Journal of caring sciences. 12(2):103-109.
doi: 10.34172/jcs.2023.31856
Original Article
Psychometric Properties of the Greek Version of Demoralization Scale-II (DS-II) in Patients with Cancer
Tania-Flora Elmasian Conceptualization, Investigation, Methodology, Resources, Writing – original draft, 1 
Maria Nikoloudi Data curation, 2
Eleni Tsilika Formal analysis, Supervision, Validation, Visualization, 3
Sotiria Kostopoulou Resources, Writing – original draft, Writing – review & editing, 2
Anna Zygogianni Supervision, 4
Stylianos Katsaragakis Supervision, 5
Kyriaki Mystakidou Project administration, 2, *
Author information:
1Social Policy and Social Anthropology, Ministry of Migration and Asylum, Asylum Service Case Officer, Greece
2Pain Relief and Palliative Care Unit, Aretaieion Hospital, National & Kapodistrian University of Athens, School of Medicine, Athens, Greece
3Health Psychologist, Pain Relief and Palliative Care Unit, Aretaieion Hospital, National & Kapodistrian University of Athens, School of Medicine, Athens, Greece
4Department of Radiology, Aretaieion Hospital, School of Medicine, National & Kapodistrian University of Athens, Athens, Greece
5Department of Nursing, National and Kapodistrian University of Athens, Athens, Greece
Abstract
Introduction:
The concept of demoralization is used to describe situations of existential distress and self-perceived inability to effectively deal with stressors. The Demoralization Scale-II (DS-II) is a short and modified version of the original DS that measures the level of demoralization in patients. The purpose of this study is to evaluate the psychometric properties of the Greek version of the Greek Demoralisation Scale-II (DS-II GR) in the population of patients with cancer.
Methods:
The main tool used in this cross-sectional study is the DS-II GR translated and evaluated for its psychometric properties in a sample of 150 Greek patients with cancer. Exploratory factor analysis (EFA), confirmatory factor analysis (CFA), convergent validity, known groups’ validity, cut-off points, internal consistency reliability and test-retest reliability were done.
Results:
According to the CFA, a two-factor model emerged with a different conceptual content and grouping than the original. The correlation coefficients between DS-II GR and Hospital Anxiety and Depression Scale-Greek (HADS-GR) The internal consistency of DS-II GR for factor 1, factor 2, and total score were measured with Cronbach’s alpha and calculated to be 0.906, 0.810, and 0.913.
Conclusion:
The Greek version of the demoralization scale is reliable and valid for assessing demoralization in Greek patients with cancer.
Keywords: Cancer, Palliative care, Anxiety, Depression, Demoralization
Copyright and License Information
© 2023 The Author(s).
This work is published by Journal of Caring Sciences as an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by-nc/4.0/). Non-commercial uses of the work are permitted, provided the original work is properly cited.
Introduction
Demoralization refers to a persistent failure of coping with stress as defined by Jerome Frank thirty years ago. Feelings of despair, isolation, hopelessness, loss of meaning and existential distress are the core features of the definition of demoralization.1,2 The necessity of examining it in patients with cancer and its complications: Physical symptoms in cancer patients may affect the increment of demoralisation.3 In addition, when patients cannot effectively manage stressful situations they feel a sense of helplessness and incompetence, which results in the feeling of lost significance and purpose in life. This psychological reaction is common among patients with advanced cancer. Demoralization in patients with cancer is closely correlated to depression. Moreover, demoralization and depression increase the risk of suicide among patients with cancer. Compared with depressed patients, demoralized patients require additional suicide-risk assessments. These results suggest that health care professionals must be sensitive to depression and demoralization syndromes in patients with cancer. The signs of demoralization are loss of purpose, meaning, hopelessness-helplessness.1,2 Demoralization is classified as a serious and potentially treatable condition.4There is a variety of psychometric tools for measuring and evaluating demoralization.4-10 The novelty of the present study is that this is the only study regarding the psychometric properties of the Demoralisation Scale-II (DS-II) in Greek patients with cancer.
The available tools to measure demoralization are: The DS,11The Short Demoralization Scale (SDS)12and a survey regarding demoralization as a diagnostic specifier for adjustment disorder and major depression.11
The aim of this study was to evaluate the psychometric properties of the Greek version of the DS II scale in oncology patients. The demoralization tool was chosen as it is the most commonly used instrument for the assessment of demoralization scale.
It is of interest the history of demoralization asthe prominent existential psychotherapist Irvin Yalom is central to the discussion on demoralization as a large focus of his work was related to existential distress. Yalom defined existential psychotherapy as a therapy that is dynamic and focused on the distress that is grounded in the individual’s existence. Demoralization can be understood to result from this existential conflict when a person lacks the resources to cope with such conflict of life.13Hopelessness, loss of meaning, and existential distress are proposed as the core features of the diagnostic category of demoralization syndrome. This syndrome can be differentiated from depression and is recognizable in palliative care settings. It is associated with chronic medical illness, disability, bodily disfigurement, fear of loss of dignity, social isolation, and where there is a subjective sense of incompetence feelings of greater dependency on others or the perception of being a burden. The impact of cancer on adverse emotional conditions such as despair can instigate the progression of suicidal ideation which, in turn, can contribute into actual suicidal behaviour. Additionally, because of the sense of impotence or helplessness, those with the syndrome predictably progress to a desire to die or to commit suicide.14 A treatment approach is described which the potential to alleviate the distress has caused by this syndrome. Overall, demoralization syndrome has satisfactory face, descriptive, predictive, construct, and divergent validity, suggesting its utility as a diagnostic category in palliative care.4 In patients with cancer, demoralization has been associated with stressors that reflect a state of existential discomfort and disintegration, destroying one’s sense of self-worth to effectively manage internal and external stimuli throughout the duration-stages of the disease.
Disease-related conditions range between existential integrity, spiritual well-being, a sense of serenity and severe existential despair.7 This syndrome includes diverse emotional states of despair and loss of meaning and purpose, along with cognitive perceptions of subjective impotence and personal failure in life that emerge from a sense of being trapped in a circumstance. The absence of a promising future due to the loss of values, roles, and goals, the lack of self-confidence and inner strength to achieve them, deprives the patient to establish effective and appropriate treatment methods.8 Jerome Frank coined the term demoralization in the 1970s.9 Clarke and Kissane hypothesized that demoralization syndrome is a distinct clinical entity characterized by symptoms: existential discomfort including despair, loss of meaning and purpose and cognitive-behavioural attitudes including pessimism, weakness, a sense of entrapment, personal failure, and lack of motivation. When combined with the absence of depressive symptoms, these effects should last for at least two weeks.2,4
The inclusion criteria included patients’ ≥ 18 years old, with advanced cancer diagnosis, considered to be as locally advanced, recurrent, or metastatic disease for solid cancers, and relapsed or refractory disease for hematologic tumours. A convenient sample of 150 from a total of 250 patients treated in the unit during that period participated in the study. All participants provided a written informed consent and underwent symptom evaluation by a specialist palliative care physician.
There has been much discussion about the syndrome of demoralization in palliative care.1Cancer can be demoralizing to patients because disrupts their biopsychosocial status and equilibrium threating their physical and mental integrity.1-4 Demoralization is a mental condition that has negative consequences for patients, making them vulnerable and jeopardizing the success of therapeutic interventions, a factor that may be associated with the desire for premature death.5,6 Kissane et al differentiated demoralization from depression and found that 7–14% of patients with cancer were demoralized but not depressed.11 In a recent systematic review depression was significantly associated with high levels of demoralization.13 Untreated demoralization results in the development of depression at a later stage.15 The signs of depression are: lethargy and a loss of interest in enjoyable activities, while the signs of demoralization are: loss of purpose, meaning, hopelessness-helplessness.16,17 Demoralization is classified as a serious and potentially treatable condition.4 There is a variety of psychometric tools for measuring and evaluating demoralization.10,11,18-21The aim of this study was to evaluate the psychometric properties of the Greek version of the DS II scale in oncology patients. Measuring demoralization with valid instruments, such as the Greek version of the DS-II questionnaire, is important on reducing error in the measurement process. Measuring demoralization with valid instruments, such as the Greek version of the DS-II questionnaire, is important for the recognition of emotional and cognitive states of existential distress and demoralization in Greek patients with cancer.
The DS-II has demonstrated convergent validity with measures of psychological distress, quality of life, and attitudes toward the end of life. It also demonstrated discriminant validity, as the DS-II differentiated patients who had different functional performance levels and high/low symptoms, with a difference of 2 points between groups on the DS-II considered clinically meaningful. Furthermore, discriminant validity was demonstrated, as comorbidity with depression was not observed at moderate levels of demoralization.22
A study by Boxley et al23 examined the internal consistency and factor structure of the Hospital Anxiety and Depression Scale (HADS( in a polytrauma/traumatic brain injury clinic. A confirmatory factor analysis (CFA) of the depression and anxiety subscales showed that the two factors were highly correlated (r=0.70). Goodness of fit statistics for the two-factor model were acceptable. The HADS demonstrated very good reliability overall (alpha=0.89) and for the individual subscales (alpha=0.84). This study supports the use of the HADS as a screen for depression and anxiety.
Materials and Methods
In this prospective cross-sectional observational study, data were collected from 150 advanced patients with cancer in the First Radiology Laboratory and Palliative Care Unit “Jenny Karezi” of Aretaieion Hospital. Approval No: 255/02-10-2020 was granted by Aretaieion Ethics committee. The study was conducted in accordance with the Declaration of Helsinki and data was collected between 03/04/2019 and 18/09/2019. The first time 150 patients completed the DS-II GR questionnaire, while the second time 30 patients completed the questionnaire after 1-3 days for the reliability analysis.
A translation of the DS-II into Greek was performed using the “forward-backword” method: two independent bilingual health care professionals translated it to Greek and then two additional bilingual independent health-care professionals translated it back into English. A matching of these translations was then performed. Finally, a review of the translation of the English version and the reverse translation were performed with excellent results. The forward-back translation method was used to translate the original version of the questionnaire into Greek. The two versions were then compared, and minor changes were made to arrive at the final agreed-upon version.
The main tool for the current study was the DS II which is a short form of the DS. The DS-II is a 16-item, 2-factor scale that has demonstrated item fit, uni-dimensionality, and reliability as a measure of demoralization in patients receiving palliative care.21 The HADS was originally developed by Zigmond and Snaith and is commonly used to determine the levels of anxiety and depression that a person is experiencing.24 The HADS is a fourteen-item scale that generates: Seven of the items relate to anxiety and seven relate to depression. Zigmond and Snaith created this outcome measure specifically to avoid reliance on aspects of these conditions that are also common somatic symptoms of illness, for example fatigue and insomnia or hypersomnia. This, it was hoped, would create a tool for the detection of anxiety and depression in people with physical health problems.
The “receiver operating curve” (ROC) function curve analysis was used to find the cut-off points of the “Meaning and Purpose” factor, the “Discomfort” factor, and the overall score of the demoralization scale for the differentiation of subgroups of patients based on their level of stress ROC, calculating the corresponding areas under the curve (AUC). The maximum probability estimation method was used to calculate areas below the ROC curve with standard error and 95% confidence interval (CI), while the HADS score was used to assess the sensitivity and specificity of the different cut-off points of the “Meaning and Purpose” factor of “Discomfort” and the overall score. The HADS determined convergent validity, particularly the Greek version of the scale.24,25
The data were statistically processed using SPSS version 21. The indicators calculated and analysed performed were: exploratory factor analysis (EFA), CFA, convergent or criterion validity, known groups’ validity, cut-off points, internal consistency reliability and test-retest reliability.
Results
A two-factor model of the authentic DS-II scale emerged, marginally characterized by unacceptable global adjustment indicators. Subsequently, two factors also emerged of different conceptual content and grouping than the original scale. The correlation coefficients between DS-II GR and HAD anxiety were: factor 1 (r=0.60, P< 0.001), factor 2 (r=0.51, P<0.001), and total score (r=-0.62, P<0.001). The correlation coefficients between DS-II GR and HAD depression were: factor 1 (r=0.70, P<0.001), factor 2 (r=0.45, P<0.001), and total score (r=-0.66, P<0.001). The above results indicate a high correlation satisfying the convergent validity. The internal consistency of DS-II GR for factors 1, 2 and total score were measured with Cronbach’s alpha and calculated to be 0.90, 0.81, and 0.91 respectively. These values indicate excellent internal consistency.
The qualitative-quantitative demographic and clinical data of the study sample are found in Table 1.
Table 1.
Demographic and disease-related patient’s characteristics
|
Variables
|
No. (%)
|
| Gender |
| Men |
61) 40.7) |
| Women |
89 (59.3) |
| Educational level |
| Primary studies |
28 (18.7) |
| Secondary studies |
73 (48.7) |
| University studies |
49 (32.7) |
| Marital status |
| Married |
108(72.0) |
| Single |
11(7.3) |
| Divorced |
15(10.0) |
| Widowed |
16(10.7) |
| Cancer location |
| Breast |
50 (33.3) |
| Lung |
22 (14.7) |
| Urogenital |
28 (18.7) |
| Gastrointestinal tract |
36 (24.0) |
| Other |
14 (9.3) |
| Eastern cooperative oncology group score |
| 0–1 |
121 (80.7) |
| 2–3 |
29 (19.3) |
| Metastasis |
| No |
68 (45.3) |
| Yes |
82 (54.7) |
| Radiotherapy |
| No |
53 (35.3) |
| Yes |
97 (64.7) |
| Surgery |
| No |
32 (21.3) |
| Yes |
118 (78.7) |
| Caregiver |
| Children |
40 (26.7) |
| Relative |
104 (69.3) |
| Friends – Other |
6 (4.0) |
| Therapy |
| Curative |
146 (97.3) |
| Palliative |
4 (2.7) |
| Age |
| Mean (SD) |
61.51 |
| Disease duration |
| Median |
9.0 |
CFA: A two-factor model of the original DS-II was conducted by CFA giving unacceptable global fit indices. The resulting global fit indices χ2=256.5, chi-square-degrees of freedom ratio=2.49, root mean square error of approximation (RMSEA)=0.100, comparative fit index (CFI)=0.870, normed fit index (NFI)=0.803, goodness-of-fit index (GFI)=0.822, adjusted goodness-of-fit (AGFI)=0.766 showed that a two-factor solution proposed by the author should be rejected but marginally.
EFA: 16 items were analysed using an Oblique rotation. Two factors, with eigenvalue>1 and items factor loadings were≥0.40 were identified (Tables 2 and 3).
Table 2.
Eigenvalues and explained variance of DS-II questionnaire
|
Items
|
Eigenvalues
|
% of Variance
|
Cumulative %
|
| 1 |
7.33 |
45.83 |
45.83 |
| 2 |
1.54 |
9.67 |
55.50 |
| 3 |
0.92 |
5.81 |
|
| 4 |
0.84 |
5.01 |
|
| 5 |
0.73 |
4.61 |
|
| 6 |
0. 65 |
4.06 |
|
| 7 |
0.56 |
3.50 |
|
| 8 |
0.49 |
3.08 |
|
| 9 |
0.48 |
3.02 |
|
| 10 |
0.44 |
2.76 |
|
| 11 |
0.42 |
2.65 |
|
| 12 |
0.39 |
2.45 |
|
| 13 |
0.27 |
1.72 |
|
| 14 |
0.26 |
1.64 |
|
| 15 |
0.24 |
1.54 |
|
| 16 |
0.17 |
1.07 |
|
Table 3.
Factor loadings of DS-IIsubscales
|
Items
|
Factor 1
|
Factor 2
|
| 1 |
0.61 |
|
| 2 |
0.84 |
|
| 3 |
0.83 |
|
| 4 |
0.64 |
|
| 5 |
0.74 |
|
| 6 |
0.68 |
|
| 7 |
0.76 |
|
| 8 |
|
0.69 |
| 9 |
0.64 |
|
| 10 |
|
0.51 |
| 11 |
|
0.67 |
| 12 |
|
0.59 |
| 13 |
0.58 |
|
| 14 |
0.72 |
|
| 15 |
|
0.67 |
| 16 |
|
0.69 |
Extraction method: maximum likelihood; Rotation: oblique; only loadings with values>0.4 are presented.
CFA new structure: A two-factor model of DS-II was examined by CFA (Figure 1). The resulting global fit indices χ2 =193.64, chi-square-degrees of freedom (df) ratio=1.88, RMSEA=.071, CFI=0.905, NFI=0.900, GFI=0.860, AGFI=0.810 showed that the new two factor solution could be retained.
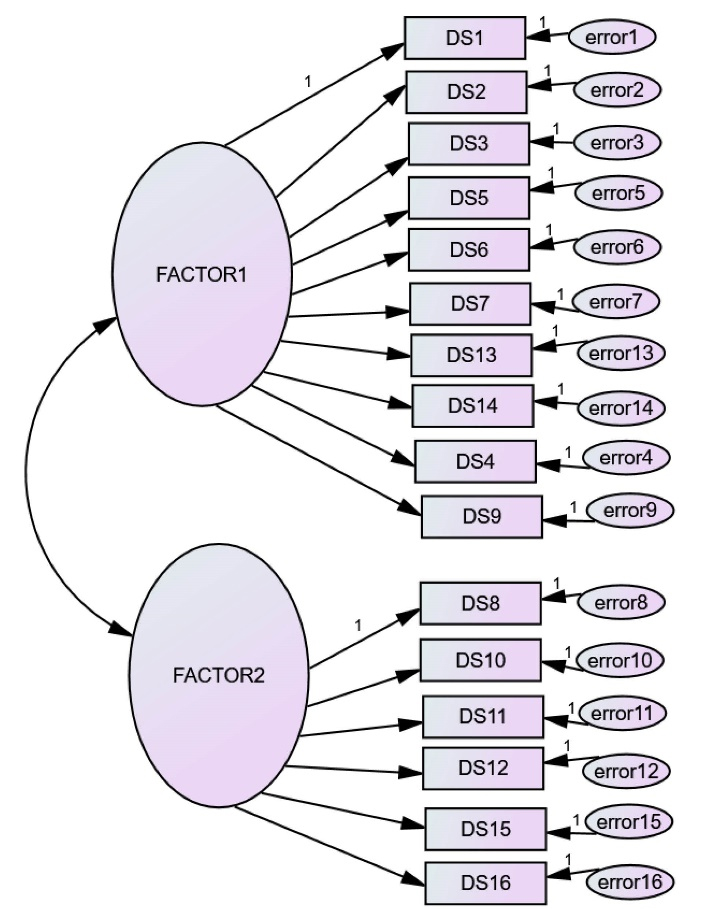
Figure 1.
Confirmatory factor analysis
.
Confirmatory factor analysis
Convergent or criterion validity: The correlation coefficients between Hospital Anxiety and Depression Scale anxiety and DS-II factors were: factor 1 (r=0.60, P< 0.001), factor 2 (r=0.51, P<0.001), total score (r=-0.62, P<0.001). The correlation coefficients between HAD depression and DS-II factors were: factor 1 (r=0.70, P<0.001), factor 2 (r=0.45, P<0.001), total score (r=-0.66, P<0.001), indicating high correlation between DS-II subscales and total score with HAD anxiety- depression scales which satisfied the criterion validity.
Known-groups validity: DS-II factor 1, 2 and total score were higher for patients with anxiety score>11 compared with those with score<11 (P<0.001; Table 4)
Table 4.
Known-group’s validity
|
HAD anxiety
|
N
|
Mean (SD)
|
P
value
*
|
| DS-II factor1 |
| <11 |
125 |
2.23 (3.06) |
<0.001 |
| ≥11 |
25 |
7.44 (6.00) |
| DS-II factor2 |
| <11 |
125 |
3.38 (2.62) |
<0.001 |
| ≥11 |
25 |
5.68 (2.59) |
| DS-II total |
| <11 |
125 |
5.61 (5.14) |
<0.001 |
| ≥11 |
25 |
13.12 (7.63) |
*Significant statistically.
The cut-off points of DS-II total score: The area under the curve (AUC) of DS-II total=0.818 (P<0.001).
The AUC of DS-II factor 1 was 0.778 (P<0.001). The AUC of DS-II factor 2 was 0.752 (P<0.001) (Figure 2).
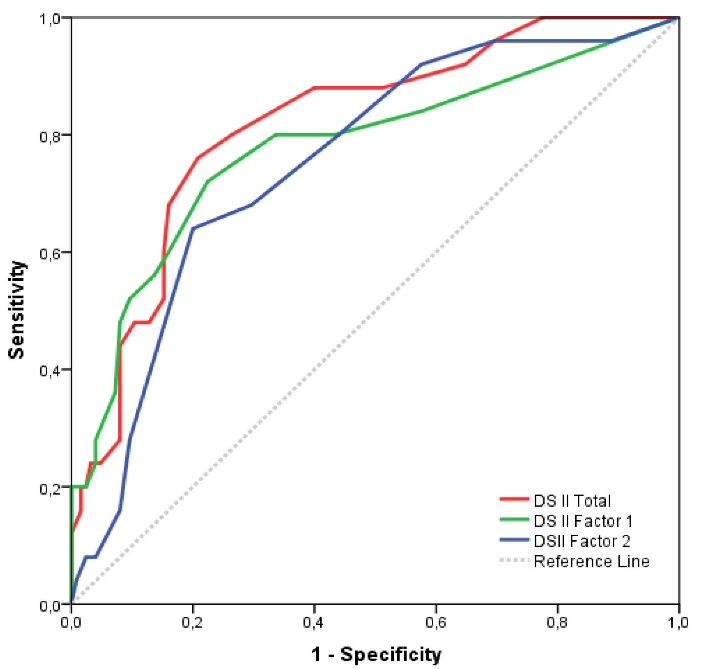
Figure 2.
Sensitivity and specificity of DS
.
Sensitivity and specificity of DS
Internal consistency reliability: The internal consistency of the DS-II factor 1, 2 and total score was measured with Cronbach’s alpha and estimated as 0.906, 0.810 and 0.913 indicate excellent internal consistency.
Test-retest reliability: The paired samples t-test between initial assessment and reassessment of DS-II subscales and total score found no statistically significant difference. The results of stability indicated that DS-II factor 1, 2 and total score were consistent between the two occasions (Table 5).
Table 5.
Test-retest reliability
|
(N=30)
|
ICC (95% CI)
|
Paired samples
t
test
|
P
value
|
|
Mean (SD)
|
|
|
Initial
|
Reassessment
|
|
| DS-II factor 1 |
0.89 (0.77-0.95) |
2.90(3.65) |
3.16(3.50) |
0.52 |
| DS-II factor 2 |
0.90 (0.79-0.95) |
4.2(2.85) |
4.1(2.92) |
0.75 |
| DS-II Total |
0.92 (0.84-0.96) |
7.10(6.06) |
7.26(6.20) |
0.78 |
ICC, intr aclass correlation coefficient
Discussion
The purpose of this study was to translate and investigate the psychometric properties of the demoralization scale by assessing its reliability and validity in Greek patients with cancer. According to the CFA a two-factor model of the authentic DS II index emerged, characterized by unacceptable global adjustment indicators. Thus, an EFA of the index followed, and two factors emerged. In the Greek version elements 4 and 9 were transferred to factor 1 resulting in two factors consisting of elements 10 and 6. In the original validation of the DS 5 factors had been emerged.11 Robinson et al suggested a 2-factor solution with 1 item deleted from each component: “I am not in good spirits” and “I am ashamed of what little I have accomplished”. Component 1 was labeled “Meaning and Purpose” while component 2 was labelled “Distress and Coping Ability”.26 The Spanish version the questionnaire contained the 2 factors of Robinson showing that item 10 “I have a lot of regret about my life” was not significant.27In the DS-II version Española-Colombia factor analysis had shown 3 factors: factor 1 “Sense of life” with 7 instruments, factor 2 “Lack of emotional control” with 7 instruments and factor 3 “Depressive symptomatology” with 2 instruments.22
A high correlation was found between the DS-II GR sub-scales and the overall HADS score, demonstrating criterion validity. There was a very strong relationship between demoralization and emotional distress-combined anxiety and depression.28The results of Española-Colombian study indicate that demoralization has within its structure components given by some depressive symptoms, but demoralization and depression are two distinct components In Robinson et al comorbidity between depression and demoralization existed at high levels of demoralization.1
Cronbach’s alpha was used indicating that the overall score and sub-scales had excellent internal consistency. In study by Robinson et al the Cronbach’s alpha index was equal to 0.89 for the overall score, 0.84 for factor 1, and 0.82 for factor 2.26Similar findings were found in the Spanish version of the DS II index, where Cronbach’s alpha was 0.88 for the overall score, 0.83 for factor 1, and 0.79 for factor 228 while Cronbach alpha index in DS-II Española-Colombian was 0.87 for total score, 0.75 for factor 1 and 0.78 for factor 2, 3. 22The test re-test reliability revealed no statistically significant differences. Accordingly, in Robinson et al the Intraclass Correlation Coefficient values for DS-II factor 1,2 and overall score were 0.68, 0.82, and 0.80 between the initial assessment and the reassessment.27 The coefficient values in Española-Colombian between the two repeated measurements for the total score were 0.56 and for factor 1: 0.55, factor 2: 0.46 and factor 3: 0.57.22 In the German version, DS-II related significantly with depression, anxiety, mental distress, and body image disturbance.29
Patients with a HAD anxiety score > 11 had higher score in “Meaning and Purpose”, “Discomfort” and overall scores, compared to patients with a score < 11. In contrast Robinson et al total score had moderate-strong positive correlations with burden, depression and desire to die. Psychological symptom burden had a higher correlation with “Distress and Coping Ability” than “Meaning and Purpose”.26 In a Spanish population there was a close relationship between demoralization and emotional distress while between depression and anxiety was less.28Thus, the factors that explain the demoralization scale and the overall score appear to be highly correlated with anxiety and depression scales assessing patients’ emotional states.
Conclusion
The Greek version of DS-II has shown to be valid, reliable and feasible with adequate psychometric properties in patients with cancer.
Acknowledgments
The authors did not receive any financial support in relation to the research, authorship, or publication of this article.
Authors’ Contribution
Conceptualization: Tania-Flora Elmasian.
Data curation: Maria Nikoloudi.
Formal analysis: Eleni Tsilika.
Investigation: Tania-Flora Elmasian.
Methodology: Tania-Flora Elmasian.
Project administration: Kyriaki Mystakidou.
Resources: Tania-Flora Elmasian, Sotiria Kostopoulou.
Supervision: Eleni Tsilika, Anna Zygogianni, Stylianos Katsaragakis.
Validation: Eleni Tsilika.
Visualization: Eleni Tsilika.
Writing–original draft: Tania-Flora Elmasian, Sotiria Kostopoulou.
Writing–review & editing: Sotiria Kostopoulou.
COI-statement
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data Availability
All the data generated or analyzed during this study have been incorporated within this published article.
Ethical Approval
Ethical approval and permission for this study was granted by the Aretaieion Ethics committee.
Funding
We do not have any funding.
Research Highlights
What is the current knowledge?
Demoralization has negative consequences for patients, jeopardizing the outcome of interventions and may be linked with wishes for hastened death.
What is new here?
This study demonstrates psychometric properties of DS-II GR in grease context which maintains internal consistency.
References
- Robinson S, Kissane DW, Brooker J, Burney S. A systematic review of the demoralization syndrome in individuals with progressive disease and cancer: a decade of research. J Pain Symptom Manage 2015; 49(3):595-610. doi: 10.1016/j.jpainsymman.2014.07.008 [Crossref] [ Google Scholar]
- Clarke DM, Kissane DW. Demoralization: its phenomenology and importance. Aust N Z J Psychiatry 2002; 36(6):733-42. doi: 10.1046/j.1440-1614.2002.01086.x [Crossref] [ Google Scholar]
- Hong YT, Lin YA, Pan YX, Lin JL, Lin XJ, Zhang J. Understanding factors influencing demoralization among cancer patients based on the bio-psycho-social model: a systematic review. Psychooncology 2022; 31(12):2036-49. doi: 10.1002/pon.6023 [Crossref] [ Google Scholar]
- Kissane DW, Clarke DM, Street AF. Demoralization syndrome--a relevant psychiatric diagnosis for palliative care. J Palliat Care 2001; 17(1):12-21. doi: 10.1177/082585970101700103 [Crossref] [ Google Scholar]
- Breitbart W, Rosenfeld B, Pessin H, Kaim M, Funesti-Esch J, Galietta M. Depression, hopelessness, and desire for hastened death in terminally ill patients with cancer. JAMA 2000; 284(22):2907-11. doi: 10.1001/jama.284.22.2907 [Crossref] [ Google Scholar]
- Chochinov HM. Dying, dignity, and new horizons in palliative end-of-life care. CA Cancer J Clin 2006; 56(2):84-103. doi: 10.3322/canjclin.56.2.84 [Crossref] [ Google Scholar]
- Kissane DW. Kissane DWPsychospiritual and existential distressThe challenge for palliative care. Aust Fam Physician 2000; 29(11):1022-5. [ Google Scholar]
- Kissane DW. Demoralization: a life-preserving diagnosis to make for the severely medically ill. J Palliat Care 2014; 30(4):255-8. doi: 10.1177/082585971403000402 [Crossref] [ Google Scholar]
- Frank J. The role of hope in psychotherapy. Int J Psychiatry 1968; 5(5):383-95. [ Google Scholar]
- Bobevski I, Kissane D, McKenzie D, Murphy G, Perera C, Payne I. The Demoralization Interview: reliability and validity of a new brief diagnostic measure among medically ill patients. Gen Hosp Psychiatry 2022; 79:50-9. doi: 10.1016/j.genhosppsych.2022.10.002 [Crossref] [ Google Scholar]
- Kissane DW, Wein S, Love A, Lee XQ, Kee PL, Clarke DM. The Demoralization Scale: a report of its development and preliminary validation. J Palliat Care 2004; 20(4):269-76. doi: 10.1177/082585970402000402 [Crossref] [ Google Scholar]
- Galiana L, Rudilla D, Oliver A, Barreto P. The Short Demoralization Scale (SDS): a new tool to appraise demoralization in palliative care patients. Palliat Support Care 2017; 15(5):516-23. doi: 10.1017/s1478951516000973 [Crossref] [ Google Scholar]
- Tang PL, Wang HH, Chou FH. A systematic review and meta-analysis of demoralization and depression in patients with cancer. Psychosomatics 2015; 56(6):634-43. doi: 10.1016/j.psym.2015.06.005 [Crossref] [ Google Scholar]
- Lai Q, Huang H, Zhu Y, Shu S, Chen Y, Luo Y. Incidence and risk factors for suicidal ideation in a sample of Chinese patients with mixed cancer types. Support Care Cancer 2022; 30(12):9811-21. doi: 10.1007/s00520-022-07386-8 [Crossref] [ Google Scholar]
- Jacobsen JC, Vanderwerker LC, Block SD, Friedlander RJ, Maciejewski PK, Prigerson HG. Depression and demoralization as distinct syndromes: preliminary data from a cohort of advanced cancer patients. Indian J Palliat Care 2006; 12(1):8-16. doi: 10.4103/0973-1075.25913 [Crossref] [ Google Scholar]
- Rudilla D, Oliver A, Galiana L, Barreto P. A new measure of home care patients’ dignity at the end of life: the Palliative Patients’ Dignity Scale (PPDS). Palliat Support Care 2016; 14(2):99-108. doi: 10.1017/s1478951515000747 [Crossref] [ Google Scholar]
- Angelino AF, Treisman GJ. Major depression and demoralization in cancer patients: diagnostic and treatment considerations. Support Care Cancer 2001; 9(5):344-9. doi: 10.1007/s005200000195 [Crossref] [ Google Scholar]
- de Figueiredo JM. de Figueiredo JMDemoralization and psychotherapy: a tribute to Jerome DFrank, MD, PhD (1909-2005). Psychother Psychosom 2007; 76(3):129-33. doi: 10.1159/000099839 [Crossref] [ Google Scholar]
- Dohrenwend BP, Dohrenwend BS, Levav I, Shrout P. The psychiatric epidemiology research interview. Harefuah 1981; 100(6):274-6. [ Google Scholar]
- Levitt EE. A structural analysis of the impact of MMPI-2 on MMPI-1. J Pers Assess 1990; 55(3-4):562-77. doi: 10.1207/s15327752jpa5503&4_13 [Crossref] [ Google Scholar]
- Cockram CA, Doros G, de Figueiredo JM. Diagnosis and measurement of subjective incompetence: the clinical hallmark of demoralization. Psychother Psychosom 2009; 78(6):342-5. doi: 10.1159/000235737 [Crossref] [ Google Scholar]
- Palacios-Espinosa X, Sánchez-Pedraza R, Rodríguez C. Psychometric properties of Demoralization Scale (DS-II Spanish version-Colombia) for oncologic patients in palliative care. Av Psicol Latinoam 2020; 38(3):84-101. doi: 10.12804/revistas.urosario.edu.co/apl/a.8408 [Crossref] [ Google Scholar]
- Boxley L, Flaherty JM, Spencer RJ, Drag LL, Pangilinan PH, Bieliauskas LA. Reliability and factor structure of the Hospital Anxiety and Depression Scale in a polytrauma clinic. J Rehabil Res Dev 2016; 53(6):873-80. doi: 10.1682/jrrd.2015.05.0088 [Crossref] [ Google Scholar]
- Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand 1983; 67(6):361-70. doi: 10.1111/j.1600-0447.1983.tb09716.x [Crossref] [ Google Scholar]
- Mystakidou K, Tsilika E, Parpa E, Katsouda E, Galanos A, Vlahos L. The Hospital Anxiety and Depression Scale in Greek cancer patients: psychometric analyses and applicability. Support Care Cancer 2004; 12(12):821-5. doi: 10.1007/s00520-004-0698-y [Crossref] [ Google Scholar]
- Robinson S, Kissane DW, Brooker J, Hempton C, Michael N, Fischer J. Refinement and revalidation of the demoralization scale: the DS-II-external validity. Cancer 2016; 122(14):2260-7. doi: 10.1002/cncr.30012 [Crossref] [ Google Scholar]
- Robinson S, Kissane DW, Brooker J, Michael N, Fischer J, Franco M. Refinement and revalidation of the demoralization scale: the DS-II-internal validity. Cancer 2016; 122(14):2251-9. doi: 10.1002/cncr.30015 [Crossref] [ Google Scholar]
- Belar A, Arantzamendi M, Rodríguez-Núñez A, Santesteban Y, Martinez M, López-Saca M. Multicenter study of the psychometric properties of the new Demoralization Scale (DS-II) in Spanish-speaking advanced cancer patients. J Pain Symptom Manage 2019; 57(3):627-34. doi: 10.1016/j.jpainsymman.2018.11.016 [Crossref] [ Google Scholar]
- Koranyi S, Hinz A, Hufeld JM, Hartung TJ, Quintero Garzón L, Fendel U. Psychometric evaluation of the German version of the Demoralization Scale-II and the association between demoralization, sociodemographic, disease- and treatment-related factors in patients with cancer. Front Psychol 2021; 12:789793. doi: 10.3389/fpsyg.2021.789793 [Crossref] [ Google Scholar]