 The study units in 9 studies were male and female patients with AIDS/HIV and in one study only women with AIDS/HIV were included. Interventions were performed on patients with different ages and stages of the disease and different underlying diseases.23
Accordingly, 3 studies reported a decrease in the severity of depression and its symptoms after the intervention.19,20,25 Also, 3 studies emphasized the improvement of patients’ adherence to the treatment regimen and the use of antiviral medications after the intervention,18,21,25 but in one of these three studies (semi-experimental study with moderate tool score),18despite the improvement in adherence to treatment, there was no significant difference between the intervention and the control groups. One article suggested that conducting a group motivational interview and a problem-solving program led to a reduction in risky behaviors in women and increased use of contraceptive methods during sexual intercourse.21 Blank et al also found that home-based care programs, counseling on medical and psychological issues and effective coordination between health care providers reduce the viral load and increase the CD4 + T cell count.16,17Concerning the effectiveness of nursing interventions on patients’ pain and managing it, some studies showed that pain intensity can be reduced by receiving palliative care and face-to-face and phone-based patient education.22,24 Moreover, the quality of life, especially in the mental and physical dimensions, significantly increased after the quantitative and qualitative improvement of the nurse’s interaction with the patient at home.17,20,25A study also showed that nurses’ use of motivational interviews along with cognitive behavioral therapy can reduce the alcohol use disorder recognition test score in patients with AIDS/HIV who consume alcohol even after six months. Also, this supportive intervention can improve the viral load, quality of life and performance of these patients.23
In addition to the main results, some studies reported secondary outcomes. Accordingly, providing patient education (motivational skills, recognizing emotional and management skills, problem-solving, and communicating with others) and virtual follow-up can improve patients’ self-efficacy and reduce perceived stress18,19,22,24; this intervention increases perceived social support and reduce the incidence of complications associated with the disease. Also, it improves a positive attitude and reduces anxiety.18 Face-to-face training and providing pamphlets and educational booklets to the patient and family, as well as telephone follow-up make the patient’s pain less interfering with daily life and increase patient and family knowledge and motivation for pain management.24 Also, providing patients with palliative care compared to routine care makes them less likely to experience psychological distress, reduces their anxiety, increases family capacity for future planning, and improves their quality of life.22 Theoretical and practical training in the management of disease symptom makes patients use positive self-care and self-management strategies to improve their mental health.19
Discussion
Given the significant impact of psychological health conditions on physical health, medical care, quality of life, and risk of HIV transmission, this study was conducted to review and summarize the psychological interventions performed by nurses on patients with AIDS/HIV. To achieve this goal, eight RCTs, one semi-experimental, and one cRCT study were reviewed and evaluated. The results of this systematic review showed that interventions such as virtual or face-to-face educational programs, written information resources, palliative care, motivational interviewing, case management, motivational interviewing with cognitive-behavioral therapy, and home care with face-to-face or telephone follow-up can positively affect the quality of life, manage disease and symptoms, increase patients’ adherence to treatment, improve their mental and functional health, and reduce patients’ risky behaviors. These psychological interventions can be done by nurses independently because they have the skills to deliver them. This is an important point because it is associated with improving patient-related outcomes and achieving health policy goals, and development of nurses’ professional roles.
Since this study is the first study to answer the research question “what are nursing psychological interventions in patients with AIDS/HIV and what are the consequences?”, therefore, the findings of other similar studies were used to compare the results:
The results of the Borgmann and Schmidt showed that psychological interventions improved the quality of life of men with prostate cancer. They found that the patients who participated in psychological interventions had a higher quality of life at the end of the interventions. This improvement was significant in the physical dimension, but there was no evidence to support the significant effect of the interventions in the psychological dimension.27 Anderson and Ozakinci in a review study examined the impact of psychological interventions on the quality of life of patients with chronic conditions; they reported the significant effect of such interventions on the quality of life.28 However, the results of a systematic review study by Timmer et al contradict the present study. They evaluated the impact of psychological interventions on patients with inflammatory bowel disease, and reported that of the 21 clinical trials reviewed, there was no evidence to support the effectiveness of psychiatric interventions on quality of life in adult patients.29 In the study of MacKenzie et al there was no evidence to support the effectiveness of psychological interventions on the quality of life of patients undergoing strabismus surgery.30
In the present study, the impact of psychological interventions on high-risk behaviors of patients with AIDS/HIV was reported in a moderate-quality study. Risky sexual behaviors appear to be related to the psychological health of patients with AIDS/HIV. One study found that women with negative emotions were not able to cope with stress due to the desire to use condoms in sexual intercourse. There was also a significant relationship between hopelessness and loneliness and sexual risk in homosexual men.31 Another study which examined the relationship between depression and condom use among 278 Chinese women found that 62% of participants had severe depression and were less likely to use condoms consistently.32 These results emphasize that psychological interventions may reduce the risk of sexual behaviors and thus decrease HIV transmission. Meader et al also reported that women with drug abuse change their high-risk behaviors, such as sexual and injective behaviors, if they receive psychological interventions. However, there was no significant difference between women receiving psychological intervention and those receiving routine care.33 Carvalho et al also reported the limited effect of behavioral interventions on condom use in women with HIV.34 However, given that only one study examined high-risk behaviors in women, no definite conclusions can be made on the impact of psychological interventions to increase protected sex behaviors among patients.
Kisely et al in a study with moderate quality found that psychological intervention, especially those with the cognitive-behavioral approach, will be effective on heart pain in people without coronary artery disease.35 Another study with good quality reported that psychological interventions along with medical treatments play an important role for patients to manage pain.36 The benefits of using psychological approaches include increasing pain self-control, improving pain management, reducing pain-related disability, and reducing emotional stress through self-monitoring, and behavioral and cognitive therapy. Implementing these interventions can help patients more control pain. Also, the skills trained through psychological interventions enable patients to actively manage their disease and provide valuable skills that patients can apply in their life.37 However, Ziehm et al in their systematic review stated that psychological interventions didn’t decrease the pain of patients undergoing open-heart surgery.38
Psychological interventions can also affect different aspects of psychological health in patients with AIDS/HIV. In addition to physical problems such as pain and lack of energy, psychological health problems such as depression and anxiety are also common among patients with AIDS/HIV.39 The prevalence of mood disorders or depressive symptoms is approximately 33% and the prevalence of anxiety is about 20%.40 Thus, psychological interventions appear to be associated with improved depression, anxiety, and distress. Consistent with this finding, a review study showed that psychological interventions leads to a short, mid, and long-term reduction in the severity of depression in diabetic patients.41 Ziehm et al also reported that psychological interventions can reduce the psychological stress experienced in patients undergoing open-heart surgery.38 In contrast to the findings of the present study, the results of a systematic review did not confirm the effectiveness of psychological interventions on the improvement of psychological health of patients with sickle cell anemia.42 Also, Natale et al.didn’t confirm the impact of psychological interventions on major depression in hemodialysis patients.43 Fisher et al also found no significant difference between the psychological intervention group and the usual care group in anxiety and depression among children with chronic and recurrent pain.44
The efficacy of psychological interventions on laboratory markers of patients with AIDS/HIV was also seen in two studies. They reported that providing medical and home care services to patients results in reduced viral load and improved CD4 + T cell. Since psychological factors (such as depressive symptoms and stress) affect immune function such as decreasing CD4 + T cell and increasing viral load,45therefore, psychological interventions with a positive impact on depression and anxiety in these patients may be influenced by laboratory results and immune function. Also, since psychological interventions lead to increased adherence to treatment, improvements in laboratory markers can be considered one of the therapeutic consequences of adherence. Locher et al also agree with the present findings regarding the impact of psychological interventions on viral load and adherence to treatment.46 Moreover, Chew et al also found that psychological interventions compared to routine care may lead to improved HbA1C outcomes in diabetic patients. Since the reviewed articles have low-quality levels, they emphasized that stronger evidence is needed to confirm the impact of psychological interventions on HbA1C levels.47 Madhombiro et al also reported similar results between the groups receiving the psychological intervention and routine care in terms of viral load and CD4 + T cell. Their finding contradicts the results of the present study.48
According to the results of the present study, psychological interventions also increase adherence to treatment. Adherence to treatment in patients with AIDS/HIV is important because it improves health and well-being and reduces the risk of infection transmission. Failure adherence to treatment is associated with psychological health problems and stressors, such as depression49 and anxiety.50 The results of a meta-analysis study showed that psychological factors are strongly associated with adherence to treatment.51 People with psychological health problems due to cognitive and behavioral problems such as fatigue, hopelessness, decreased motivation and concentration may have more difficulty in seeking treatment.52 Psychological interventions primarily focus on psychological or social factors rather than just on medical factors. Therefore, psychological therapies may be a priority for adherence to treatment. Goldbeck et al also emphasize the positive effect of psychological interventions on diet in children with cystic fibrosis.53 These differences in different studies can be attributed to differences in the power and quality of studies, and intervention protocols (provider, skill level, content, style, duration of intervention, etc.), and target groups.
One of the strengths of this study is that it was conducted comprehensively because several databases and reviewed articles published from 2009 to 2022 were searched. Also, to the best of our knowledge, this systematic review is one of the first records to document the psychological interventions directly provided by nurses to patients with AIDS/HIV. So it can be a guideline for future research. Limitations of this review study include lack of access to full-text articles despite contact with authors and lack of knowledge of authors in non-English languages. The results of this study may also be influenced by the bias in the studies and a considerable degree of heterogeneity between them. In general, given the limited literature in this area, it is needed for further clinical trials on the research question. Meta-analysis studies are also recommended to gain a clear understanding of the results.
Conclusions
There is evidence that nurses are able to independently design and implement effective psychological interventions for patients with AIDS/HIV. This is a fundamental step for developing the professional roles of nurses and improving the care of AIDS/HIV patients. These interventions lead to the achievement of health goals in the physical, psychological, behavioral and laboratory fields. However, the clinical impact of these results is unclear because this systematic review only summarized and reported results qualitatively. Therefore, it is not possible to measure the intensity of the interventions from this systematic review. So, it is suggested to conduct meta-analysis studies to determine the intensity of the effect of each of these interventions on specific aspects of the problems of patients with AIDS/HIV.
Acknowledgments
The authors would like to thank all the authors of the articles used in this review study. Also, the central library authorities of Mashhad University of Medical Sciences is appreciated for providing access to related studies from various databases.
Authors’ Contribution
Conceptualization: Malihe Davoudi, Abbas Heydari, Zahra Sadat Manzari.
Data curation: Malihe Davoudi.
Formal analysis: Malihe Davoudi, Zahra Sadat Manzari.
Funding acquisition: Abbas Heydari.
Methodology: Malihe Davoudi, Abbas Heydari, Zahra Sadat Manzari.
Project administration: Abbas Heydari.
Supervision: Abbas Heydari, Zahra Sadat Manzari.
Writing–original draft: Malihe Davoudi.
Writing–review & editing: Abbas Heydari, Zahra Sadat Manzari.
COI-statement
There is no conflict of interest.
Data Availability
All data generated or analyzed during this study are included in this published article.
Ethical Approval
Ethical considerations have been observed in all stages of research, including the study and collection of data, their documentation, analysis, and publication.
Funding
The financial support of this study was provided by the Research and Technology Vice-Chancellor of Mashhad University of Medical Sciences.
Research Highlights
What is the current knowledge?
-
HIV/AIDS patients experience significant medically and psychologically suffering
-
One of the traditional responsibilities and roles of nurses is psychological support for these patients.
-
We do not know what interventions nurses can take directly and independently to provide psychological support to these patients and what are the consequences.
What is new here?
-
Virtual and face-to-face training programs, written information resources, palliative care, motivational interviewing, case management, visits and home care services along with face-to-face and telephone follow-up can be done directly by nurses.
-
Psychological interventions have a significant positive effect on quality of life and management of high-risk behaviors, disease management, and adherence to treatment, immune system function and psychological health in patients with HIV/AIDS.
References
- World Health Organization (WHO). Global HIV & AIDS Statistics—Fact Sheet. 2019. Available from: https://www.unaids.org/en/resources/fact-sheet.
- Paul AA, Premraj FC. Psychosocial problems and its impact faced by the HIV/AIDS infected patients. IOSR J Humanit Soc Sci 2008; Available from: https://www.iosrjournals.org/iosr-jhss/papers/Conf.17004/Volume-3/7.%2040-45.pdf.
- Pahuja M, Merlin J, Selwyn PA, Sullivan M. Issues in HIV/AIDS in Adults in Palliative Care. 2021. Available from: https://www.uptodate.com/contents/issues-in-hiv-aids-in-adults-in-palliative-care#:~:text=Associated%20conditions%20%E2%80%93%20Co%2Doccurring%20pain,and%20substance%20use%20%5B71%2C111%2C112%5D.
- Owe-Larsson B, Säll L, Salamon E, Allgulander C. HIV infection and psychiatric illness. Afr J Psychiatry (Johannesbg) 2009; 12(2):115-28. doi: 10.4314/ajpsy.v12i2.43729 [Crossref] [ Google Scholar]
- Yi S, Chhoun P, Suong S, Thin K, Brody C, Tuot S. AIDS-related stigma and mental disorders among people living with HIV: a cross-sectional study in Cambodia. PLoS One 2015; 10(3):e0121461. doi: 10.1371/journal.pone.0121461 [Crossref] [ Google Scholar]
- Buckingham E, Schrage E, Cournos F. Why the Treatment of mental disorders is an important component of HIV prevention among people who inject drugs. Adv Prev Med 2013; 2013:690386. doi: 10.1155/2013/690386 [Crossref] [ Google Scholar]
- Hughes E, Bassi S, Gilbody S, Bland M, Martin F. Prevalence of HIV, hepatitis B, and hepatitis C in people with severe mental illness: a systematic review and meta-analysis. Lancet Psychiatry 2016; 3(1):40-8. doi: 10.1016/s2215-0366(15)00357-0 [Crossref] [ Google Scholar]
- Chuah FLH, Haldane VE, Cervero-Liceras F, Ong SE, Sigfrid LA, Murphy G. Interventions and approaches to integrating HIV and mental health services: a systematic review. Health Policy Plan 2017; 32(Suppl 4):iv27-iv47. doi: 10.1093/heapol/czw169 [Crossref] [ Google Scholar]
- Dumitru G, Irwin K, Tailor A. Updated federal recommendations for HIV prevention with adults and adolescents with HIV in The United States: the pivotal role of nurses. J Assoc Nurses AIDS Care 2017; 28(1):8-18. doi: 10.1016/j.jana.2016.09.011 [Crossref] [ Google Scholar]
- Tunnicliff SA, Piercy H, Bowman CA, Hughes C, Goyder EC. The contribution of the HIV specialist nurse to HIV care: a scoping review. J Clin Nurs 2013; 22(23-24):3349-60. doi: 10.1111/jocn.12369 [Crossref] [ Google Scholar]
- Wood JH, Chambers M, White SJ. Nurses’ knowledge of and attitude to electroconvulsive therapy. J ect 2007; 23(4):251-4. doi: 10.1097/yct.0b013e31813e0692 [Crossref] [ Google Scholar]
- Papathanassoglou ED. Psychological support and outcomes for ICU patients. Nurs Crit Care 2010; 15(3):118-28. doi: 10.1111/j.1478-5153.2009.00383.x [Crossref] [ Google Scholar]
- The Australasian Society for HIV, Viral Hepatitis and Sexual Health Medicine (ASHM). Standards for Psychological Support for Adults with HIV. 2010. Available from: https://www.bhiva.org/file/BbShtfyMFNKCz/Standards_for_psychological_support_for_adults_living_with_HIV.pdf.
- Cumpston M, Li T, Page MJ, Chandler J, Welch VA, Higgins JP. Updated guidance for trusted systematic reviews: a new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst Rev 2019; 10:ED000142. doi: 10.1002/14651858.ed000142 [Crossref] [ Google Scholar]
- Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 2009; 6(7):e1000097. doi: 10.1371/journal.pmed.1000097 [Crossref] [ Google Scholar]
- Blank MB, Hanrahan NP, Fishbein M, Wu ES, Tennille JA, Ten Have TR. A randomized trial of a nursing intervention for HIV disease management among persons with serious mental illness. Psychiatr Serv 2011; 62(11):1318-24. doi: 10.1176/ps.62.11.pss6211_1318 [Crossref] [ Google Scholar]
- Blank MB, Hennessy M, Eisenberg MM. Increasing quality of life and reducing HIV burden: the PATH + intervention. AIDS Behav 2014; 18(4):716-25. doi: 10.1007/s10461-013-0606-x [Crossref] [ Google Scholar]
- Côté J, Godin G, Ramirez-Garcia P, Rouleau G, Bourbonnais A, Guéhéneuc YG. Virtual intervention to support self-management of antiretroviral therapy among people living with HIV. J Med Internet Res 2015; 17(1):e6. doi: 10.2196/jmir.3264 [Crossref] [ Google Scholar]
- Eller LS, Kirksey KM, Nicholas PK, Corless IB, Holzemer WL, Wantland DJ. A randomized controlled trial of an HIV/AIDS Symptom Management Manual for depressive symptoms. AIDS Care 2013; 25(4):391-9. doi: 10.1080/09540121.2012.712662 [Crossref] [ Google Scholar]
- Hanrahan NP, Wu E, Kelly D, Aiken LH, Blank MB. Randomized Clinical trial of the effectiveness of a home-based advanced practice psychiatric nurse intervention: outcomes for individuals with serious mental illness and HIV. Nurs Res Pract 2011; 2011:840248. doi: 10.1155/2011/840248 [Crossref] [ Google Scholar]
- Holstad MM, DiIorio C, Kelley ME, Resnicow K, Sharma S. Group motivational interviewing to promote adherence to antiretroviral medications and risk reduction behaviors in HIV infected women. AIDS Behav 2011; 15(5):885-96. doi: 10.1007/s10461-010-9865-y [Crossref] [ Google Scholar]
- Lowther K, Selman L, Simms V, Gikaara N, Ahmed A, Ali Z. Nurse-led palliative care for HIV-positive patients taking antiretroviral therapy in Kenya: a randomised controlled trial. Lancet HIV 2015; 2(8):e328-34. doi: 10.1016/s2352-3018(15)00111-3 [Crossref] [ Google Scholar]
- Madhombiro M, Kidd M, Dube B. Effectiveness of a psychological intervention delivered by general nurses for alcohol use disorders in people living with HIV in Zimbabwe: a cluster randomized controlled trial. J Int AIDS Soc 2020; 23(12):e25641. doi: 10.1002/jia2.25641 [Crossref] [ Google Scholar]
- Nkhoma K, Seymour J, Arthur A. An educational intervention to reduce pain and improve pain management for malawian people living with HIV/AIDS and their family carers: a randomized controlled trial. J Pain Symptom Manage 2015;50(1):80-90.e4. 10.1016/j.jpainsymman.2015.01.011
- Wang H, Zhou J, Huang L, Li X, Fennie KP, Williams AB. Effects of nurse-delivered home visits combined with telephone calls on medication adherence and quality of life in HIV-infected heroin users in Hunan of China. J Clin Nurs 2010; 19(3-4):380-8. doi: 10.1111/j.1365-2702.2009.03048.x [Crossref] [ Google Scholar]
- Lempesi E, Koletsi D, Fleming PS, Pandis N. The reporting quality of randomized controlled trials in orthodontics. J Evid Based Dent Pract 2014; 14(2):46-52. doi: 10.1016/j.jebdp.2013.12.001 [Crossref] [ Google Scholar]
- Borgmann H, Schmidt S. [Psychosocial interventions for men with prostate cancer]. Urologe A 2015; 54(6):863-6. doi: 10.1007/s00120-015-3858-4 [Crossref] [ Google Scholar]
- Anderson N, Ozakinci G. Effectiveness of psychological interventions to improve quality of life in people with long-term conditions: rapid systematic review of randomised controlled trials. BMC Psychol 2018; 6(1):11. doi: 10.1186/s40359-018-0225-4 [Crossref] [ Google Scholar]
- Timmer A, Preiss JC, Motschall E, Rücker G, Jantschek G, Moser G. Psychological interventions for treatment of inflammatory bowel disease. Cochrane Database Syst Rev 2011(2):CD006913. doi: 10.1002/14651858.CD006913.pub2 [Crossref]
- MacKenzie K, Hancox J, McBain H, Ezra DG, Adams G, Newman S. Psychosocial interventions for improving quality of life outcomes in adults undergoing strabismus surgery. Cochrane Database Syst Rev 2016; 2016(5):CD010092. doi: 10.1002/14651858.CD010092.pub4 [Crossref] [ Google Scholar]
- Su X, Zhou AN, Li J, Shi LE, Huan X, Yan H. Depression, loneliness, and sexual risk-taking among HIV-negative/unknown men who have sex with men in China. Arch Sex Behav 2018; 47(7):1959-68. doi: 10.1007/s10508-017-1061-y [Crossref] [ Google Scholar]
- Hong Y, Li X, Fang X, Zhao R. Depressive symptoms and condom use with clients among female sex workers in China. Sex Health 2007; 4(2):99-104. doi: 10.1071/sh06063 [Crossref] [ Google Scholar]
- Meader N, Li R, Des Jarlais DC, Pilling S. Psychosocial interventions for reducing injection and sexual risk behaviour for preventing HIV in drug users. Cochrane Database Syst Rev 2010; 2010(1):CD007192. doi: 10.1002/14651858.CD007192.pub2 [Crossref] [ Google Scholar]
- Carvalho FT, Gonçalves TR, Faria ER, Shoveller JA, Piccinini CA, Ramos MC. Behavioral interventions to promote condom use among women living with HIV. Cochrane Database Syst Rev 2011(9):CD007844. doi: 10.1002/14651858.CD007844.pub2 [Crossref]
- Kisely SR, Campbell LA, Skerritt P, Yelland MJ. Psychological interventions for symptomatic management of non-specific chest pain in patients with normal coronary anatomy. Cochrane Database Syst Rev 2010(1):CD004101. doi: 10.1002/14651858.CD004101.pub3 [Crossref]
- Jensen MP. Psychosocial approaches to pain management: an organizational framework. Pain 2011; 152(4):717-25. doi: 10.1016/j.pain.2010.09.002 [Crossref] [ Google Scholar]
- Roditi D, Robinson ME. The role of psychological interventions in the management of patients with chronic pain. Psychol Res Behav Manag 2011; 4:41-9. doi: 10.2147/prbm.s15375 [Crossref] [ Google Scholar]
- Ziehm S, Rosendahl J, Barth J, Strauss BM, Mehnert A, Koranyi S. Psychological interventions for acute pain after open heart surgery. Cochrane Database Syst Rev 2017; 7(7):CD009984. doi: 10.1002/14651858.CD009984.pub3 [Crossref] [ Google Scholar]
- Morrison MF, Petitto JM, Ten Have T, Gettes DR, Chiappini MS, Weber AL. Depressive and anxiety disorders in women with HIV infection. Am J Psychiatry 2002; 159(5):789-96. doi: 10.1176/appi.ajp.159.5.789 [Crossref] [ Google Scholar]
- Evans DL, Charney DS, Lewis L, Golden RN, Gorman JM, Krishnan KR. Mood disorders in the medically ill: scientific review and recommendations. Biol Psychiatry 2005; 58(3):175-89. doi: 10.1016/j.biopsych.2005.05.001 [Crossref] [ Google Scholar]
- Baumeister H, Hutter N, Bengel J. Psychological and pharmacological interventions for depression in patients with diabetes mellitus: an abridged Cochrane review. Diabet Med 2014; 31(7):773-86. doi: 10.1111/dme.12452 [Crossref] [ Google Scholar]
- Anie KA. Psychological complications in sickle cell disease. Br J Haematol 2005; 129(6):723-9. doi: 10.1111/j.1365-2141.2005.05500.x [Crossref] [ Google Scholar]
- Natale P, Palmer SC, Ruospo M, Saglimbene VM, Rabindranath KS, Strippoli GF. Psychosocial interventions for preventing and treating depression in dialysis patients. Cochrane Database Syst Rev 2019; 12(12):CD004542. doi: 10.1002/14651858.CD004542.pub3 [Crossref] [ Google Scholar]
- Fisher E, Law E, Dudeney J, Palermo TM, Stewart G, Eccleston C. Psychological therapies for the management of chronic and recurrent pain in children and adolescents. Cochrane Database Syst Rev 2018; 9(9):CD003968. doi: 10.1002/14651858.CD003968.pub5 [Crossref] [ Google Scholar]
- Ironson G, O’Cleirigh C, Fletcher MA, Laurenceau JP, Balbin E, Klimas N. Psychosocial factors predict CD4 and viral load change in men and women with human immunodeficiency virus in the era of highly active antiretroviral treatment. Psychosom Med 2005; 67(6):1013-21. doi: 10.1097/01.psy.0000188569.58998.c8 [Crossref] [ Google Scholar]
- Locher C, Messerli M, Gaab J, Gerger H. Long-term effects of psychological interventions to improve adherence to antiretroviral treatment in HIV-infected persons: a systematic review and meta-analysis. AIDS Patient Care STDS 2019; 33(3):131-44. doi: 10.1089/apc.2018.0164 [Crossref] [ Google Scholar]
- Chew BH, Vos RC, Metzendorf MI, Scholten RJ, Rutten GE. Psychological interventions for diabetes-related distress in adults with type 2 diabetes mellitus. Cochrane Database Syst Rev 2017; 9(9):CD011469. doi: 10.1002/14651858.CD011469.pub2 [Crossref] [ Google Scholar]
- Madhombiro M, Musekiwa A, January J, Chingono A, Abas M, Seedat S. Psychological interventions for alcohol use disorders in people living with HIV/AIDS: a systematic review. Syst Rev 2019; 8(1):244. doi: 10.1186/s13643-019-1176-4 [Crossref] [ Google Scholar]
- Gonzalez JS, Batchelder AW, Psaros C, Safren SA. Depression and HIV/AIDS treatment nonadherence: a review and meta-analysis. J Acquir Immune Defic Syndr 2011; 58(2):181-7. doi: 10.1097/QAI.0b013e31822d490a [Crossref] [ Google Scholar]
- Safren SA, O’Cleirigh C, Tan JY, Raminani SR, Reilly LC, Otto MW. A randomized controlled trial of cognitive behavioral therapy for adherence and depression (CBT-AD) in HIV-infected individuals. Health Psychol 2009; 28(1):1-10. doi: 10.1037/a0012715 [Crossref] [ Google Scholar]
- Langebeek N, Gisolf EH, Reiss P, Vervoort SC, Hafsteinsdóttir TB, Richter C. Predictors and correlates of adherence to combination antiretroviral therapy (ART) for chronic HIV infection: a meta-analysis. BMC Med 2014; 12:142. doi: 10.1186/preaccept-1453408941291432 [Crossref] [ Google Scholar]
- Wagner GJ, Goggin K, Remien RH, Rosen MI, Simoni J, Bangsberg DR. A closer look at depression and its relationship to HIV antiretroviral adherence. Ann Behav Med 2011; 42(3):352-60. doi: 10.1007/s12160-011-9295-8 [Crossref] [ Google Scholar]
- Goldbeck L, Fidika A, Herle M, Quittner AL. Psychological interventions for individuals with cystic fibrosis and their families. Cochrane Database Syst Rev 2014; 2014(6):CD003148. doi: 10.1002/14651858.CD003148.pub3 [Crossref] [ Google Scholar]