Journal of caring sciences. 14(3):182-190.
doi: 10.34172/jcs.025.33367
Original Article
The Program Development of Training for Family Caregivers Caring for Homebound Older Adults in a Rural Community in Thailand: A Mixed-Methods Study
Boonyada Wongpimoln Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Project administration, Validation, Visualization, Writing – original draft, Writing – review & editing, 1 
Ladda Pholputta Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – review & editing, 1, *
Nitchapanrawee Phengphol Conceptualization, Funding acquisition, Project administration, Supervision, Validation, Visualization, Writing – review & editing, 1
Sattawas Udonsat Formal analysis, Funding acquisition, Project administration, Project administration, Validation, Visualization, Writing – review & editing, 1
Author information:
1Division of Adult and Gerontological Nursing, Faculty of Nursing, Roi Et Rajabhat University, Roi Et, Thailand
Abstract
Introduction:
Family caregivers play a key role in supporting homebound older adults. This study explored the community context, developed, and evaluated a training program for family caregivers of homebound older adults in Selaphum District, Roi Et province, Thailand.
Methods:
We used a mixed method approach with three phases. In phase I, we conducted semi-structured interviews with eight family caregivers. In phase II, we developed a training program based on the interview findings. In phase III, we implemented and evaluated the program using a pretest-posttest nonequivalent control group design with 57 participants in each group. We collected data through in-depth interviews, and questionnaires on knowledge, attitude, and practice. We analyzed quantitative data using descriptive and inferential statistics, and qualitative data using content analysis.
Results:
Two themes were explored in Phase I: Low quality of care, and Caregivers burden. A program involves six activities: 1) providing family caregivers’ knowledge, 2) demonstrating and practicing caregiving, 3) providing homebound older adults’ hygiene care 4) promoting leisure and recreation activities to homebound older adults 5) modifying the safe environment and 6) creating a sense of self-worth and self-efficacy among the family caregivers. The quantitative results showed that the experimental group had significantly higher mean score in knowledge, attitude, and practice compared to the control group.
Conclusion:
This study enhanced knowledge, attitude, and practice among family caregivers for caring homebound older adults, resulting in better caregiving outcomes and improved quality of life for both caregivers and care recipients.
Keywords: Program development, Elderly, Caregivers, Homebound persons
Copyright and License Information
© 2025 The Author(s).
This work is published by Journal of Caring Sciences as an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/). Non-commercial uses of the work are permitted, provided the original work is properly cited.
Funding Statement
This study was funded and supported by the Faculty of Nursing, Roi Et Rajabhat University, Roi Et, Thailand (Grant No. Special/2566).
Introduction
Globally, advancements in health care services and living standards have resulted in increased life expectancy and a higher proportion of older people in populations. The number of people aged 65 years or older worldwide is projected to more than double, rising from 761 million in 2021 to 1.6 billion in 2050. The number of people aged 80 years or older is growing even faster.1In Thailand, the number of people aged 60 and older is expected to grow from 13% in 2020 to 25% in 2060, making Thailand one of the fastest-aging countries in the world.2 This increase in older population can also lead to an increase in the proportion of homebound older adults who stay at home.3 In Roi Et province, there are 899,141 residents, with 226,294 older adults, accounting for 25.17%.4
The older adults can be categorized based on their functional and physical capacity using the Barthel Index of Activities of Daily Living (ADLs). These groups are as follows: active (ADLs more than 11), homebound (ADLs, 5-11), and bedridden elderly (ADLs, 0-4). Each group has particular care needs. For example, a healthier older adult may not require any assistance to perform daily activities, while the bedridden and homebound may need more support in their daily routines.5 The rising number of dependent older adults with limited functional ability and complex health conditions is contributing to an increased healthcare burden worldwide.1,6
Being homebound can affect physical and mental health by decreasing movement, which can be exacerbated by the deterioration of the older adult’s health.7Homebound older adults experience decreased physical activity, psychological health, and quality of life.8Limited social connectedness in older adults is a risk factor for poor physical and mental health. Older adults who are socially isolated, lonely, and disconnected have a higher risk of chronic illness, depression, and premature death.9As society ages, an increase in the number of older adults who need long-term care, including homebound older adults, has emerged as a major social problem. Living in “the boundary of daily life limited to home” negatively affects older adults’ health and decreases their quality of life.7Despite the high demand for medical care services, their access to healthcare services is limited because of their physical and economic dependency, coupled with a lack of information and support.10 Thus,caregiving for persons with multiple chronic conditions, including those who are homebound, can be challenging for family caregivers.11
Family caregivers are defined as unpaid individuals involved in assisting family members with activities of daily living and/or medical tasks. They are the primary source of support for older adults with chronic illness and disability12 and play a key role in delaying and possibly preventing institutionalization, establishing a comfortable routine, benefiting long-term health, reducing the risk of depression, and helping older adults maintain exercise and healthy eating habits. However, their knowledge, practice, and needs in the care of older adults are often overlooked.13Previous study has shown that family caregivers had inadequate knowledge and skills to deliver proper care and received little guidance from healthcare professionals, resulting in devastating effects for both the older adults and family caregivers.14
In rural northeastern Thai society, most family caregivers provide care to their homebound older adults who are their loved ones. Previous study in the United State stated that over 70 percent of family caregivers report receiving little to no training on how to provide care, particularly in managing medical and personal care tasks.15 To reduce the unmet needs of family caregivers, it is important to understand the current situation as well as interventions for homebound older adults. The development of a program providing knowledge, strengthening attitude, and practicing care for homebound older adults by family caregivers results in homebound older adults having a better quality of life. Previous studies in Cameroon developed a training program for older adults which includes assistance with activities of daily living and instrumental activities of daily living, psychosocial care strategies to involve elderly persons in various activities, and the creation of age-friendly environments.16Furthermore, the researchers, nursing lecturers at The Faculty of Nursing at Roi Et Rajabhat University, are responsible for developing local communities by integrating knowledge into innovation in local development to create national stability as a vision of the university, which is necessary to enhance the quality of life of the people, including family caregivers and homebound older adults. Consequently, the researchers were interested in conducting this study. This study hypothesized that family caregivers would have enhanced knowledge, positive attitude, and enhanced practice after participating in the program development. This study aimed to explore the community context, develop, and evaluate the training program for family caregivers of homebound older adults in Selaphum District, Roi Et province, Thailand, to educate and empower them to take responsibility for managing, promoting, and providing care to homebound older adults effectively.
Materials and Methods
The methodology employed in this study was Research and Development (R&D), utilizing the exploratory sequential mixed method design conducted from June to October 2023 to examine three objectives as described in the following three phases.
Phase I: Explored Community Context
Based on the literature review, in-depth interviews were used to explore the community context among family caregivers in Selaphum District, Roi Et province, Thailand. The interviews were performed by researchers experienced in conducting qualitative research and who had no intimate relationship or influence on the welfare of the participants. Participants were recruited using purposive sampling and were eligible to participate based on criteria. They were being Thai, older than 18 thus able to give informed consent, being a family members of a homebound older adults (aged ≥ 60 years and a self-care ability with a score between 5-11 score assessed by Barthel Activity of Daily living), taking care of older adults as the main caregiver for more than 3 months, and able to communicate in Thai language. The snowballing approach was used to supplement purposive sampling. Sampling continued until data saturation was reached or when there was no new information17 to complete the categories and subcategories and answered the study question. Participants were appointed for individual face-to-face in-depth interviews through semi-structured questions that lasted approximately 45 to 60 minutes. An interview guide was developed by all researchers based on the study objectives and relevant research literature and validated by three experts in qualitative research. The questions included open-ended questions such as: 1) How do you feel about caring for homebound older adults? 2) How do you provide care? 3) What are the problems/obstacles? 4) How do you manage? Family caregivers shared their experiences on care needs for their relatives. Researchers extracted information until data saturation was reached from the eight participants. Interviews were digitally recorded and subsequently transcribed verbatim. After each interview, researchers immediately began to write basic field notes to capture participants’ behavior and facial expressions and the environment in the field to complete the information. The information and data from Phase I will be used to develop the program in Phase II. Data collection took place at Selaphum District, Roi Et province. Demographic data of participants were obtained using a demographic form during individual interviews at their own homes.
Phase II: Developed a Training Program
Researchers designed a draft of a training program based on the information and data from Phase I. The content of the training program comprised three sessions and divided into sixth activities. The first session, theoretical training, involved a 5- day training session (30 hours). Family caregivers were trained by a nutritionist, physical therapist, community nurse practitioner, and gerontologist nurse to increase their knowledge in caring for homebound older adults. Topics included nutrition, exercise, mental care, sleep and rest, urinary and bowel elimination, environment and fall prevention, personal hygiene, and basic life support. The second session, laboratory training, involved a 5-day training session (30 hours) where family caregivers practiced basic care for older adults, including primary health screening such as blood pressure and body temperature monitoring, exercise, basic life support, hygiene care such as oral and perineum care, meditation and recreation activities, food preparation, and environment in fall prevention. The first and second session were conducted at Roi Et Rajabhat University. The third session, practical training, involved twelve weeks of practical training at Koh-keaw and Ta-muang Subdistrict, Roi Et province, Thailand, consisting of four activities: Firstly, providing hygiene care to homebound older adults: Family caregivers practiced to provide proper basic care to homebound older adults, including bathing, shampooing, nail clipping, oral care, and perineum care. Secondly, promoting leisure and recreation activities to homebound older adults: Family caregivers found available time for promoting leisure and recreation activities that appropriated with their loves one such as gardening, knitting, card club, jigsaw, puzzles, yoga, and dancing. This can promote cognitive stimulation, enhances emotional well-being, improves physical health, and fosters social connection. So, the researchers would be a consultant for family caregivers. This activity could be promoted both mental and physical among homebound older adults. Thirdly, modifying the safety environment: Family caregivers provide home modification such as cleaned up clutter, repaired or removed tripping hazard, lighted it right, applied reflective tape to a stair, and the use of walking aids. Lastly, creating a sense of self-worth and self-efficacy to the family caregivers: Family caregivers reflexed and shared their own strengths and areas that needed development among family caregivers weekly until 12 weeks. This leaded to higher quality of care for homebound older adults. The process of training program was divided into 3 steps; 1) pre-assessment, 2) Implementation, and 3) Evaluation. The Program content was validated by five experts in the fields of gerontology, education, and community health nursing. Evaluation result of appropriateness of the activities for healthcare among homebound older adults, the overall average score was at a high level (Mean= 4.40, SD = 0.66). This was revised according to the recommendations of those experts and prepared in Figure 1 before full implementation in step 3.
Phase III: Evaluation a Program Development
The duration of training program was implemented over a period of 12 weeks at the Koh-keaw and Ta-muang Subdistrict,Selaphum District, Roi Et Province, Thailand. Program development was conducted by 114 family caregivers and randomly assigned to the experimental (n = 57) and control groups (n = 57) to homebound older adults through a pretest-posttest nonequivalent control group with a quasi-experimental quantitative design. The control group received usual family caregivers’ care. The experimental group received the developed program. The researchers provided consultations to family caregivers at the study site as needed. As the result, 114 family caregivers participated in the evaluation. The research was able to include comparison of knowledge, attitude, and practice among family caregivers before and after implementation of the program as shown in Figure 2.
The sample group was family caregivers of homebound older adults. Inclusion criteria were: being Thai; older than 18 thus able to give informed consent; being a family members of a homebound older adults (aged ≥ 60 years and a self-care ability with a score between 5-11 score assessed by Barthel Activity of Daily living); taking care of older adults as the main caregiver for more than 3 months; and able to communicate in Thai language. Purposive random sampling was use to select two rural communities (Koh-keaw and Ta-muang Subdistrict) which is similar setting from 18 Sub-District of Selephum District, Roi Et province, Northeastern, Thailand. After that, simple random sampling was used from caregiver lists from Koh-keaw and Tha-muang health promoting hospital. The sample size was calculated by using the G*Power 3 program.18The effect size was determined at 0.5.19 The power of test was 0.80, the significance level was 0.05., showing a sample size of 51 participants per group, or 102 participants total. Anticipating dropout rate of 10%,20 57 participants per group or a total number of 114 participants were recruited. The participants from two rural communities in Selaphum District, Roi Et province, northeast Thailand, were equally assigned to the control and intervention groups.
The tool for quantitative data collection were three instruments. Firstly, the knowledge questionnaire. It is a 25 items in which respondents were asked to rate each item as correct or incorrect on knowledge of family caregivers about caring homebound older adults. The questionnaire had both positive and negative item questions, with negative item score reversed. The questionnaire presents seven dimensions includes nutrition, exercise, mental care, sleep and rest, urinary and bowel elimination, environment in fall prevention and, personal hygiene. The score of all item was classified into three level as follow: low (0-8 score), fair (9-16 score), high (17-25). Secondly, attitude questionnaire. A 5-item structured questionnaire was used to assessed the level of attitude, each rated on 4-point Likert scale, with strongly agree (4 scores), agree (3 scores), neither agree nor disagree (2 scores), and disagree (1 score). The questionnaire had both positive and negative item questions, with negative item score reversed. The interpretation of mean score was categorized into three level: poor (1.00-1.99), fair (2.00-2.99), and good (3.00-4.00). Lastly, practice questionnaire. A 16-item structured questionnaire with a 4-point Likert scale was used to measure respondents’ level of practice, with respondents being asked to identify weather they practiced always (7 day/week) (3 score), almost (4-6 day/week) (2 scores), sometimes (1-3 day/week) (1 score), or never (0 score). The questionnaire presents seven dimensions includes nutrition, exercise, mental care, sleep and rest, urinary and bowel elimination, environment in fall prevention and, personal hygiene. The interpretation of mean score was divided into 3 levels; 0.00-0.99 as poor level, 1.00-1.99 as average level, 2.00- 3.00 as good level. All instruments were developed by the researchers. Data was analyzed using percentages and means for demographic data. Questionnaires were analyzed using mean, standard deviation, independent t-test, and paired t-tests.
The instruments were tested for content validity by three experts (two gerontology nurses and one community nurse). The implementation knowledge, attitude, and practice questionnaire had a scale-level content validity index (S-CVI) of 0.90, 0.91, 0.94 respectively and consistency reliability tested through a pilot study among 30 family caregivers who had similar qualifications to the actual participants. In this study, The Kuder-Richardson 20 (KR-20) of the knowledge questionnaire was 0.80, while the Cronbach’s alpha values for the attitude and practice questionnaire were 0.86 and 0.89 respectively.
The tool for qualitative data collection was in-depth interview through semi-structured questions to explore community context and need of healthcare among family caregivers in caring homebound older adults. Data were analyzed by using content analysis method.21 Transcripts from participants were read line-by-line. Then, codes were generated. Similar codes were grouped into sub-themes and themes, respectively. This analysis was done manually.
Lincoln and Guba’s trustworthiness criteria were applied.22 Credibility was established by building relationship with all participants in order to build trust so that the accuracy of the data could be achieved. The researchers conducted member checking by discussing the interpretation reports with three participants in this study. Transferability was produced by providing a thick description of information relevant to the context and participants. Dependability was achieved when the researchers reviewed the interviews and analyzed the data independently. After that, the researchers discussed reaching a consensus. Finally, confirmability was obtained by establishing an audit trail using field notes, checking and rechecking the raw data with the experts as external auditors, and analyzing and synthesizing data throughout the study.
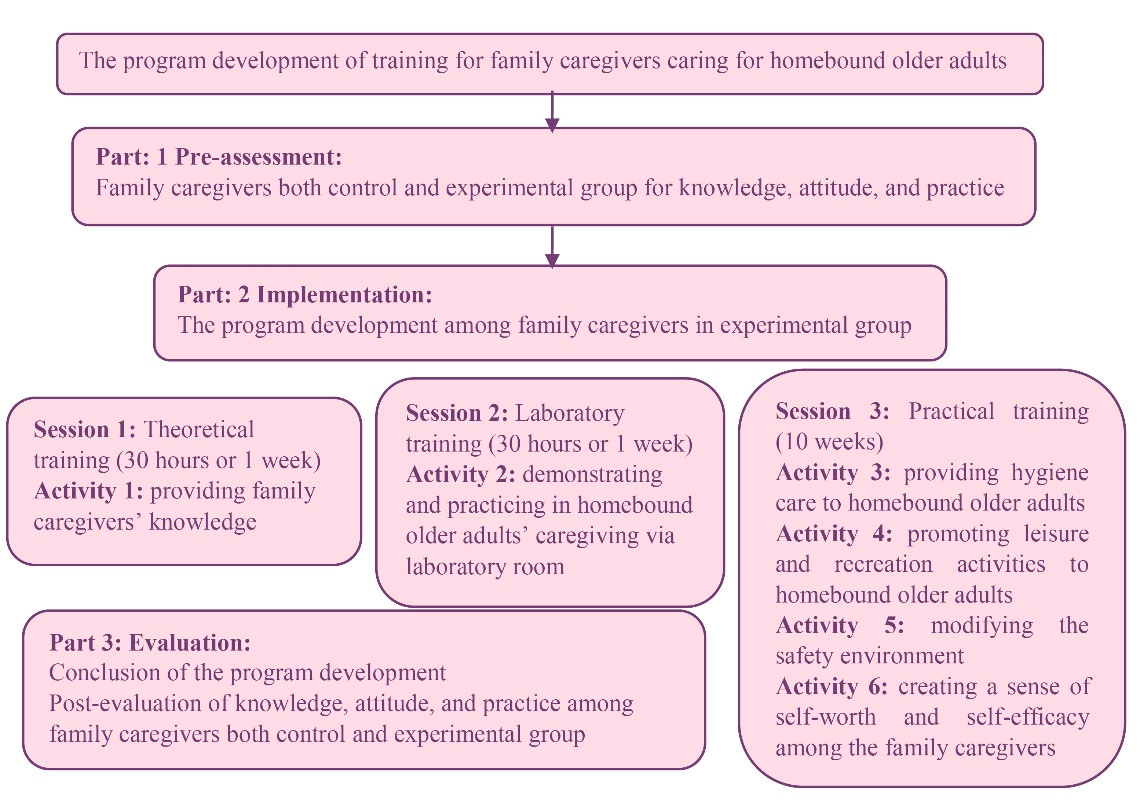
Figure 1.
Program development of family caregivers training for caring homebound older adults
.
Program development of family caregivers training for caring homebound older adults
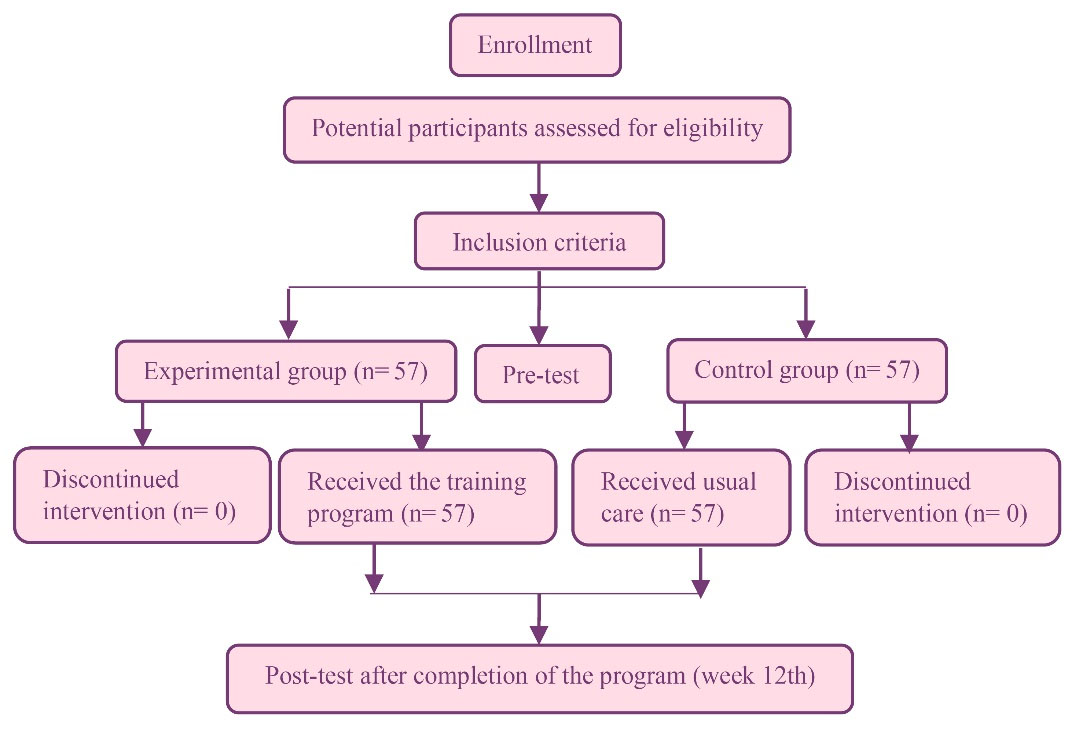
Figure 2.
Flow of participants throughout the study
.
Flow of participants throughout the study
Results
Findings from this research can be summed up into qualitative and quantitative results as follows:
1. Findings on Qualitative Results on Current Situation and Need for Healthcare Among Homebound Older Adults in a Community
Seven participating family caregivers were females and one were male with ages ranging from 32 to 68 years. Five of the participants had a primary school education, and three were high school graduates and above. Caregiving experience of homebound older adults were between three months to until 5 years. Most of family caregivers were married and adult children of homebound older adults. Findings were defined into two major themes and two sub-themes as shown in Table 1.
Theme 1: Low Quality of care
Many family caregivers expressed that caregiving for their loved ones was not easy. All of them provided caregiving with willingness. But, they sometimes felt unconfident in caring resulting in providing care infectively. Some family caregiver felt incapable of caregiving because they did not know how to provide care. However, during the care provided, the main issues of the caregivers were as follows: 1) knowledge deficit, and 2) poor practice.
Table 1.
Themes, sub-themes, and basic concept codes extracted
|
Themes
|
Sub-themes
|
Basic concept codes
|
| Low quality of care |
Knowledge deficit
Poor practice |
-Misunderstanding about caring older adults with underlying diseases
-Don’t know about caring older adults with pressure sore
-Providing improper care |
| Caregiver burden |
|
-Cannot go anywhere in social outings.
-Feeling stressful that being the only one who provided care
-Struggling to find time for self-care. |
Sub-theme 1: Knowledge deficit
Even through the family caregivers might have already provided care completely, they still needed to learn proper care for the homebound older adults. Some family caregivers expressed that they were unable to promote both mental and physical health for homebound older adults.
“…Since my mom have many underlying diseases such as diabetes mellitus, dyslipidemia, hypertension, heart disease, and chronic kidney disease stage 3, I do not let her to do all types of exercise because I am worry about the accident and she will be more sickness. So, I almost do everything for her as much as possible such as meal preparation, house cleaning, cloths washing, bathing, toileting, and managing medication to maintain her health…” (Participant 1)
“…I do not know what to do when my mom has pressure sore. I take her to the hospital.” (Participant 5)
Sub-themes 2: Poor Practice
Many family caregivers have provided care improper, they still need to learn specific health care for the homebound older adults. Some family caregivers were unable to provide basic care.
“…I used alcohol to clean a perineal care for my dad who lived with a urinary catheter...” (Participant 3)
“…My aunt did not want to eat, so I prepared her favorite food which was raw beef salad for her….” (Participant 8)
“…When my mother smells bad, I used fabric softener to wash my mother.” (Participant 6)
Theme 2: Caregiver Burden
Due to the health problems of homebound older adults, some family caregivers felt burdened because of inability to maintain social activities. Care responsibilities might force them to give up some of the social activities they previously enjoyed, which made them feel isolated from typical social events such as meeting friends, making merit, and traveling. Sometimes, caregivers needed to find ways to take care themselves.
“…I cannot go anywhere in social outings. My children and friends invited me to make merit at famous temple but I cannot…” (Participant 7)
“…Sometimes, I felt stressful that I had to be the only one who provided care to my mom because I could not go for travelling anywhere...” (Participant 5)
“…I struggle to find time for self-care while being a full-time caregiver…” (Participant 4)
2. Findings on Quantitative Results on the Implementation of Program Development of Family Caregivers Training for Caring Homebound Older Adults
Finding on the Demographic Data Among Family Caregivers
The majority of participants in the experimental and the control group were female, in the middle adulthood (41-59 years old). The average period of being caregiver of both group was similar for 1-5 years (70.20% for the experimental and 75.40% for the control group). Most of participant in experimental group and control group were farmer, married, and all were Buddhist. Participants had graduated in secondary school level, 49.10% in the experimental group and 42.10% in the control group. Most in both group had status as child at 59.60% and 56.10%, respectively. Also, the majority of them earned a monthly income of 5,000-10,000 baht (149-298 USD), 66.70% in the experimental group and 68.40% in the control group. There were no significant differences between participants in the experimental and control groups regarding demographic (P > 0.05).
Finding on the Implementation of Program Development among Family Caregivers
The comparison of the average score of variables at before and after the implementation of program development (n = 114). Within-group comparisons showed that the experimental group experienced significant improvements from before to after implementation in knowledge (P < 0.001), attitude (P < 0.001), and practice (P < 0.001), whereas the control group showed no significant changes in knowledge (P = 0.214) and attitude (P = 0.322), but a small yet significant increase in practice (P = 0.009) as shown in Table 2. The comparison of the average score of variables between experimental (n = 57) and control group (n = 57) at before and after the implementation of program development, between-group comparisons showed no significant differences in knowledge, attitude, and practice scores between the experimental and control groups before the implementation (P = 0.682, 0.743, and 0.857, respectively). After implementation, the experimental group demonstrated significantly higher scores than the control group for knowledge (P < 0.001), attitude (P < 0.001), and practice (P < 0.001) as shown in Table 3.
Table 2.
The comparison of the average score of variables at before and after the implementation of program development. (N = 114)
|
Variables
|
Mean (SD)
|
t
|
P
value
|
|
Before implementation
|
After implementation
|
| Knowledge |
|
|
|
|
| Experimental group |
18.14 (1.505) |
20.86 (2.333) |
12.015 |
< 0.001 |
| Control group |
18.02 (1.685) |
18.19 (1.663) |
1.256 |
0.214 |
| Attitude |
|
|
|
|
| Experimental group |
16.28 (0.796) |
18.82 (1.212) |
17.411 |
< 0.001 |
| Control group |
16.23 (0.907) |
16.25 (0.912) |
1.000 |
0.322 |
| Practice |
|
|
|
|
| Experimental group |
52.04 (4.179) |
57.05 (5.177) |
9.088 |
< 0.001 |
| Control group |
51.89 (4.122) |
52.23 (3.813) |
2.700 |
0.009 |
Table 3.
The comparison of the average score of variables between experimental (N = 57) and control group (N = 57) at before and after the implementation of program development
|
Variables
|
Mean (SD)
|
t
|
P
value
|
|
Experimental group
|
Control group
|
| Knowledge |
|
|
|
|
| Before implementation |
18.14 (1.505) |
18.02 (1.685) |
0.410 |
0.682 |
| After implementation |
20.86 (2.333) |
18.19 (1.663) |
7.026 |
< 0.001 |
| Attitude |
|
|
|
|
| Before implementation |
16.28 (0.796) |
16.23 (0.907) |
0.329 |
0.743 |
| After implementation |
18.82 (1.212) |
16.25 (0.912) |
12.838 |
< 0.001 |
| Practice |
|
|
|
|
| Before implementation |
52.04 (4.179) |
51.89 (4.122) |
0.181 |
0.857 |
| After implementation |
57.05 (5.177) |
52.23 (3.813) |
5.665 |
< 0.001 |
Discussion
Most participants in this study were middle adulthood. The role of a child in a Thai family focuses on expressing their gratitude by providing unconditional care with love for their seniors to repay their kindness. However, the result of this study showed that family caregivers lacked of knowledge and poor practice to provide care for homebound older adults. This was happened because homebound older adults were mostly had chronic diseases and functional impairment23 which needed a specific care. Similarly, most of family caregivers often felt unprepared to provide care, lacked specific knowledge and caregiving skills to deliver proper care.13,14,24,25 Previous study found that more than half of family caregivers were poor in total knowledge about elderly care and they were not competent in practice.26 Lack of knowledge and practice resulted in devastating consequences to both the older adults and family caregivers in Sri Lanka.14Nevertheless, there was needed for training on care for homebound older adults at home in Cameroon.24 Therefore, the researchers developed a training program of family caregivers for caring homebound older adults.
Previous literature findings stated that homebound older adults needed help from family caregivers due to physical limitations from chronic conditions. Family caregivers often assumed daily caregiving tasks to assist their loved ones, and provide much needed emotional support.27Importantly,homebound older adults experienced both physical and mental health challenges that restricted their ability to participate in activities of daily living, recreation, and social interactions, as a result, they often felt dependent, helpless, lonely, and socially isolated.23 However, participating in leisure activities contributed successful aging by supporting an active lifestyle28 and providing environmental modification was essential for preventing falls among homebound older adults as well.29,30So, family caregivers play a significant role for caring homebound older adults. In addition, previous studied found that family caregiver had a low-moderate level of burden and moderate quality of life in caring older adults with physical disabilities in a rural community.31 Consequently, there was important to develop a training program of family caregivers to prevent worsen health condition among homebound older adults and enhance self-worth and self-efficacy among family caregivers. A training program in this study involved providing knowledge, demonstrating and practicing in caring homebound older adults, providing hygiene care, providing leisure and recreation activities, modifying the safety environment to homebound older adults and, creating a sense of self-worth and self-efficacy among the family caregivers to improve their caring abilities. This study developed a training program based on literature review and qualitative results. In contrast, previous studies developed training programs using the Health Belief Model and found that the programs could improve health and well-being among the elderly.16 Similarly, the findings highlight the widespread of family caregivers’ training needs, particularly with medically oriented activities, and indicated that escalations in older adults’ care needs are linked to caregiver training needs. Therefore, caring may present critical opportunities to connect family caregivers with training resources.32 Furthermore, healthcare providers including nurses should be involved in healthcare and health promotion among homebound older adults to support family caregivers.33
This study results also showed that the training program carried out by family caregivers which resulted in higher mean score of knowledge, attitude, and practice. Therefore, family caregivers who had inadequate knowledge, attitude, and caring ability could be improved quality of care. Importantly, homebound older adults were very often representing the preliminary stage for bedridden older adults. Hence, training program for family caregivers to maintain the quality of life is equally important as preventing them from becoming bedridden34,35 However, to prevent rural older adults from becoming homebound, it is necessary that they are supported by the health and welfare system.
Conclusion
Family caregivers provided healthcare for homebound older adults who was their loves ones, but they still lacked of knowledge and had poor practice on providing a healthcare for homebound older adults.This training program development could enhance knowledge, attitude, and practice among family caregivers for caregiving homebound older adult. Thus, this model could be applied to other communities with similar contexts. However, as the Thailand demographic continues to shift toward more adults living into older age, health care systems must provide this vulnerable population with the appropriate care and resources, as well as improve support for the family caregivers of homebound older adults.
Firstly,the findings of this study cannot be freely generalized to the population in other regions of Thailand or other countries because it was set in Selaphum District, Roi Et province, the northeastern region of Thailand. Thus, cultural differences would lead to an increased likelihood of differences in the results. Secondly, this research should involve community participation in every phase to create strength and sustainability.
Acknowledgements
We would liketo express special thanks to the Faculty of Nursing, Roi Et Rajabhat University, Roi Et, Thailand, for providing a scholarship to this study. Lastly, we are also truly grateful to family caregivers and their homebound older adults for their cooperation.
Competing Interests
There was no conflict of interest in this study.
Data Availability Statement
Data is not and will not be made available elsewhere. Further data set could be obtained on request if required through corresponding author with email: ladda@reru.ac.th.
Ethical Approval
Permission was obtained from the Research Ethics Committee of Roi Et Rajabhat University, Thailand (certification number 073/2566). All participants received written and verbal explanations of the study. Before giving written informed consent they learnt of the objectives, methods, risks, benefits, and their right to withdraw from the study at any time.
Research Highlights
What is the current knowledge?
What is new here?
-
Family caregivers lack sufficient knowledge and skills to care for homebound older adults.
-
Family caregivers experience a high caregiving burden.
-
This training program development could enhance knowledge, attitude, and practice among family caregivers for caregiving homebound older adult.
References
- United Nations, Department of Economic and Social Affairs. World Social Report 2023: Leaving No One Behind in an Ageing World. Available from: https://desapublications.un.org/publications/world-social-report-2023-leaving-no-one-behind-ageing-world. Accessed January 19, 2024.
- World Health Organization (WHO). Thailand’s Leadership and Innovations Towards Healthy Ageing. WHO; 2023. Available from: https://www.who.int/southeastasia/news/feature-stories/detail/thailands-leadership-and-innovation-towards-healthy-ageing. Accessed January 1, 2024.
- Uemura K, Makizako H, Lee S, Doi T, Lee S, Tsutsumimoto K. The impact of sarcopenia on incident homebound status among community-dwelling older adults: a prospective cohort study. Maturitas 2018; 113:26-31. doi: 10.1016/j.maturitas.2018.03.007 [Crossref] [ Google Scholar]
- Health Data Center, Ministry of Public Health. Population Registration: Age and Gender. Fiscal Year 2567. Available from: https://hdcservice.moph.go.th/hdc/reports/report.php?&cat_id = ac4eed1bddb23d6130746d62d2538fd0&id = f83d0cd8b830706dab4cd3cb09afa584. Published June 2024.
- Suriyanrattakorn S, Chang CL. Long-term care (LTC) policy in Thailand on the homebound and bedridden elderly happiness. Health Policy Open 2021; 2:100026. doi: 10.1016/j.hpopen.2020.100026 [Crossref] [ Google Scholar]
- Abdi S, Spann A, Borilovic J, de Witte L, Hawley M. Understanding the care and support needs of older people: a scoping review and categorisation using the WHO international classification of functioning, disability and health framework (ICF). BMC Geriatr 2019; 19(1):195. doi: 10.1186/s12877-019-1189-9 [Crossref] [ Google Scholar]
- Ko Y, Noh W. A scoping review of homebound older people: definition, measurement and determinants. Int J Environ Res Public Health 2021; 18(8):3949. doi: 10.3390/ijerph18083949 [Crossref] [ Google Scholar]
- Lee J, Suh Y, Kim Y. Multidimensional factors affecting homebound older adults: a systematic review. J Nurs Scholarsh 2022; 54(2):169-75. doi: 10.1111/jnu.12724 [Crossref] [ Google Scholar]
- Simionato J, Vally H, Archibald D. Circumstances that promote social connectedness in older adults participating in intergenerational programmes with adolescents: a realist review. BMJ Open 2023; 13(10):e069765. doi: 10.1136/bmjopen-2022-069765 [Crossref] [ Google Scholar]
- Ramraj B, Logaraj M. Is home bound a major burden towards health access among the elderly population? A community based cross sectional study in the selected northern districts in Tamilnadu. Clin Epidemiol Glob Health 2021; 9:132-6. doi: 10.1016/j.cegh.2020.08.002 [Crossref] [ Google Scholar]
- Robertson ML, Phung A, Bhatnagar S, Li L, Schuchman M, Wolff J. Assessing the wellbeing of family caregivers of multimorbid and homebound older adults-a scoping literature review. J Am Geriatr Soc 2023; 71(1):268-75. doi: 10.1111/jgs.18077 [Crossref] [ Google Scholar]
- Schulz R, Beach SR, Czaja SJ, Martire LM, Monin JK. Family caregiving for older adults. Annu Rev Psychol 2020; 71:635-59. doi: 10.1146/annurev-psych-010419-050754 [Crossref] [ Google Scholar]
- Ab Ghani NN, Makhtar A, Syed Elias SM, Ahmad N, Ludin SM. Knowledge, practice and needs of caregiver in the care of older people: a review. Int J Care Sch 2022; 5(3):70-8. doi: 10.31436/ijcs.v5i3.269 [Crossref] [ Google Scholar]
- Meegoda ML, Fernando S, Sivayogan S, Atulomah NO. Exploring the preparedness of family care givers to provide cancer palliative care. Int J Res 2019; 7(6):18-26. doi: 10.29121/granthaalayah.v7.i6.2019.734 [Crossref] [ Google Scholar]
- AARP Public Policy Institute, National Alliance for Caregiving. Caregiving in the United States 2020. AARP. Available from: https://www.aarp.org/pri/topics/ltss/family-caregi-ving/caregiving-in-the-united-states.html.
- Ubenoh US, Bassah N, Palle JN. Development of a training program for family caregivers on home care of older adults in Cameroon. Int J Trop Dis Health 2019; 38(4):1-11. doi: 10.9734/IJTDH/2019/v38i430192 [Crossref] [ Google Scholar]
- Fusch PI, Ness LR. Are we there yet? Data saturation in qualitative research. Qual Rep 2015; 20(9):1408-16. doi: 10.46743/2160-3715/2015.2281 [Crossref] [ Google Scholar]
- Faul F, Erdfelder E, Buchner A, Lang AG. Faul F, Erdfelder E, Buchner A, Lang AGStatistical power analyses using G*Power 31: tests for correlation and regression analyses. Behav Res Methods 2009; 41(4):1149-60. doi: 10.3758/brm.41.4.1149 [Crossref] [ Google Scholar]
- Cohen J. Statistical Power Analysis for the Behavioral Sciences. Lawrence Erlbaum Associates Inc; 1977.
- Burns N, Grove SK. The Practice of Nursing Research: Appraisal, Synthesis and Generation of Evidence. 6th ed. St Louis: Saunders; 2009.
- Holloway I, Wheeler S. Qualitative Research in Nursing and Healthcare. 3rd ed. Oxford: Blackwell; 2010.
- Lincoln YS, Guba EG. Naturalistic Inquiry. Newbury Park, CA: SAGE Publications; 1985.
- Cheng JM, Batten GP, Yao NA. A qualitative study of the social and lived experiences of homebound older adults. J Appl Gerontol 2022; 41(3):744-53. doi: 10.1177/07334648211040383 [Crossref] [ Google Scholar]
- Bassah N, Ubenoh US, Palle JN. An exploratory study of the knowledge and practices of family caregivers in the care of the elderly at home in the Buea health district, Cameroon. J Gerontol Geriatr Res 2018; 7(3):1000473. doi: 10.4172/2167-7182.1000473 [Crossref] [ Google Scholar]
- Supaporn K, Isaramalai SA, Khaw T. Family caregivers’ perceptions of caring for older persons in the palliative care stage at home. Pac Rim Int J Nurs Res 2022; 26(1):161-74. [ Google Scholar]
- Mohammed ZS, Ahmad AM, Farahat HM. Assessment of knowledge and practices regarding elderly care among elderly care givers at geriatric homes. Egypt J Health Care 2022; 13(2):260-9. doi: 10.21608/ejhc.2022.229086 [Crossref] [ Google Scholar]
- Chan KT, Marsack-Topoleswki C, LaFave S, Ratnayake M, Graves J, Fenski D. Teaching note-supporting homebound older adults and caregivers through integrative service learning. J Soc Work Educ 2023; 59(4):1249-57. doi: 10.1080/10437797.2022.2045238 [Crossref] [ Google Scholar]
- Col BK, Kose BG, Basaran AG. The effect of leisure activities on successful aging. Niger J Clin Pract 2022; 25(11):1904-10. doi: 10.4103/njcp.njcp_384_22 [Crossref] [ Google Scholar]
- Campani D, Caristia S, Amariglio A, Piscone S, Ferrara LI, Barisone M. Home and environmental hazards modification for fall prevention among the elderly. Public Health Nurs 2021; 38(3):493-501. doi: 10.1111/phn.12852 [Crossref] [ Google Scholar]
- Lektip C, Chaovalit S, Wattanapisit A, Lapmanee S, Nawarat J, Yaemrattanakul W. Home hazard modification programs for reducing falls in older adults: a systematic review and meta-analysis. PeerJ 2023; 11:e15699. doi: 10.7717/peerj.15699 [Crossref] [ Google Scholar]
- Tuttle D, Griffiths J, Kaunnil A. Predictors of caregiver burden in caregivers of older people with physical disabilities in a rural community. PLoS One 2022; 17(11):e0277177. doi: 10.1371/journal.pone.0277177 [Crossref] [ Google Scholar]
- Burgdorf JG, Arbaje AI, Wolff JL. Training needs among family caregivers assisting during home health, as identified by home health clinicians. J Am Med Dir Assoc 2020; 21(12):1914-9. doi: 10.1016/j.jamda.2020.05.032 [Crossref] [ Google Scholar]
- Guo P, Zhang S, Niu M, Wang P, Li L, Wu C. A qualitative study of the interaction experiences between family caregivers and community nurses for disabled elderly people at home. BMC Geriatr 2023; 23(1):243. doi: 10.1186/s12877-023-03917-y [Crossref] [ Google Scholar]
- Jing LW, Wang FL, Zhang XL, Yao T, Xing FM. Occurrence of and factors influencing elderly homebound in Chinese urban community: a cross-sectional study. Medicine (Baltimore) 2017; 96(26):e7207. doi: 10.1097/md.0000000000007207 [Crossref] [ Google Scholar]
- Schirghuber J, Schrems B. Homebound: A concept analysis. Nurs Forum 2021; 56(3):742-51. doi: 10.1111/nuf.12586 [Crossref] [ Google Scholar]