Journal of caring sciences. 14(3):165-172.
doi: 10.34172/jcs.025.33325
Original Article
Psychometric Evaluation of Indonesian Version of the Somatic Symptom Scale-8 (ISSS-8)
I Made Moh. Yanuar Saifudin Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Project administration, Validation, Visualization, Writing – original draft, Writing – review & editing, 1 
Ananda Prastuti Sutrisno Data curation, Funding acquisition, Investigation, Project administration, Resources, Writing – review &
editing, 2
Sri Warsini Formal analysis, Funding acquisition, Methodology, Project administration, Validation, Writing – review & editing, 3
Intansari Nurjannah Funding acquisition, Project administration, Supervision, Writing – original draft, Writing – review & editing, 3, *
Author information:
1Department of Nursing, Faculty of Medicine, Universitas Tanjungpura, Pontianak, Indonesia
2Faculty of Medicine, Public Health, and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia
3Department of Mental Health and Community Nursing, Faculty of Medicine, Public Health, and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia
Abstract
Introduction:
Somatic symptom disorders (SSDs) refer to a group of patients experiencing distressing physical symptoms accompanied by excessive thoughts, feelings, or behaviors related to these symptoms. SSDs are associated with various medical and psychiatric conditions, leading to significant healthcare costs. Therefore, early identification and intervention for SSD are crucial. The Somatic Symptom Scale-8 (SSS-8) is an efficient and valuable self-report instrument for assessing the burden of somatic symptoms. Therefore, this study has two main objectives; Firstly, translating the SSS-8 to suit the Indonesian population by creating the Indonesian version, known as ISSS-8, and secondly, comprehensively assessing the psychometric characteristics of the ISSS-8.
Methods:
The SSS-8 items was translated into Bahasa Indonesian using WHO translation method and produced ISSS-8. The second phase involved evaluating the scale’s psychometric properties, including construct validity and reliability. Confirmatory factor analysis (CFA) and Cronbach alpha testing was performed.
Results:
The Cronbach's alpha outcomes affirmed the reliability of ISSS-8 with score of α=0.627. Additionally, CFA confirmed the singular-factor structure of SSS-8 with fit model (χ2/df=0.126, CFI=0.957, GFI=0.881, RMSEA=0.053, and SRMR=0.054).
Conclusion:
The ISSS-8 proved to be a valid and reliable instrument for evaluating somatic symptoms in the adult population. It exhibited acceptable validity and reliability, consistent with prior research conducted in diverse cultural settings. These results affirm the effectiveness of ISSS-8 as a valuable screening tool for identifying somatic symptoms within the Indonesian-speaking population.
Keywords: Indonesia, Somatic symptoms, Somatic symptom scale-8, Surveys and questionnaires, Validation study
Copyright and License Information
© 2025 The Author(s).
This work is published by Journal of Caring Sciences as an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/). Non-commercial uses of the work are permitted, provided the original work is properly cited.
Funding Statement
This study was funded by Final Project Recognition Grant of Universitas Gajah Mada (Ref. Number: 656/UN1.PII/KPT/HUKOR/2023).
Introduction
The fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) has modified the diagnostic classification previously recognized as somatoform and related disorders to now be referred to as somatic symptom and related disorders (SSDs).1 According to American Psychiatric Association, SSD is a “DSM-5 diagnosis that describes a cluster of patients who have distressing somatic symptoms along with excessive thoughts, feelings, or behaviors related to these symptoms.2 SSD is an umbrella term intended to describe most of the patients who had previously held the diagnoses of somatization disorder, pain disorder, and hypochondriasis, which appeared in the DSM-IV chapter on somatoform disorders.” This revision has fundamentally altered the definition of SSDs.3
The prevalence of SSDs varies across different populations and settings. Research indicates that in Taiwan, the prevalence of SSDs is 5.0%,4 while in China, it is 63.2% among the elderly and 45.3% among the non-elderly.5 In Oman, the rate is 17.8%,6 in the Kingdom of Saudi Arabia, it stands at 39%,7 and in Palestine, it is 32.5%.8 Ultimately, a previous scoping review of general population studies using self-report questionnaires found an average prevalence of SSDs to be 12.9%.9
SSDs are shared across diverse medical conditions, serving as indicators in diagnostic evaluations and treatment monitoring.10 SSDs are associated with low quality of life, heightened psychological distress, and increased healthcare utilization. These symptoms manifest in conditions like cancer, coronary heart disease, and psychiatric disorders such as depression and anxiety.11 Studies suggest that SSDs often cluster into four groups including pain, cardiopulmonary, gastrointestinal, and general symptoms.12
Various methods, such as self-report surveys, can identify the somatic symptoms associated with this disorder. Among the commonly employed scales for evaluating the presence and intensity of typical SSDs is the Patient Health Questionnaire-15 (PHQ-15).12,13 Furthermore, the Somatic Symptom Scale-8 (SSS-8) was created to facilitate the evaluation of the disease status in SSDs.14 Several studies have demonstrated the favorable item characteristics and outstanding reliability of the SSS-8 in diverse clinical contexts,15-17 and across different countries.17-20 Additionally, research has indicated that its psychometric properties are equivalent to those of the PHQ-15.14,15
The SSS-8 has been evaluated against other scales, such as the PHQ-15, for detecting SSD, showing favorable outcomes when used alongside other assessment tools.15,21 Compared to previous tools, SSS-8 is an efficient 8-item scale that succinctly captures somatic symptoms, making it more practical and easier to administer in clinical settings compared to other tools.22 This brevity enhances its usability for assessing somatic symptom burden.23,24 The SSS-8 includes validated cutoff values, allowing researchers to classify individuals into various levels of somatic symptom burden, from mild to very high.23
For individuals with SSDs, efforts to address somatic symptoms and psychological issues through pharmacotherapy and psychotherapy have been made.25 Despite these efforts, functional somatic symptoms in these patients often persist for more than six months,1 particularly in severe cases.26,27 Careless examinations or diagnostic procedures by healthcare providers can lead to iatrogenic consequences if an illness is missed, resulting in significant financial burdens on the healthcare system. Patients with undiagnosed pain may find themselves in difficult situations as they continue to seek medical services. The quality of early caregiving experiences has long-lasting effects on somatic well-being, with childhood trauma and negative interactions with primary caregivers potentially leading to somatic symptoms in adolescence. Therefore, it is crucial for healthcare professionals to be aware of these risks and collaborate to reduce the occurrence of iatrogenic harm.9,28,29
Therefore, screening individuals with SSD to determine prevalence and enhance intervention strategies would be beneficial. In busy clinical environments, the SSS-8 could be a more practical screening tool, especially for identifying severe cases. Its brevity, with only 8 items, makes the SSS-8 quick and easy to administer, reducing the burden on both patients and healthcare providers. This efficiency enables rapid completion during consultations without consuming excessive time, supporting informed decision-making due to its proven reliability in clinical settings. Previous research has highlighted the SSS-8 as a concise and valuable instrument for assessing common somatic symptoms in clinical settings. However, the SSS-8 has not been validated in Indonesia. Thus, this study has two main objectives: Firstly, translating the SSS-8 to suit the Indonesian population by creating the Indonesian version, known as ISSS-8, and secondly, comprehensively assessing the psychometric characteristics of the ISSS-8.
Materials and Methods
A cross-sectional study was conducted in Yogyakarta, Indonesia, employing a two-phase approach. The first phase involved the translation of the SSS-8 to create the ISSS-8, while the second phase focused on administering psychometric testing on the ISSS-8. Convenience sampling methods was used to select the participants.
The study population was selected from a community-based environment in Yogyakarta city, the capital of the Special Region of Yogyakarta Province, located in central Java Island, Indonesia. The study participants recruited during a community health screening program conducted by the Faculty of Medicine, Universitas Gadjah Mada, as part of their regular community outreach services. Upon arrival at the event, participants were screened for eligibility: They had to be 18 years or older, capable of understanding and reading Bahasa Indonesia, and willing to participate. Individuals with diagnosed psychiatric disorders (including depression, anxiety disorders), chronic medical conditions (such as diabetes mellitus, hypertension, and cardiovascular diseases), acute medical conditions requiring ongoing treatment, or those currently taking psychotropic medications were excluded. To identify diseases among the participants, the study implemented a thorough screening process during the health community services event. Participants completed a medical history screening, which included questions about past and present physical and mental health conditions, ongoing treatments, and medications.
Kyriazos30 suggested a recommended ratio of 20:1 between the number of participants and items for confirmatory factor analysis (CFA). Consequently, with the ISSS-8 comprising 8 items, a minimum sample size of 160 participants was determined for this study. Additionally, 30 participants were included in the instrument pre-testing phase.
The SSS-8 is a concise version comprising 8 items adapted from the PHQ-15.14,31 The PHQ-15 assesses the presence and intensity of common SSDs and is widely recognized as one of the most extensively used and well-validated self-report instruments for gauging the burden of SSDs. Originally designated as the PHQ-SSS in the DSM-5 field trials, the scale was later renamed to SSS-8 to streamline the name and correspond to the number of items.32
The SSS-8 was developed as part of the DSM-5 field trials to provide a brief assessment tool for the newly introduced SSDs. To simplify the scale, certain PHQ-15 items pertaining to menstrual problems, sexual problems, and fainting were excluded due to low communalities, symptom prevalence, and associations with functioning, quality of life, and healthcare use. Additionally, PHQ-15 items related to gastrointestinal and cardiovascular symptoms were combined into 2 new items. The SSS-8 utilizes a 5-point response option (0-4) for each item. It adopts a 7-day time frame, deviating from the 4-week time frame of the PHQ-15, aligning with the Patient Reported Outcomes Measurement Information System measures used in the DSM-5 field trials. Consequently, the SSS-8 score ranges from 0 to 32. Higher scores indicate a greater severity of SSD. The SSS-8 demonstrated good internal consistency reliability with a Cronbach’s alpha coefficient of 0.81 and displayed significant associations with depression, anxiety, overall health status, and healthcare services utilization.14
Furthermore, the cutoff scores were used to classify individuals into different levels of somatic symptom burden, including minimal, low, medium, high, and very high somatic symptom burden. Scores from 0 to 3 points indicated minimal burden, 4 to 7 points were classified as low burden, 8 to 11 points indicated medium burden, 12 to 15 points identified high burden, and 16 to 32 points defined very high burden.14
This study followed the World Health Organization’s guidelines for translating the instrument.33 The SSS-8 was initially translated from English to Bahasa Indonesia through forward translation by two translators fluent in both languages. The translated versions were then reviewed and compiled by researchers, resulting in the initial version of ISSS-8. Subsequently, two translators, proficient in both English and Bahasa Indonesia, performed a backward translation of the initial ISSS-8 version to English. The forward and backward translations were compared to identify any significant discrepancies. Based on this process, no meaningful differences were found between the forward and backward translations. Additionally, a pre-testing or feasibility phase was conducted with 30 participants. Prior to participation, participants were provided with detailed information about the purpose and procedures of the pre-testing phase and asked to sign an informed consent form. They were then given the translated scale (ISSS-8) to complete, with instructions to carefully read and respond to each item based on their understanding. Following completion of the scale, participants were invited to provide feedback through either individual interviews or structured surveys to gather insights into their experiences with the scale. This feedback aimed to assess item comprehension, cultural sensitivity, and the appropriateness of response options. Participants were asked if they encountered difficulties understanding the language or meaning of the scale items, if they found any items culturally insensitive or inappropriate, and if they had any issues with the response format or options. The overall face validity of the scale was evaluated based on participants’ feedback, assessing whether it appeared to measure what it intended to measure and whether it seemed suitable for the target population. Data analysis was conducted to identify common themes or patterns in participant feedback, guiding potential revisions or adjustments to improve the scale’s clarity, cultural relevance, and suitability for the target population. This iterative process continued until no further issues were identified, and the scale was deemed suitable for use in the main study.
The data were presented using descriptive statistics, including means and standard deviations (SDs). Furthermore, a comprehensive psychometric evaluation was performed, covering construct validity, and reliability testing.
In this study, construct validity underwent assessment through CFA. CFA was conducted using maximum likelihood estimation. Model fit was assessed using specific criteria, including (a) a χ2/df ratio ≤ 3.00 for acceptable fit, (b) root mean square error of approximation (RMSEA) ≤ 0.06 for acceptable fit, (c) standardized root mean square residual (SRMR) ≤ 0.05 for good fit, and (d) goodness of fit index (GFI) and comparative fit index (CFI) ≥ 0.90.
Reliability was assessed through internal consistency measures. Cronbach’s alpha coefficient was employed to evaluate internal consistency for the scale of the ISSS-8. An alpha coefficient exceeding 0.60 was considered indicative of acceptable internal consistency. Homogeneity was gauged by reviewing item-total correlations, with item-total correlations above 0.30 and interitem correlations ranging from 0.30 to 0.70 considered acceptable coefficients, signifying the coherence of the scale’s items.34-36
Results
Table 1 shows characteristics of the 160 participants. The mean age of the participants was 65.51 years. Most participants were female (68.8%), married (66.3%), and had one chronic disease (48,1%). Nearly half of the participants completed high school education or above (45.6%).
As shown in Table 2, one item (item number three) did not meet the acceptability criteria in the CFA, as its factor loading was below the recommended minimum threshold of 0.4 (0.39).17 We did not delete the item despite its factor loading falling below the recommended threshold of 0.4. This decision was based on the theoretical significance of the item and the consideration that the scale consists of only eight items. Each item contributes uniquely to the construct being measured, and removing an item could potentially compromise the comprehensiveness and validity of the instrument.
Therefore, even though one item did not meet the expected factor loading criterion, it was retained in the analysis to maintain the integrity and completeness of the scale. Nevertheless, the remaining seven items demonstrated loading factors surpassing 0.4. It is important to highlight that Item 1 had the highest loading factor at 0.92, while Item 7 had the lowest loading factor at 0.41.
Furthermore, the model fit indices offer additional support for the appropriateness of the proposed model for the ISSS-8. The χ2/df ratio, computed at 0.126, signifies an acceptable fit between the model and the observed data. Additionally, the CFI achieved a score of 0.957, indicating a high degree of agreement between the model and the data. Likewise, the GFI also scored 0.881, confirming the overall fit of the model. The RMSEA, calculated at 0.053, suggests a reasonable approximation of the population covariance matrix, as values below 0.08 are indicative of an acceptable fit. Furthermore, the SRMR registered a value of 0.054, falling within the acceptable range, implying a reasonable level of discrepancy between the model and the observed data. In summary, these results suggest that the proposed model structure exhibits a good fit with the available data, supporting the validity of the ISSS-8 in accurately assessing SSDs in the adult population as indicated in Figure 1.
The reliability of the scale was examined through measures of internal consistency. After conducting the factor analysis, internal consistency was assessed within the same sample by calculating the Cronbach›s alpha coefficient. The obtained Cronbach›s alpha value for the entire scale was 0.627 (Table 3). These coefficients confirm the reliability and consistency of the scale›s items, indicating a high level of consistent responses over time.
Table 1.
Participants characteristics (n = 160)
|
Variable
|
|
| Age, mean (SD ( |
65.51)12.161( |
| Sex, No. (%) |
|
| Male |
50 (31.3) |
| Female |
110 (68.8) |
| Marital status, No. (%) |
|
| Married |
106 (66.3) |
| Unmarried |
5 (3.1) |
| Widow/widower |
49 (30.6) |
| Educational background, No. (%) |
|
| No education |
24 (15.0) |
| Junior high school or below |
63 (39.4) |
| High school or above |
73 (45.6) |
| Number of chronic diseases, No. (%) |
|
| No |
51 (31.9) |
| One |
77 (48.1) |
| Two or more |
32 (20.0) |
Table 2.
The results of the confirmatory factor analysis on the ISSS-8
|
Item
|
I-SSS8
|
Mean (SD)
|
Factor loading
|
| ISSS-1 |
Masalah perut atau buang air besar
(Stomach or bowel problems) |
0.33 (0.75) |
0.92 |
| ISSS-2 |
Nyeri punggung
(Back pain) |
0.72 (1.02) |
0.65 |
| ISSS-3 |
Nyeri di lengan, kaki atau sendi
(Pain in your arms, legs, or joints) |
0.93 (1.08) |
0.39 |
| ISSS-4 |
Sakit kepala ( nyeri kepala )
(Headaches) |
0.73 (1.00) |
0.67 |
| ISSS-5 |
Nyeri dada atau nafas pendek
(Chest pain or shortness of breath) |
0.31 (0.69) |
0.90 |
| ISSS-6 |
Pusing ( sensasi berputar )
(Dizziness) |
0.42 (0.82) |
0.55 |
| ISSS-7 |
Merasa Lelah atau energi lemah
(Feeling tired or having low energy) |
0.23 (0.72) |
0.41 |
| ISSS-8 |
Kesulitan dalam tidur
(Trouble sleeping) |
0.66 (0.99) |
0.56 |
Discussion
The primary objective of this study was to translate the SSS-8 and evaluate its psychometric properties among adults in the Indonesian population. To accomplish this, the SSS-8 was translated into Indonesian, resulting in the ISSS-8, which was then administered to 160 individuals, and its psychometric properties were assessed. In summary, the Indonesian version of the SSS-8 (ISSS-8) exhibited satisfactory validity and reliability. The evaluation of the ISSS-8›s reliability, as assessed by Cronbach›s alpha, indicated acceptable levels in this study. The Cronbach›s alpha coefficient obtained was 0.627, which, while lower than that reported in previous studies, was still considered acceptable when compared to values reported in other language versions such as the German version (0.81 to 0.82),11,14 the Japanese version (0.86),19 the Korean version (0.85),18 and the Greek version (0.831).17
The analysis of construct validity, assessed by conducting CFA. The outcomes of the CFA affirmed a strong fit between the model and the data concerning structural validity. These results align with findings from the German version14 and the Greek version.17 The general-factor structure, as revealed in our analysis, has been consistently demonstrated in previous studies.11,14,18,19 These investigations delved into underlying aspects of somatic symptoms, revealing a comprehensive factor encompassing various somatic symptoms. In a clinical context, these clusters align with four prevalent medical syndromes: pain, gastrointestinal symptoms, cardiopulmonary symptoms, and fatigue. Furthermore, this factor structure allows for the consolidation of individual item scores into a straightforward, easily understandable cumulative score that ranges from 0 to 32 points.
The SSS-8 evaluates the burden of somatic symptoms based on patients› subjective reports without presuming the underlying cause. Its adaptability spans different medical situations, where SSS-8 scores offer measurable assessments of somatic symptom load in individuals dealing with persistent conditions like cancer or coronary heart disease. These conditions commonly lead to varied somatic symptoms, impacting quality of life and psychological well-being. Reference scores for the general population are available, enabling comparisons considering age and gender.11,13,31 Furthermore, the SSS-8 contributes to the diagnosis of SSD, a classification introduced in DSM-5. The scale is particularly relevant to assessing DSM-5 Criterion A for SSD, which requires the presence of one or more distressing somatic symptoms that significantly disrupt daily functioning.1,32
Moreover, repeated use of the SSS-8 offers a means to monitor somatic symptom burden over time. This process facilitates the enhancement of symptom management by enabling regular reassessment and adjustments in treatment.37,38 The SSS-8 has the capability to identify burdensome and untreated somatic symptoms that may not serve as primary indicators of a particular disease, such as musculoskeletal pain in individuals with coronary heart disease.39,40 Considering the correlation between somatic symptom burden and increased healthcare utilization and costs, the administration of the SSS-8 to frequent visitors of outpatient clinics and emergency departments can assist in assessing whether an increased somatic symptom burden contributes to heightened utilization of healthcare service.41,42 Moreover, the scale could find applications in managing patient panels within primary care settings or influencing reimbursement strategies for such patients. The SSS-8 might contribute to risk adjustment for patient populations since somatic symptom burden independently predicts hospitalization and mortality. This prediction holds true even when accounting for factors like clinical characteristics, chronic medical conditions, self-rated health, and depression.43-45
This study has several limitations. The applicability of the results is limited as the study sample may not comprehensively represent all individuals who speak Indonesian. Additionally, the study was conducted with a sample size of 160 individuals, and while this size was sufficient for factor analysis, it is advisable to replicate the study with a larger sample, preferably exceeding 200, to bolster the robustness of the analysis. Lastly, the study exclusively concentrated on individuals without any mental disorder, and it is recommended to broaden the research scope to include individuals with pre-existing disorders, such as anxiety and depression.
This study holds several important implications for clinical practice, research, and cross-cultural understanding. The validated Indonesian version of the SSS-8 emerges as a valuable tool in clinical settings, offering healthcare professionals an efficient means to assess and monitor somatic symptom severity in individuals experiencing depression. Moreover, the study suggests that the ISSS-8 can serve as an effective screening measure for identifying somatic symptoms early on, aiding in the timely diagnosis of SSD. The validation of the ISSS-8 in the Indonesian-speaking population not only contributes to the field of psychometrics but also emphasizes the need for culturally sensitive assessment tools. The study›s findings highlight the efficiency of the Overall, this study advances both clinical understanding and research methodologies, fostering improvements in the assessment and comprehension of somatic symptoms in individuals with depression in the Indonesian-speaking context.
Table 3.
Internal consistency for each factor of ISSS-8
|
Component
|
Cronbach’s alpha if item deleted
|
Item-total correlation
|
Cronbach’s alpha
|
| ISSS-1 |
0.589 |
0.354 |
0.627 |
| ISSS-2 |
0.553 |
0.452 |
| ISSS-3 |
0.628 |
0.232 |
| ISSS-4 |
0.608 |
0.272 |
| ISSS-5 |
0.608 |
0.274 |
| ISSS-6 |
0.613 |
0.251 |
| ISSS-7 |
0.552 |
0.458 |
| ISSS-8 |
0.600 |
0.310 |
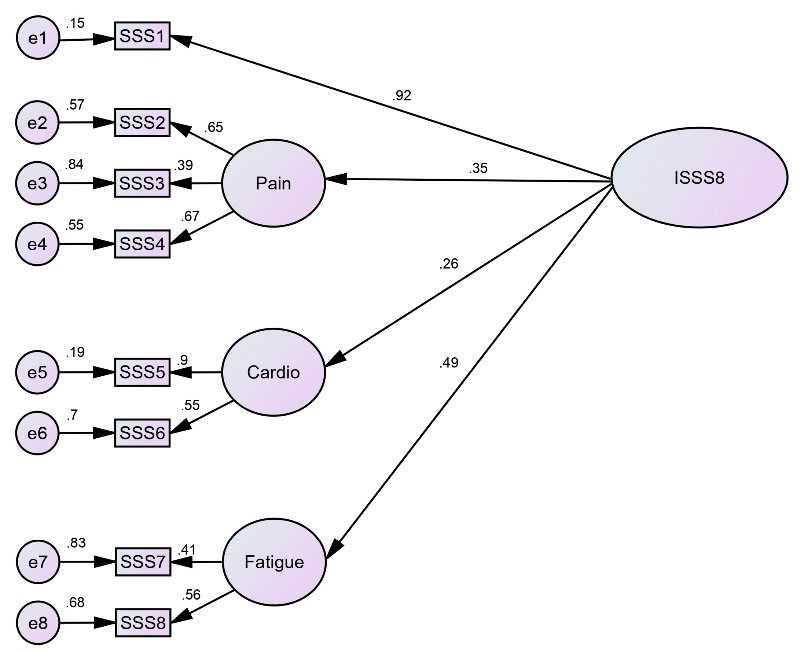
Figure 1.
Confirmatory factor analysis graphical presentation. Abbreviation: SSS = Somatic Symptom Scale
.
Confirmatory factor analysis graphical presentation. Abbreviation: SSS = Somatic Symptom Scale
Conclusion
In conclusion, ISSS-8 showed a valid and reliable tool for assessing somatic symptoms among adults population. The ISSS-8 demonstrated good validity and reliability, aligning with previous research in different cultural contexts. The findings support the utility of SSS-8 as an effective screening measure for somatic symptoms in the Indonesian-speaking population. The study›s outcomes contribute to the broader understanding of the psychometric properties of SSS-8 and emphasize its cross-cultural applicability.
Acknowledgement
The authors would like to thank all of participants of this study. The authors also would like to acknowledge the Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia, for the support of this study.
Competing Interests
The authors affirm that there were no financial or commercial conflicts of interest throughout the conduct of this study and state that they have no competing interests with the funders.
Data Availability Statement
The data associated with this study has not been deposited into any publicly available repository. However, the data can be made available upon a reasonable request.
Ethical Approval
The study received ethical approval from the Research Ethics Committee at The Medical and Health Research Ethics Committee (MHREC) Universitas Gadjah Mada, Indonesia (Approval number: KE/FK/1014/EC/2023). All participants were thoroughly briefed on the study’s purpose, data usage, and storage procedures, and assured that the researcher adhered to all relevant ethical regulations to safeguard the confidentiality of their information. Informed consent was obtained from all participants before completing the instruments. Additionally, data collection involved anonymization measures.
Research Highlights
What is the current knowledge?
-
The Diagnostic and Statistical Manual of Mental Disorders (DSM-5) has reclassified somatoform and related disorders as somatic symptom and related disorders (SSDs).
-
SSDs are prevalent across various medical conditions, impacting quality of life and psychological well-being.
-
The Somatic Symptom Scale-8 (SSS-8) is a scale used to assess somatic symptoms, offering measurable evaluations in clinical and general populations.
-
SSDs often persist for over six months, presenting challenges in severe cases and leading to increased healthcare utilization.
-
The SSS-8 has been employed in different countries, demonstrating favorable item characteristics and reliability in diverse clinical contexts.
What is new here?
-
The study introduces the translation and validation of the SSS-8 for the Indonesian population, resulting in the creation of the Indonesian version (ISSS-8).
-
The ISSS-8 exhibits satisfactory validity and reliability in the Indonesian context, as assessed through Cronbach’s alpha and test-retest results.
-
The study extends the cross-cultural applicability of the ISSS-8 by providing evidence of its psychometric properties in the Indonesian-speaking population.
References
- American Psychiatric Association (APA). Diagnostic and Statistical Manual of Mental Disorders: DSM-5. Washington, DC: APA; 2013.
- American Psychiatric Association (APA). Somatic Symptom and Related Disorders. DSM-5-TR® Clinical Cases. Washington, DC: APA; 2023.
- Dimsdale JE, Creed F, Escobar J, Sharpe M, Wulsin L, Barsky A. Somatic symptom disorder: an important change in DSM. J Psychosom Res 2013; 75(3):223-8. doi: 10.1016/j.jpsychores.2013.06.033 [Crossref] [ Google Scholar]
- Huang WL, Chang SS, Wu SC, Liao SC. Population-based prevalence of somatic symptom disorder and comorbid depression and anxiety in Taiwan. Asian J Psychiatr 2023; 79:103382. doi: 10.1016/j.ajp.2022.103382 [Crossref] [ Google Scholar]
- Wu Y, Tao Z, Qiao Y, Chai Y, Liu Q, Lu Q. Prevalence and characteristics of somatic symptom disorder in the elderly in a community-based population: a large-scale cross-sectional study in China. BMC Psychiatry 2022; 22(1):257. doi: 10.1186/s12888-022-03907-1 [Crossref] [ Google Scholar]
- Alalawi NM, Al Salmani AA, Aljabri MK, Azmi IS, Aljardani MM, Al Mandhari SS. Epidemiology and prevalence of somatic symptom disorder at the primary care level in Muscat, Oman: a cross-sectional study. Int J Psychiatry Med 2023; 58(3):284-94. doi: 10.1177/00912174221088263 [Crossref] [ Google Scholar]
- Goweda R, Alshinawi MA, Janbi BM, Idrees UY, Babukur RM, Alhazmi HA. Somatic symptom disorder among medical students in Umm Al-Qura University, Makkah Al-Mukarramah, Kingdom of Saudi Arabia. Middle East J Fam Med 2022; 20(5):6-11. doi: 10.5742/mewfm.2022.9525030 [Crossref] [ Google Scholar]
- Nazzal Z, Maraqa B, Abu Zant M, Qaddoumi L, Abdallah R. Somatic symptom disorders and utilization of health services among Palestinian primary health care attendees: a cross-sectional study. BMC Health Serv Res 2021; 21(1):615. doi: 10.1186/s12913-021-06671-2 [Crossref] [ Google Scholar]
- Löwe B, Levenson J, Depping M, Hüsing P, Kohlmann S, Lehmann M. Somatic symptom disorder: a scoping review on the empirical evidence of a new diagnosis. Psychol Med 2022; 52(4):632-48. doi: 10.1017/s0033291721004177 [Crossref] [ Google Scholar]
- Witthöft M, Hiller W, Loch N, Jasper F. The latent structure of medically unexplained symptoms and its relation to functional somatic syndromes. Int J Behav Med 2013; 20(2):172-83. doi: 10.1007/s12529-012-9237-2 [Crossref] [ Google Scholar]
- Kohlmann S, Gierk B, Hümmelgen M, Blankenberg S, Löwe B. Somatic symptoms in patients with coronary heart disease: prevalence, risk factors, and quality of life. JAMA Intern Med 2013; 173(15):1469-71. doi: 10.1001/jamainternmed.2013.6835 [Crossref] [ Google Scholar]
- Zijlema WL, Stolk RP, Löwe B, Rief W, White PD, Rosmalen JG. How to assess common somatic symptoms in large-scale studies: a systematic review of questionnaires. J Psychosom Res 2013; 74(6):459-68. doi: 10.1016/j.jpsychores.2013.03.093 [Crossref] [ Google Scholar]
- Kroenke K, Zhong X, Theobald D, Wu J, Tu W, Carpenter JS. Somatic symptoms in patients with cancer experiencing pain or depression: prevalence, disability, and health care use. Arch Intern Med 2010; 170(18):1686-94. doi: 10.1001/archinternmed.2010.337 [Crossref] [ Google Scholar]
- Gierk B, Kohlmann S, Kroenke K, Spangenberg L, Zenger M, Brähler E. The Somatic Symptom Scale-8 (SSS-8): a brief measure of somatic symptom burden. JAMA Intern Med 2014; 174(3):399-407. doi: 10.1001/jamainternmed.2013.12179 [Crossref] [ Google Scholar]
- Toussaint A, Kroenke K, Baye F, Lourens S. Comparing the Patient Health Questionnaire-15 and the Somatic Symptom Scale-8 as measures of somatic symptom burden. J Psychosom Res 2017; 101:44-50. doi: 10.1016/j.jpsychores.2017.08.002 [Crossref] [ Google Scholar]
- Behm AC, Hüsing P, Löwe B, Toussaint A. Persistence rate of DSM-5 somatic symptom disorder: 4-year follow-up in patients from a psychosomatic outpatient clinic. Compr Psychiatry 2021; 110:152265. doi: 10.1016/j.comppsych.2021.152265 [Crossref] [ Google Scholar]
- Petrelis M, Domeyer PR. Translation and validation of the Greek version of the Somatic Symptom Scale-8 (SSS-8) in patients with chronic low back pain. Disabil Rehabil 2022; 44(16):4467-73. doi: 10.1080/09638288.2021.1900415 [Crossref] [ Google Scholar]
- Yang CM, Hwang KS, Lee SY, Seo JS, Jang SH. Reliability and validity of the Korean version of Somatic Symptom Scale-8. Psychiatry Investig 2020; 17(8):814-21. doi: 10.30773/pi.2020.0112 [Crossref] [ Google Scholar]
- Matsudaira K, Oka H, Kawaguchi M, Murakami M, Fukudo S, Hashizume M. Development of a Japanese version of the Somatic Symptom Scale-8: psychometric validity and internal consistency. Gen Hosp Psychiatry 2017; 45:7-11. doi: 10.1016/j.genhosppsych.2016.12.002 [Crossref] [ Google Scholar]
- Kliem S, Krieg Y, Beller J, Brähler E, Baier D. Psychometric properties of the Somatic Symptom Scale-8 (SSS-8) in a representative sample of German adolescents. J Psychosom Res 2021; 149:110593. doi: 10.1016/j.jpsychores.2021.110593 [Crossref] [ Google Scholar]
- Cao J, Wei J, Fritzsche K, Toussaint AC, Li T, Zhang L. Detecting DSM-5 somatic symptom disorder in general hospitals in China: B-criteria instrument has better accuracy-a secondary analysis. Front Psychiatry 2022; 13:935597. doi: 10.3389/fpsyt.2022.935597 [Crossref] [ Google Scholar]
- Yamada S, Hoshi T, Toda M, Tsuge T, Matsudaira K, Oka H. Changes in neck pain and somatic symptoms before and after the adjustment of the pillow height. J Phys Ther Sci 2023; 35(2):106-13. doi: 10.1589/jpts.35.106 [Crossref] [ Google Scholar]
- Huang S, Zhuang W, Wang D, Zha L, Xu X, Li X. Persistent somatic symptom burden and sleep disturbance in patients with COVID-19 during hospitalization and after discharge: a prospective cohort study. Med Sci Monit 2021; 27:e930447. doi: 10.12659/msm.930447 [Crossref] [ Google Scholar]
- Pollo CF, Meneguin S, Miot HA, de Oliveira C. Translation, cultural adaptation and validation of the Somatic Symptom Scale-8 (SSS-8) for the Brazilian Portuguese language. BMC Prim Care 2022; 23(1):222. doi: 10.1186/s12875-022-01836-2 [Crossref] [ Google Scholar]
- Hashimoto K, Takeuchi T, Koyama A, Hiiragi M, Suka S, Hashizume M. Effect of relaxation therapy on benzodiazepine use in patients with medically unexplained symptoms. Biopsychosoc Med 2020; 14:13. doi: 10.1186/s13030-020-00187-7 [Crossref] [ Google Scholar]
- Sattel H, Lahmann C, Gündel H, Guthrie E, Kruse J, Noll-Hussong M. Brief psychodynamic interpersonal psychotherapy for patients with multisomatoform disorder: randomised controlled trial. Br J Psychiatry 2012; 200(1):60-7. doi: 10.1192/bjp.bp.111.093526 [Crossref] [ Google Scholar]
- Hahn SR. Physical symptoms and physician-experienced difficulty in the physician-patient relationship. Ann Intern Med 2001; 134(9 Pt 2):897-904. doi: 10.7326/0003-4819-134-9_part_2-200105011-00014 [Crossref] [ Google Scholar]
- Sardesai A, Muneshwar KN, Bhardwaj M, Goel DB. the importance of early diagnosis of somatic symptom disorder: a case report. Cureus 2023; 15(9):e44554. doi: 10.7759/cureus.44554 [Crossref] [ Google Scholar]
- Dunphy L, Penna M, El-Kafsi J. Somatic symptom disorder: a diagnostic dilemma. BMJ Case Rep 2019; 12(11):e231550. doi: 10.1136/bcr-2019-231550 [Crossref] [ Google Scholar]
- Kyriazos TA. Applied psychometrics: sample size and sample power considerations in factor analysis (EFA, CFA) and SEM in general. Psychology 2018; 9(8):2207-30. doi: 10.4236/psych.2018.98126 [Crossref] [ Google Scholar]
- Kroenke K, Spitzer RL, Williams JB. The PHQ-15: validity of a new measure for evaluating the severity of somatic symptoms. Psychosom Med 2002; 64(2):258-66. doi: 10.1097/00006842-200203000-00008 [Crossref] [ Google Scholar]
- Narrow WE, Clarke DE, Kuramoto SJ, Kraemer HC, Kupfer DJ, Greiner L. DSM-5 field trials in the United States and Canada, part III: development and reliability testing of a cross-cutting symptom assessment for DSM-5. Am J Psychiatry 2013; 170(1):71-82. doi: 10.1176/appi.ajp.2012.12071000 [Crossref] [ Google Scholar]
- World Health Organization (WHO). WHODAS 2.0 Translation Package (Version 1.0): Translation and Linguistic Evaluation Protocol and Supporting Material. WHO; 2012. Available from: https://terrance.who.int/mediacentre/data/WHODAS/Guidelines/WHODAS%202.0%20Translation%20guidelines.pdf. Accessed April 1, 2022.
- Gliem JA, Gliem RR. Calculating, Interpreting, And Reporting Cronbach’s Alpha Reliability Coefficient for Likert-Type Scales. Midwest Research-to-Practice Conference in Adult, Continuing, and Community Education; 2003.
- Cornélio ME, Gallani MC, Godin G, Rodrigues RC, Mendes RD, Nadruz Junior W. Development and reliability of an instrument to measure psychosocial determinants of salt consumption among hypertensive patients. Rev Lat Am Enfermagem 2009; 17(5):701-7. doi: 10.1590/s0104-11692009000500017 [Crossref] [ Google Scholar]
- Ferketich S. Ferketich SFocus on psychometricsAspects of item analysis. Res Nurs Health 1991; 14(2):165-8. doi: 10.1002/nur.4770140211 [Crossref] [ Google Scholar]
- Guadagnoli E, Velicer WF. Relation of sample size to the stability of component patterns. Psychol Bull 1988; 103(2):265-75. doi: 10.1037/0033-2909.103.2.265 [Crossref] [ Google Scholar]
- Kroenke K, Spitzer RL, Williams JB, Löwe B. The Patient Health Questionnaire Somatic, Anxiety, and Depressive Symptom Scales: a systematic review. Gen Hosp Psychiatry 2010; 32(4):345-59. doi: 10.1016/j.genhosppsych.2010.03.006 [Crossref] [ Google Scholar]
- Löwe B, Spitzer RL, Williams JB, Mussell M, Schellberg D, Kroenke K. Depression, anxiety and somatization in primary care: syndrome overlap and functional impairment. Gen Hosp Psychiatry 2008; 30(3):191-9. doi: 10.1016/j.genhosppsych.2008.01.001 [Crossref] [ Google Scholar]
- Sha MC, Callahan CM, Counsell SR, Westmoreland GR, Stump TE, Kroenke K. Physical symptoms as a predictor of health care use and mortality among older adults. Am J Med 2005; 118(3):301-6. doi: 10.1016/j.amjmed.2004.12.015 [Crossref] [ Google Scholar]
- Zhang Y, Baumeister D, Spanidis M, Engel F, Berens S, Gauss A. How symptoms of simple acute infections affect the SSS-8 and SSD-12 as screening instruments for somatic symptom disorder in the primary care setting. Front Psychiatry 2023; 14:1114782. doi: 10.3389/fpsyt.2023.1114782 [Crossref] [ Google Scholar]
- Fujii T, Oka H, Katsuhira J, Tonosu J, Kasahara S, Tanaka S. Association between somatic symptom burden and health-related quality of life in people with chronic low back pain. PLoS One 2018; 13(2):e0193208. doi: 10.1371/journal.pone.0193208 [Crossref] [ Google Scholar]
- Li Z, Zhang Y, Pang Y, He Y, Song L, Wang Y. The mediating effect of somatic symptom disorder between psychological factors and quality of life among Chinese breast cancer patients. Front Psychiatry 2023; 14:1076036. doi: 10.3389/fpsyt.2023.1076036 [Crossref] [ Google Scholar]
- Atasoy S, Hausteiner-Wiehle C, Sattel H, Johar H, Roenneberg C, Peters A. Gender specific somatic symptom burden and mortality risk in the general population. Sci Rep 2022; 12(1):15049. doi: 10.1038/s41598-022-18814-4 [Crossref] [ Google Scholar]
- Engelmann P, Löwe B, Brehm TT, Weigel A, Ullrich F, Addo MM. Risk factors for worsening of somatic symptom burden in a prospective cohort during the COVID-19 pandemic. Front Psychol 2022; 13:1022203. doi: 10.3389/fpsyg.2022.1022203 [Crossref] [ Google Scholar]