Journal of caring sciences. 14(4):259-266.
doi: 10.34172/jcs.025.33176
Original Article
Development and Validation of Psychological Adaptation Tool (PAT) for Children with Chronic Illness
Shivani Singh Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Visualization, Writing – original draft, Writing – review & editing, 1, * 
Mukesh Chandra Sharma Formal analysis, Methodology, Project administration, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing, 2
Sanjeeta Dara Formal analysis, Methodology, Project administration, Resources, Supervision, Validation, 2
Author information:
1Paediatric Nursing, College of Nursing, All India Institute of Medical Sciences, Jodhpur, India
2College of Nursing, All India Institute of Medical Sciences, Jodhpur, India
Abstract
Introduction:
Children with chronic illnesses experience many difficulties in adapting to their conditions. A review of the literature indicates a lack of instruments to measure this concept. Therefore, the aim of this study was development and validation of psychological adaptation tool (PAT) for children with chronic illness.
Methods:
An exploratory mixed method design was used to develop and validate the PAT for children with chronic illness. The study was conducted in the paediatric OPD (outpatient department) and IPD (in patient department) at All India Institute of Medical Sciences, Jodhpur, and Rajasthan. It took place in three phases (phase one: item development, phase two: tool development, phase three: tool evaluation) and a final tool of 16 items, classified into four domains was made. The method of convenient sampling was used to select 160 study participants. The reliability was tested using Cronbach’s alpha. The construct validity of the tool was checked with exploratory factor analysis.
Results:
The results of study suggest that PAT is a valid and highly reliable tool. The content validity index was 0.96. The Cronbach’s alpha value for the entire 16 items of PAT was 0.850 which was found to be good. The principal component analysis yielded 4 factors (Cognitive, conative, self-efficacy and coping strategies) with an eigenvalue of more than 1.00.
Conclusion:
The result of this study has shown that PAT is a feasible highly reliable and valid tool.
Keywords: Chronic illness, Psychological adaptation, Tool, Children
Copyright and License Information
© 2025 The Author(s).
This work is published by Journal of Caring Sciences as an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/). Non-commercial uses of the work are permitted, provided the original work is properly cited.
Funding Statement
No funding was received for this study
Introduction
The concept of adaptation is omnipresent in psychology.1Adaptation is described as the ability to accept and respond to changes in the internal and external environment with the right attitude and behaviour.2
Piaget defined adaptation as a process through which children modify their actions, ideas, or plans in response to environmental changes in order to reach a condition of cognitive equilibrium.3 A chronic illness or medical condition is a health issue that impacts a child’s daily activities, lasts three months or more, and necessitates repeated hospitalisations, home health care, and/or intensive medical attention.4 In general, chronic diseases have at least three key characteristics: They are rarely fully curable, have a long duration, and do not resolve spontaneously.5
Psychological adaptation is a functional change in response to environmental stimuli, in terms of sensory functioning, behavior, cognition, or emotions.1,6-8 The theory of cognitive adaptation is based on the assumption that people possess unrealistically positive views of themselves to enhance their well-being.9,10
The emotional reaction to the diagnosis of a chronic illness can be a greater challenge than coping with the physical manifestations of the illness.11-14Children use various strategies to cope with the psychological stressors associated with chronic illness.15
Hospitalization is considered as most unfamiliar environment for children. Children experience psychosocial problems as a result of short and long-term impact of hospitalization.16,17 Children undergo a variety of unpleasant situations in addition to varied physical environments, such as painful procedures and the adverse effects of chemotherapy.18
The need of the study is that we hope to provide academic and practical researchers with a tool that allows them to explore new aspects of children’s well-being and improve their coping abilities, and, consequently, their health status. Children’s psychological adaptation is an area of study that’s yet to be explored. Measuring children’s psychological adaptation is an important endeavour, knowing the adaptation levels of the children can guide treatment, care, education, and counselling planning for optimum growth and development during their chronic illness period.19,20On other hand, parents were chosen as the instrument completers due to the uncooperativeness of the children with the defined age group. Therefore, the aim of this study was to development and validation of psychological adaptation tool (PAT) for children with chronic illness.
Material and Methods
An exploratory mixed method design was used to conduct the study. The PAT was developed in three phases. Figure 1 shows the schematic representation of the research.
Phase 1: Item Development Phase
This phase has two steps
1. Identification of Domain
Extensive Review of Literature
For the identification of domains, an extensive review of literature was carried out in order to explore the psychological adaptation of children with chronic illness. The review had been conducted from various journals, articles and other previous studies using the electronic databases PubMed, MEDLINE, CINHAL, Cochrane Library and Google Scholar. The areas focused in this review were related to the psychological adaptation children undergo who is suffering from chronic illness. The BOOLEAN operators, AND/OR was used for review, using the following:
Psychological adaptation AND Children
Psychological adaptation AND Chronic illness
Psychological adaptation AND Chronic illness AND children
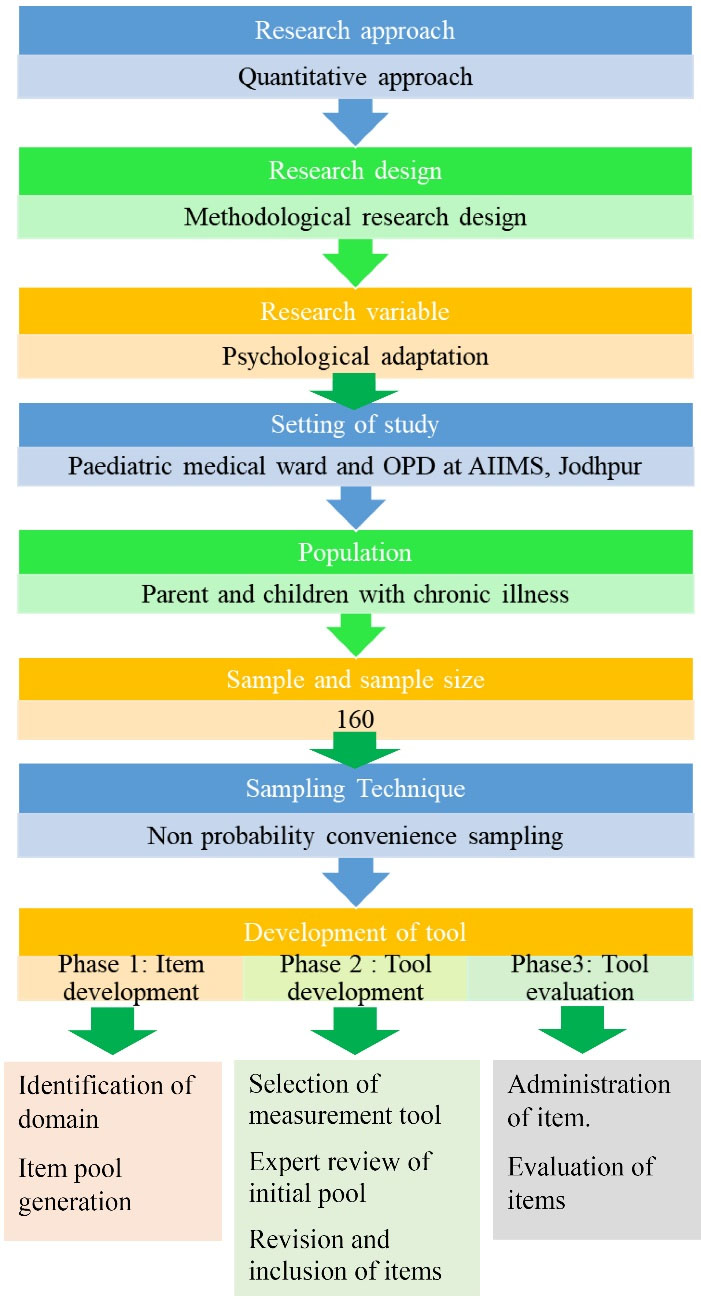
Figure 1.
Systematic representation of research methodology
.
Systematic representation of research methodology
Focused Group Discussion (FGD)
In order to develop the items, focused group discussion (unstructured) was conducted among two groups. One group consisted of 6 Pediatric doctors and 8 pediatric nurses working in pediatric medicine unit at AIIMS (All India Institute of Medical Sciences), Jodhpur and the other consisted of 10 parents whose children were suffering from chronic illness. Both FGDs were of about 30-35 minutes duration and the responses were noted.
The components of psychological adaptation of children with chronic illness obtained from the FGDs commonly included cognitive component which included about attention, learning, memory and concentration of the child. Other components included self-efficacy which included interaction of the child or relationship with others as a component of psychological adaptation to chronic illness in children. Participants also highlighted different coping mechanism usually used by the children.
2. Item Pool Generation
An item pool was generated which consisted of 4 domains, 14 subdomain and 29 items, generated based on the content that were identified through deductive and inductive methods via literature reviews and FGDs respectively. The items generated from literature review and FGDs were summarised domain wise in following manner in Table 1.
Phase 2: Tool Development
1.Selection of measurement scale
After the generation of the item pool list of opposite adjectives pairs in accordance with the statement were selected and a 5-point semantic differential tool was prepared based on which the participants selected the response that best represent the direction and intensity of their judgement about the adaptation of their child in last 6 months.
2. Expert Review of Initial Item Pool
The review of initial pool of items was done by the expert panel through the modified Delphi process. Two rounds of modified Delphi were conducted.
Stages of Delphi
Different stages are followed in the Delphi process:
Identification and Selection of Experts
The proper accomplishment of Delphi process depends mainly on the expert panel. Therefore, careful selection of experts should be made.
The Delphi panel for the present study consisted of 15 experts out of which 6 were from the field of paediatric nursing, 2 from the Department of Clinical and Child Psychology, and 7 from the Department of Psychiatry.
Table 1.
Summary of item pool generation
|
Domain/Sub-domain
|
Items
|
|
Cognitive domain
|
| Memory |
Is your child less efficient at remembering things now than he/she used to be? |
| Does your child misplace things more frequently now than he/she used to? |
| Does your child find it difficult to remember names of friends and relative? |
| Does your child remember the order of things in which any particular event occurred? |
| Attention |
Does your child get frequently distracted by the events around? |
| Learning |
Does your child show interest in learning new things? |
| Concentration |
Does your child jump from topic to topic in a conversation? |
| Does your child go from one assignment to another without completing them? |
| Conative |
Does your child interact less with other people around now? |
| Does your child share his/her concern about illness with you? |
| Does your child make friends easily? |
| Does your child have any difficulty with initiating or responding to conversation? |
| Does your child behave well with his/her sibling? |
| Is your child hopeful for positive outcome of treatment of his/her illness? |
| Does your child believe his/her illness is a kind of punishment? |
| Have you observed sudden mood change in your child because of illness? |
| Self-efficacy |
Does your child generally maintain an adequate diet? |
| Does your child take his/her prescribed medications? |
| Does your child look interested in grooming him/herself? |
|
|
Coping strategies
|
| Denial |
Does your child deny to accept his disease condition? |
| Fantasy |
Does your child say that superhero will come to save him? |
| Does your child enjoy playing with his/her toys more over any other activity? |
| Isolation |
Does your child prefer to stay alone? |
| Distortion |
Does your child only see negative in a situation than positive? |
| Repression |
Does your child share about the painful procedures after discharge or when at home? |
| Regression |
Does your child begin to suck their thumb or wet the bed when they need to spend some time in the hospital? |
| Displacement |
Does your child start hitting his toys when frustrated with the treatment procedures? |
| Temper tantrum |
Does your child show anger when asked for hospitalization? |
| Avoidance |
Does your child avoid talking about his disease condition? |
Sending Invitation to the Experts
The initial contact with the selected experts was made through mail in which a request letter was sent inviting them for the Delphi method along with the study title. Request letter was sent to 30 experts out of whom 21 had given the consent for participation. For those experts within the Institute, the correspondence was obtained through personal contact.
First Delphi Round
Once the confirmation mail was obtained, another email was sent to the experts consisting of the brief study methodology, preliminary draft of the tool and the evaluation criteria for validation of the tool, notifying them regarding the return of their suggestions to the same email id. Out of 21 experts to whom the draft was sent, 15 experts completed the first round. The first round was completed in three weeks.
Analysis of First Delphi Round Results
Once the response was obtained, the interpretation of the first round was done. The major areas of suggestion included merging of sub-domains, renaming of some domains and rephrasing of the sentences. The item related to thought (cognitive domain), global functioning (self-efficacy), repression and regression (defence mechanism) were considered irrelevant. Renaming of the domain defence mechanism as coping strategies was also suggested. Out of initial 11 items 8 items were considered as highly relevant by all validators and 3 needed modifications. Also, out of 29 items, 7 items were considered highly significant, 5 items were rephrased, 9 were merged and 8 were considered as irrelevant by the majority of validators and therefore removed.
After interpretation of expert’s suggestion from first Delphi round, first modification was made in the initial draft of tool with 29 items. Items were reviewed and revised. Further, the revised items were rearranged by assigning them to appropriate categories. The revision of initial draft was made in manner as given in Table 2.
Second Delphi Round
Invitation for the second round was sent to only those who completed the first round and feedback of first round was also sent along with the modified tool. Out of 15 experts to whom the feedback of first round was sent, 9 completed the second round. It took 2 weeks to complete the second round.
Analysis of Delphi Round Second Results
After obtaining the responses from the validators, interpretation of second round was done. There were no suggestions for section A. for section B suggestions regarding removal of items 2, 8, 15, 17, 18, 19, 21 and 26 from initial draft were accepted by validators along with merging of items. Final 16 item tool with opposite adjective pairs after Delphi modification (Table 2).
Revision and Inclusion of Items
After the expert’s review of initial item pool, the tool consists of 4 domains (cognitive, conative, self-efficacy and coping strategies) with 10 subdomains (Attention, Learning, Memory, Concentration, Interaction, Denial, Isolation, Temper tantrums, Distortion, Fantasy) and 16 items. The S-CVI/ Ave and S- CVI/UA were 0.96 and 0.87 respectively. This shows good content validity.
Phase 3: Tool Evaluation
Administration of the Items to the Subjects
The final modified draft of tool consisting of 16 items that were evolved through literature review, content validation by experts, and the study was then administered to 160 parents of children with chronic illness in the study setting at AIIMS, Jodhpur, in order to test the validity and reliability. Researcher has taken the ethical approval for the current study from the institutional ethical committee. The process of data collection explained to the subjects (parents) and a written informed consent obtained from them. Confidentiality regarding the data was assured so as to get cooperation throughout the procedure of data collection. Data were collected using PAT in Hindi language and only from those who fulfil the inclusion criteria. Parents were asked to fill the 5point semantic differential tool of PAT, ranging from 1-5, with their responses between two opposite adjective pairs. The method of administration was pen and paper method. Confidentiality and anonymity of the responses maintained throughout the study.
For Reliability analysis of the PAT Cronbach alpha was calculated, to find out the internal consistency of the tool.
Exploratory factor analysis was done to find out construct validity. Principal component matrix was used to normalize the sets of data. The appropriateness of PAT was checked by Kaiser–Meyer–Olkin (KMO) test and the Bartlett test of sphericity by using Statistical Package for the Social Sciences (SPSS, version 22).
Results
Evaluation of the Items
Reliability Analysis for the PAT
The Cronbach alpha was calculated to find out the internal consistency of the tool. The Cronbach alpha value was 0.814 for the entire 16 items, which was found to be good.
Since the value of Cronbach’s alpha of scale increase on deletion of item 6, this item can be removed from the tool, but after discussing with the experts and considering the importance of the item it was decided to retain it.
Construct Validity Analysis for the PAT
The KMO value of the PAT was 0.886 and Bartlett’s test of sphericity shows P value of < 0.001 with a χ2 value of 586.418, which was significant. These values show the adequacy of the sample for factor analysis.
To find out the extraction communality of each item of the tool, principal component analysis method was instituted. The initial communality of each item was assured to be 1 (100%). For the PAT, extraction communality of the item was in between 0.322-0.670 (Table 3). Hence, this data was appropriate for factor analysis.
Table 4 shows total variance of the item extracted through principal component analysis. Factor extraction condenses the item into smaller number of items and is used to identify the number of underlying dimensions. Principal component analysis method was used for the extraction of factors for PAT. Principal component analysis had generated 4 factors (cognitive, conative, self-efficacy and coping strategies). The Eigen value of all the 4 factors was above 1.00. Here the principal component analysis had showed the first four factors account for 51.0% of the total variance.
Figure 2 illustrates the scree plot for the four-factor structure for the PAT. Since there is considerable discontinuity after 4th component with Eigen value of less than 1.00, four factors could be extracted.
Table 5 depicts the Rotated Component Matrix of PAT through varimax rotation. Once the factors were extracted through principal component analysis was done with Varimax with Kaiser Normalization.
The first factor had an initial acceptable loading of 7 items (Item- 1, 5, 10, 12, 13, 14, 15) (range, 0.474-0.690) accounted for 30.34% of variance with Eigenvalue of 4.85. The second factor evidenced loading of 4 items out of which 3 were retained (Item- 2, 3, 4) (range, 0.419-0.806) and accounted for 7.60 % of variance with Eigenvalue of 1.21. The third factor was loaded with 3 items (Item 7, 9, 16) (range, 0.475-0.722) and accounted for 6.78% of variance and Eigenvalue of 1.086. The fourth factor evidenced acceptable loading from 3 items (Item-6, 8, 11) (range-0.533-0.631) and accounted for 6.26% of variance with an Eigenvalue of 1.00.
A factor loading of 0.4 was considered as the criteria for acceptable loading.21 Also the items were retained within the factor in which they had higher factor loading.22,23 The four factors were cognitive, conative, self-efficacy and coping strategies.
Table 2.
Summary of the modification of the tool
|
Old items
|
Items after first modification
|
Items after second modification
|
| Your child at remembering things (attentive-in attentive) |
How does your child look while doing work? (Attentive-inattentive) rephrased. |
How does your child look while doing work? (Attentive-inattentive) |
| Your child misplaces things (more frequently-less frequently) |
Removed |
|
| How does your child remember names of friends and relatives (recall easily-face difficulty) |
How does your child remember names of friends and relatives (recall easily-face difficulty) |
How does your child remember names of friends and relatives? (Recall easily-face difficulty) |
| Your child at remembering things (efficient- non efficient) |
How does your child remember things (efficiently-non efficiently)? rephrased |
How does your child remember things? (Efficiently-non efficiently) |
| What your child does when in a conversation (concentrated-distracted) |
What your child does when in a conversation? (Stick to the particular topic-jump from one topic to other) item 5 and 7 merged |
What your child does when in a conversation? (Stick to the particular topic-jump from one topic to other) |
| What is your child reaction while learning new things (curious-incurious). |
What is your child reaction while learning new things? (Curious-incurious). |
What is your child reaction while learning new things? (Curious-incurious). |
| Your child jump from topic to topic in a conversation (Never- sometimes) |
See item 5 |
|
| Does your child go from one assignment to another without completing them (frequently-never) |
Removed |
|
| Your child while interacting to others look (interested-indifferent) |
How does your child look while interacting with others? (Interested-indifferent) rephrased |
How does your child look while interacting with others? (Interested-indifferent) |
| What is your child reaction after any painful procedure? (Share his/her feelings- avoid talking much) |
What is your child reaction after any panful procedure? (Share his/her feelings- avoid talking much) |
What is your child reaction after any painful procedure? (Share his/her feelings- avoid talking much) |
| What is your child behaviour towards you (friendly-unfriendly) |
What is your child behaviour towards other (friendly-unfriendly) item 11,12,13 merged |
What is your child behaviour towards other? (Friendly-unfriendly) |
| Does your child have any difficulty with initiating or responding to conversation |
See item 11 |
|
| Does your child behave well with his/her sibling |
See item 11 |
|
| Is your child hopeful for positive outcome of treatment of his/her illness |
Your child perspective towards life (positive - negative) item 14 and 24 merged |
Your child perspective towards life? (Positive - negative) |
| Does your child believe his/her illness is a kind of punishment |
Removed |
|
| Your child mood most of the time (steady-unstable) |
Your child mood most of the time (steady-unstable) |
Your child mood most of the time? (Steady-unstable) |
| Does your child generally maintain an adequate diet |
Removed |
|
| Does your child take his/her prescribed medications |
Removed |
|
| Does your child look interested in grooming him/herself |
Removed |
|
| Your child when you ask about his/her illness (accept the illness-deny his illness) |
What is your child reaction when you ask about his/her illness? (Accept his/her illness-deny his/her illness) rephrased |
What is your child reaction when you ask about his/her illness? (Accept his/her illness-deny his/her illness) |
| Does your child say that superhero will come to save him |
Removed |
|
| Does your child enjoy playing with his/her toys more over any other activity (never-always) |
Your child spends most of the time living in (reality -fantasy) rephrased |
Your child spends most of the time living in? (Reality -fantasy) |
| Most of the time your child prefers to stay (socialized-isolated) |
How does your child prefer to stay? (Socialised-isolated) rephrased |
How does your child prefer to stay? (Socialised-isolated) |
| Does your child only see negative in a situation than positive (always-never) |
See item 14 |
|
| Does your child share about the painful procedures after discharge or when at home (often-sometimes) |
Your child reaction after any painful procedure (share feeling-avoid talking much) rephrased |
Your child reaction after any painful procedure (share feeling-avoid talking much) |
| Does your child begin to suck their thumb or wet the bed when they need to spend some time in the hospital |
Removed |
|
| Does your child start hitting his toys when frustrated with the treatment procedures |
What is your child reaction when asked for hospitalization (does not react much- show anger/tantrums) item 27 and 28 merged |
What is your child reaction when asked for hospitalization (does not react much- show anger/tantrums) |
| Does your child show anger when asked for hospitalization |
See item 27 |
|
| How does your child behave when you talk about his/her illness (courteous-rude) |
How does your child behave when you talk about his/her illness (courteous-rude) |
How does your child behave when you talk about his/her illness (courteous-rude) |
Scoring Of Psychological Adaption Tool
The scoring of the tool was divided into five parts with score of 16 being not at all adaptable, score of > 16-32 being a little bit adaptable, > 32-48 somewhat adaptable, > 48-64 as quite a bit adaptable and > 64 as very much adaptable.
Discussion
In this study to assess the psychological adaptation of children with chronic illness a 16-item, 5-point semantic differential tool was prepared. Through literature review it was evidenced that the previously developed adaptation tool are all Likert type.24 The reason behind selecting the semantic differential scale was that it tends to produce more accurate results than Likert scale and offer the participant a bipolar adjective pair which makes it easy to respond.25 The PAT developed in three phases: item development, tool development and tool evaluation through seven steps. Similar methodology was used in other studies from the literature.26,27 The final items were compiled by reviewing the literature, conducting semi-structured interviews and Delphi process.
The study unequivocally emphasizes the significance of assessing psychological adaptation in children with chronic illnesses, which is consistent with previous study finding regarding the importance of assessing psychological adaptation.15,24 Additionally, the study discusses the need of taking into account the psychological component, which is more frequently disregarded, in children who are living with chronic disease and also the lack of tools for assessing psychological adaptation in paediatric population.
Four domains were identified to measure the psychological adaptation with PAT those were cognitive, conative, self-efficacy and coping strategies. Studies looking at illness-related coping methods also showed that children with chronic illnesses used cognitive adaption techniques more frequently.28
Although the PAT represents an important methodological advance in the area of children’s psychological adaptation, its limitations must be recognized. First, research findings cannot be generalized as only single setting was selected for conducting the study also age group of the study subject was school age i.e., 6 to 12 years and thus not applicable to all paediatric age groups.
Table 3.
Extraction communality of items through principal component analysis
|
|
Initial
|
Extraction
|
| Item 1 |
1.000 |
0.571 |
| Item 2 |
1.000 |
0.627 |
| Item 3 |
1.000 |
0.604 |
| Item 4 |
1.000 |
0.670 |
| Item 5 |
1.000 |
0.444 |
| Item 6 |
1.000 |
0.504 |
| Item 7 |
1.000 |
0.489 |
| Item 8 |
1.000 |
0.494 |
| Item 9 |
1.000 |
0.531 |
| Item 10 |
1.000 |
0.540 |
| Item 11 |
1.000 |
0.322 |
| Item 12 |
1.000 |
0.374 |
| Item 13 |
1.000 |
0.468 |
| Item 14 |
1.000 |
0.414 |
| Item 15 |
1.000 |
0.611 |
| Item 16 |
1.000 |
0.495 |
Table 4.
Total variance of the items extracted through principal component analysis
|
Component
|
Initial eigenvalues
|
Extraction sums of squared loadings
|
Rotation sums of squared loadings
|
|
Total
|
% Of variance
|
Cumulative %
|
Total
|
% Of variance
|
Cumulative %
|
Total
|
% Of variance
|
Cumulative %
|
| 1 |
4.855 |
30.346 |
30.346 |
4.855 |
30.346 |
30.346 |
2.934 |
18.335 |
18.335 |
| 2 |
1.217 |
7.607 |
37.953 |
1.217 |
7.607 |
37.953 |
2.006 |
12.538 |
30.874 |
| 3 |
1.086 |
6.785 |
44.738 |
1.086 |
6.785 |
44.738 |
1.716 |
10.728 |
41.602 |
| 4 |
1.002 |
6.264 |
51.002 |
1.002 |
6.264 |
51.002 |
1.504 |
9.400 |
51.002 |
| 5 |
0.952 |
5.947 |
56.949 |
|
|
|
|
|
|
| 6 |
0.920 |
5.749 |
62.698 |
|
|
|
|
|
|
| 7 |
0.862 |
5.390 |
68.088 |
|
|
|
|
|
|
| 8 |
0.817 |
5.108 |
73.196 |
|
|
|
|
|
|
| 9 |
0.720 |
4.499 |
77.695 |
|
|
|
|
|
|
| 10 |
0.669 |
4.182 |
81.876 |
|
|
|
|
|
|
| 11 |
0.632 |
3.947 |
85.824 |
|
|
|
|
|
|
| 12 |
0.576 |
3.598 |
89.422 |
|
|
|
|
|
|
| 13 |
0.486 |
3.040 |
92.461 |
|
|
|
|
|
|
| 14 |
0.465 |
2.907 |
95.368 |
|
|
|
|
|
|
| 15 |
0.379 |
2.371 |
97.740 |
|
|
|
|
|
|
| 16 |
0.362 |
2.260 |
100.000 |
|
|
|
|
|
|
Table 5.
Rotated component matrix of the items extracted through principal component analysis
|
|
Component
|
|
1
|
2
|
3
|
4
|
| Item 1 |
0.556 |
0.419 |
|
|
| Item 2 |
|
0.526 |
|
|
| Item 3 |
|
0.623 |
|
|
| Item 4 |
|
0.806 |
|
|
| Item 5 |
0.582 |
|
|
|
| Item 6 |
|
|
|
0.631 |
| Item 7 |
|
|
0.671 |
|
| Item 8 |
|
|
|
0.621 |
| Item 9 |
|
|
0.722 |
|
| Item 10 |
0.690 |
|
|
|
| Item 11 |
|
|
|
0.533 |
| tem 12 |
0.549 |
|
|
|
| Item 13 |
0.614 |
|
|
|
| Item 14 |
0.474 |
|
|
|
| Item 15 |
0.633 |
|
|
|
| Item 16 |
|
|
0.475 |
|
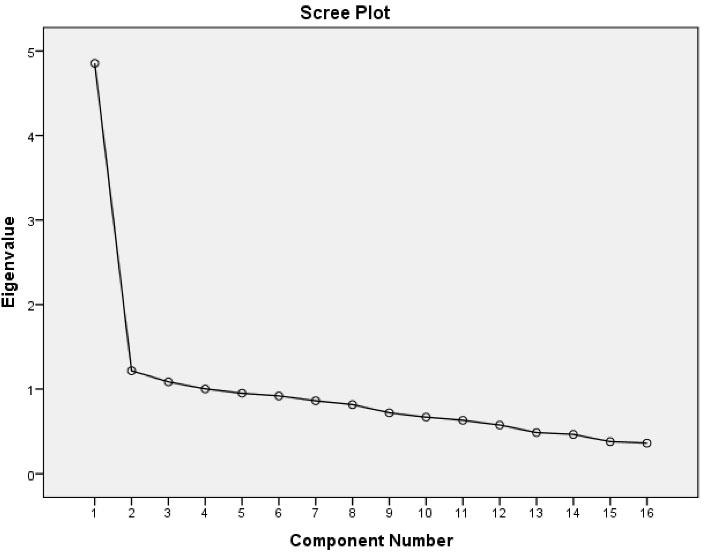
Figure 2.
Scree plot for the four-factor structure for the PAT
.
Scree plot for the four-factor structure for the PAT
Conclusion
In conclusion, result of this study has shown that PAT is a feasible, highly reliable and valid tool to measure the psychological adaptation in children with chronic illness and thus can be used to assess the psychological adaptation level. It accords towards the need for further more research into the measurement of the psychological adaptation since it is an important aspect to consider in children who are suffering from the chronic illness. Therefore, by paying attention to the psychological adaptation level doctors and nurses can provide high quality paediatric health care services for children.
Competing Interests
There is no conflict of interest in the study.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Ethical Approval
Ethical clearance was obtained from the institutional ethical committee of the with reference number: AIIMS/IEC/2022/4061. Informed written consent was taken from the study subjects after giving proper explanation of the purpose of the study. Confidentiality and anonymity of the subjects and the data collected were maintained throughout the study.
Research Highlights
What is the current knowledge?
-
Currently there has been no such tool like PAT (Psychological adaption tool) for children.
-
While treating the physical symptoms the “psychological adaptation” aspect is often ignored in children who are suffering from chronic illness.
What is new here?
-
First structured tool focused on assessing psychological adaptability in children with chronic illness.
-
Can be used as a screening tool in pediatric clinics, schools or counselling centers.
-
Help identify children with poor adaptability and support them.
-
Applicable in pediatric medicine, child psychiatry, psychology and community health.
Acknowledgements
I extend my gratefulness towards all the study participants, for their cooperation and devotion of time during each phase of my study process, without which it might not have been possible to reach the goal of this study. I would also like to appreciate the help and assistance offered by all the staff of Paediatric Ward of AIIMS Jodhpur.
Words are not enough to express my sincere appreciation to my guide, Dr. Mukesh Chandra Sharma, Associate Professor, College of Nursing. AIIMS Jodhpur, who had convincingly encouraged and guided me throughout this endeavour, without whose persistent support, this work would not have been completed. I am also deeply grateful to my co-guides Mrs. Sanjeeta Dara for her constant encouragement and insightful suggestions.
References
- Bjorklund DF. Developing adaptations. Dev Rev 2015; 38:13-35. doi: 10.1016/j.dr.2015.07.002 [Crossref] [ Google Scholar]
- Atik D, Karatepe H. Scale development study: adaptation to chronic illness. Acta Med Mediterr 2016; 32(1):135-42. doi: 10.19193/0393-6384_2016_1_21 [Crossref] [ Google Scholar]
- Piaget J. Piaget’s theory. In: Inhelder B, Chipman HH, Zwingmann C, eds. Piaget and His School: A Reader in Developmental Psychology. Berlin, Heidelberg: Springer; 1976. p. 11-23. 10.1007/978-3-642-46323-5_2
- Mokkink LB, van der Lee JH, Grootenhuis MA, Offringa M, Heymans HS. Defining chronic diseases and health conditions in childhood (0-18 years of age): national consensus in the Netherlands. Eur J Pediatr 2008; 167(12):1441-7. doi: 10.1007/s00431-008-0697-y [Crossref] [ Google Scholar]
- Stanton AL, Revenson TA, Tennen H. Health psychology: psychological adjustment to chronic disease. Annu Rev Psychol 2007; 58:565-92. doi: 10.1146/annurev.psych.58.110405.085615 [Crossref] [ Google Scholar]
- Roberts MC. Handbook of Pediatric Psychology. 3rd ed. New York: Guilford Press; 2003. p. 772.
- Dennis M, Simic N, Bigler ED, Abildskov T, Agostino A, Taylor HG. Cognitive, affective, and conative theory of mind (ToM) in children with traumatic brain injury. Dev Cogn Neurosci 2013; 5:25-39. doi: 10.1016/j.dcn.2012.11.006 [Crossref] [ Google Scholar]
- Lazarus RS. Coping with the stress of illness. WHO Reg Publ Eur Ser 1992; 44:11-31. [ Google Scholar]
- Samson A, Siam H. Adapting to major chronic illness: a proposal for a comprehensive task-model approach. Patient Educ Couns 2008; 70(3):426-9. doi: 10.1016/j.pec.2007.10.018 [Crossref] [ Google Scholar]
- Taylor SE. Adjustment to threatening events: a theory of cognitive adaptation. Am Psychol 1983; 38(11):1161-73. doi: 10.1037/0003-066x.38.11.1161 [Crossref] [ Google Scholar]
- Aspinwall LG, Taylor SE. Modeling cognitive adaptation: a longitudinal investigation of the impact of individual differences and coping on college adjustment and performance. J Pers Soc Psychol 1992; 63(6):989-1003. doi: 10.1037//0022-3514.63.6.989 [Crossref] [ Google Scholar]
- Samson A, Siam H, Lavigne R. Psychosocial adaptation to chronic illness: description and illustration on an integrated task-based model. Interventions. 2007(127): 16-28.
- Turner J, Kelly B. Emotional dimensions of chronic disease. West J Med 2000; 172(2):124-8. doi: 10.1136/ewjm.172.2.124 [Crossref] [ Google Scholar]
- Telford K, Kralik D, Koch T. Acceptance and denial: implications for people adapting to chronic illness: literature review. J Adv Nurs 2006; 55(4):457-64. doi: 10.1111/j.1365-2648.2006.03942.x [Crossref] [ Google Scholar]
- Nair D, Bonnet K, Wild MG, Umeukeje EM, Fissell RB, Faulkner ML, et al. Psychological adaptation to serious illness: a qualitative study of culturally diverse patients with advanced chronic kidney disease. J Pain Symptom Manage 2021; 61(1): 32-41.e2. 10.1016/j.jpainsymman.2020.07.014
- Robb SL. The effect of therapeutic music interventions on the behavior of hospitalized children in isolation: developing a contextual support model of music therapy. J Music Ther 2000; 37(2):118-46. doi: 10.1093/jmt/37.2.118 [Crossref] [ Google Scholar]
- Crnković M, Divcić B, Rotim Z, Corić J. Emotions and experiences of hospitalized school age patients. Acta Clin Croat 2009; 48(2):125-35. [ Google Scholar]
- Kirkby RJ, Whelan TA. The effects of hospitalisation and medical procedures on children and their families. J Fam Stud 1996; 2(1):65-77. doi: 10.5172/jfs.2.1.65 [Crossref] [ Google Scholar]
- Hampel P, Rudolph H, Stachow R, Laß-Lentzsch A, Petermann F. Coping among children and adolescents with chronic illness. Anxiety Stress Coping 2005; 18(2):145-55. doi: 10.1080/10615800500134639 [Crossref] [ Google Scholar]
- Gajdošová E, Janičová J. Social-emotional health and psychological well-being among church school students. Acta Educ Gen 2021; 11(2):19-30. doi: 10.2478/atd-2021-0010 [Crossref] [ Google Scholar]
- Floyd FJ, Widaman KF. Factor analysis in the development and refinement of clinical assessment instruments. Psychol Assess 1995; 7(3):286-96. doi: 10.1037/1040-3590.7.3.286 [Crossref] [ Google Scholar]
- Bishnoi AK. Review of the steps for development of quantitative research tools. J Adv Pract Nurs 2015; 1(1):103. doi: 10.4172/apn.1000103 [Crossref] [ Google Scholar]
- Agius RM, Blenkin H, Deary IJ, Zealley HE, Wood RA. Survey of perceived stress and work demands of consultant doctors. Occup Environ Med 1996; 53(4):217-24. doi: 10.1136/oem.53.4.217 [Crossref] [ Google Scholar]
- Biesecker BB, Erby LH, Woolford S, Adcock JY, Cohen JS, Lamb A. Development and validation of the Psychological Adaptation Scale (PAS): use in six studies of adaptation to a health condition or risk. Patient Educ Couns 2013; 93(2):248-54. doi: 10.1016/j.pec.2013.05.006 [Crossref] [ Google Scholar]
- Friborg O, Martinussen M, Rosenvinge JH. Likert-based vs. semantic differential-based scorings of positive psychological constructs: a psychometric comparison of two versions of a scale measuring resilience. Pers Individ Dif 2006; 40(5):873-84. doi: 10.1016/j.paid.2005.08.015 [Crossref] [ Google Scholar]
- Boateng GO, Neilands TB, Frongillo EA, Melgar-Quiñonez HR, Young SL. Best practices for developing and validating scales for health, social, and behavioral research: a primer. Front Public Health 2018; 6:149. doi: 10.3389/fpubh.2018.00149 [Crossref] [ Google Scholar]
- Kim CH, Kang KA. The validity and reliability of the Healthy Lifestyle Screening Tool. Phys Ther Rehabil Sci 2019; 8(2):99-111. doi: 10.14474/ptrs.2019.8.2.99 [Crossref] [ Google Scholar]
- Knapp PK, Harris ES. Consultation-liaison in child psychiatry: a review of the past 10 years. Part I: clinical findings. J Am Acad Child Adolesc Psychiatry 1998; 37(1):17-25. doi: 10.1097/00004583-199801000-00012 [Crossref] [ Google Scholar]