Journal of caring sciences. 14(3):139-150.
doi: 10.34172/jcs.025.33447
Systematic Review
Nonpharmacological Interventions on Intramuscular Vaccination Pain among Infants: A Systematic Review and Meta-Analysis of Randomized Control Trials
Kurvatteppa Halemani Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Project administration, Supervision, Validation, Visualization, 1, * 
Elsa Vitale Conceptualization, Writing – original draft, Writing – review & editing, 2
Asha Shetty Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Project administration, Supervision, Validation, Visualization, 3
Lata Thimmappa Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Project administration, Supervision, Validation, Visualization, 4
Alwin Issac Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Project administration, Supervision, Validation, Visualization, 3
Vijay VR Formal analysis, Data curation, Investigation, Methodology, Project administration, Resources, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing, 1
Prabhakar Mishra Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Project administration, Supervision, Validation, Visualization, 5
Author information:
1College of Nursing, All India Institute of Medical Sciences (AIIMS), Raebareli UP, India
2Healthcare and Nursing Professions Department, ASL Bari, Bari, Italy
3College of Nursing, All India Institute of Medical Sciences (AIIMS), Bhubaneswar, India
4College of Nursing, All India Institute of Medical Sciences (AIIMS), Kalyani, West Bengal, India
5Department of Biostatistics & Health Informatics, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow, India
Abstract
Introduction:
Vaccination pain is the most common distress for young children and their parents. Non-pharmacological interventions significant impact on vaccination pain in infants. This systematic review and meta-analysis aimed to appraises the evidence concerning the non-pharmacological interventions on vaccine related pain in infants.
Methods:
This study was followed Preferred Reporting Items for Systematic review and Meta-Analysis (PRISMA) statement and recommendation of Cochrane guidelines. Electronic databases, including PubMed, Cumulative Index to Nursing & Allied Health Literature (CINAHL), EMBASE, Web of Science, and Clinical Key, were searched for original trails. Pooled data were analyzed using a random‐effects model with 95% confidence intervals (CIs). The subgroup analysis including breastfeeding, sucrose, kangaroo mother care, massage, heat-cold applications, and pain scales were presented in forest plots using RevMan software 5 version 4.1.
Results:
A total of 1,739 infants were included from 19 trials. Of these, 1,055 infants received interventions, while 684 infants given usual care. Eight trails used breastfeeding as an intervention, standard mean difference (SMD): -3.28. 95% (CI): -4.16 to -2.4, P=0.0, I2=95%. Similarly, six trials employed sucrose [SMD -2.22, CI: -3.68 to -0.75, P=0.0, I2=97%]. Three studies utilized kangaroo mother care (KMC), SMD: -1.1 CI: -2.18 to -0.02, P=0.0, I2=89%) and hot and cold applications [SMD: -1.14, CI: -2.86 to 0.58, P=0.0, I2=95%].
Conclusion:
Noninvasive therapies such as breastfeeding, massage, sucrose, KMC, and hot and cold applications were effective interventions in reducing vaccination pain in infants. Studies have proved that nonpharmacological interventions were ideal and acted as analgesics among children with fewer side effects.
Keywords: Infants, Vaccine, Pain, Pharmacological, Therapeutic interventions
Copyright and License Information
© 2025 The Author(s).
This work is published by Journal of Caring Sciences as an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/). Non-commercial uses of the work are permitted, provided the original work is properly cited.
Funding Statement
None.
Introduction
Children are not merely smaller versions of adults; their developmental needs and requirements differ significantly from those of other age groups. Children have passive immunity, conferred through breastfeeding and immunization. Vaccines serve as preventive measures that contain antibodies or antigens, triggering the body’s natural immune response against specific pathogens.According to the Centres for Disease Control and Prevention (CDC), vaccinations are a crucial public health strategy that protects millions of children from various diseases every year.Immunization is an invasive procedure that may induce pain during and after the injection. Children typically exhibit a higher pain threshold than adults; however, perception of pain, physiological responses, and behavioral manifestations can vary significantly.Certain vaccines, particularly those administered intramuscularly (IM) into the vastus lateralis muscle, are associated with notable discomfort. However, the anterior lateralis site is preferred for infants due to fewer nerves and blood vessels. Vaccines such as Diphtheria, Pertussis, Tetanus (DPT), and Pentavalent are delivered into the largest segment of the vastus lateralis muscle. The pain intensity may escalate six hours following vaccination, and some children may also develop fever.Nevertheless, the pain associated with vaccination can be effectively managed through symptomatic treatment.
Pain management in pediatric populations is frequently neglected, despite its crucial role during painful procedures. There is frequently a divergence of opinions between clinicians and family members regarding the use of pharmaceutical interventions. Additionally, pain management strategies for children are not usually aligned with those used for adults, which can lead to a greater reliance on medications.However, there is currently a lack of standardized guidelines for non-pharmacological interventions aimed at managing pain in children. Prior literature has reported inconsistent findings about the effectiveness of non-pharmacological methods for managing procedural pain in neonates.
In this context, Queiros in 2023 conducted a systematic review to assess the efficacy of non-pharmacological interventions in an alleviating vaccination-related pain in infants. No systematic reviews and meta-analysis conducted to assess the effectiveness of non-pharmacological interventions for relieving vaccination pain. Hence, this systematic review and meta-analysis aimed to evaluate various non-pharmacological strategies, including breastfeeding, sucrose administration, massage, kangaroo mother care (KMC), and the application of hot and cold treatments, for reducing vaccination pain among infants.
Materials and Methods
This systematic review and meta-analysis aimed to appraises the evidence concerning the effectiveness of non-pharmacological interventions on vaccine related pain among infants. The Cochrane Collaboration guidelines were adopted, and reported with using Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) 2020 statement. The review protocol has been registered with PROSPERO (CRD42023476666).
A comprehensive search strategy was formulated using the MeSH words or key terms connected to PICO statement (population or patient, intervention, comparator or control, and outcome) in PubMed and tailored into different databases. Population: Infants visited routine immunization (Hepatitis B, DPT and Pentavalent vaccine); Intervention: non-pharmacological management; Comparison with routine care; Outcomes: vaccine related pain, duration of cry and heart rates. The databases, including PubMed (MEDLINE), Cumulative Index to Nursing and Allied Health Literature (CINAHL), ClinicalKey, Web of Science, EMBASE, and Scopus were searched for relevant articles from inception January, 2008 to September 2023. In addition to this manual search was conducted in tracking citations of references.
The identified articles were imported into Rayyan software, where duplicates were removed using the “check for duplicates” tool.A manual search was carried out to the direction of a citation and references of relevant studies. Observational studies, qualitative studies, case reports, and editorials were excluded. Further full articles were screened based on review criteria. The non-pharmacological intervention was major intervention in randomized control trials (RCTs) with pain reduction was primary outcome and duration of cry and heart rates were secondary outcomes.
Two independent authors (KH, EV) conducted screening of included trials. Any disagreements between the first two authors of the extracted data was referred to the third author (AS) for the final settlement. A retrieved data was presented in data extraction sheet with the following headings, author’s name, country and year of study conducted, sample size, study design, diagnostic criteria, duration of study, study selection criteria, and study outcomes were retrieved.
Search Outcome
The search strategy identified 14539 studies through electronic databases and 15 studies from other media, 2841 duplicate records were excluded. After assessing the titles and abstracts, 11619 studies were omitted, as they did not meet the criteria of the review according to PICO. Again 17 articles were not reviewed, after assessing the full text, another 43 articles were excluded, as they did not match the inclusion criteria of the systematic review and meta‐analysis. The reasons for excluding articles were that the study involved Nonpharmacologic intervention was given in combination with other therapies as an intervention, and the Difference in the primary outcome and inappropriate research methods. Although, an RCT evaluated the effectiveness of non-pharmacological interventions among infants undergoing vaccination. Thus, nineteen articles were involved in narrative synthesis, and meta‐analysis. The flow diagram of study selection process is presented in.
The Cochrane risk of bias tool (ROB-2) was used to evaluate the risk of bias of the included trials. The details regarding the risk of bias of all included trials and judgements about each risk of bias item are presented in Narrative synthesis was carried out and summarized in data extraction form, which included author, year of publication, country, design, sample size, gestational age, and birth weight, age during vaccination, inclusion criteria, exclusion criteria, intervention, name instruments and study outcome.
Interventions and Instruments
The use of pharmaceutical therapy in children can lead to increased adverse effects. Therefore, non-pharmacological interventions are often preferred for children due to their fewer side effects. For instance, breastfeeding is commonly offered as a natural source of comfort for newborns during painful procedures. In addition to breastfeeding, several randomized controlled trials (RCTs) have examined non-pharmacological interventions for pain management, including sucrose solutions, skin contact, massage, heat and cold applications, and flicking. In contrast, the control group received standard care after vaccinations. This review utilized various standardized scales namely Neonatal Infant Pain Scale (NIPS), Face, Legs, Activity, Cry, and Consolability (FLACC) scale, Douleur Aiguë Nouveau-né (DAN scale). Adventure Behavior Seeking Scale (ABSS scale) and Wisconsin Children’s Hospital (UWCH, scale) to assess the severity of pain experienced by infants during vaccinations.
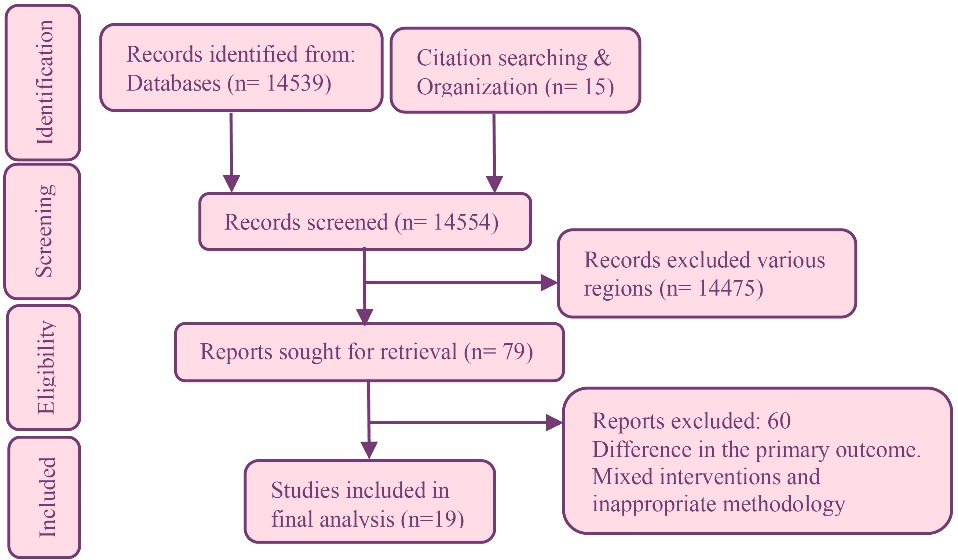
Figure 20.
Flow diagram of study
.
Flow diagram of study
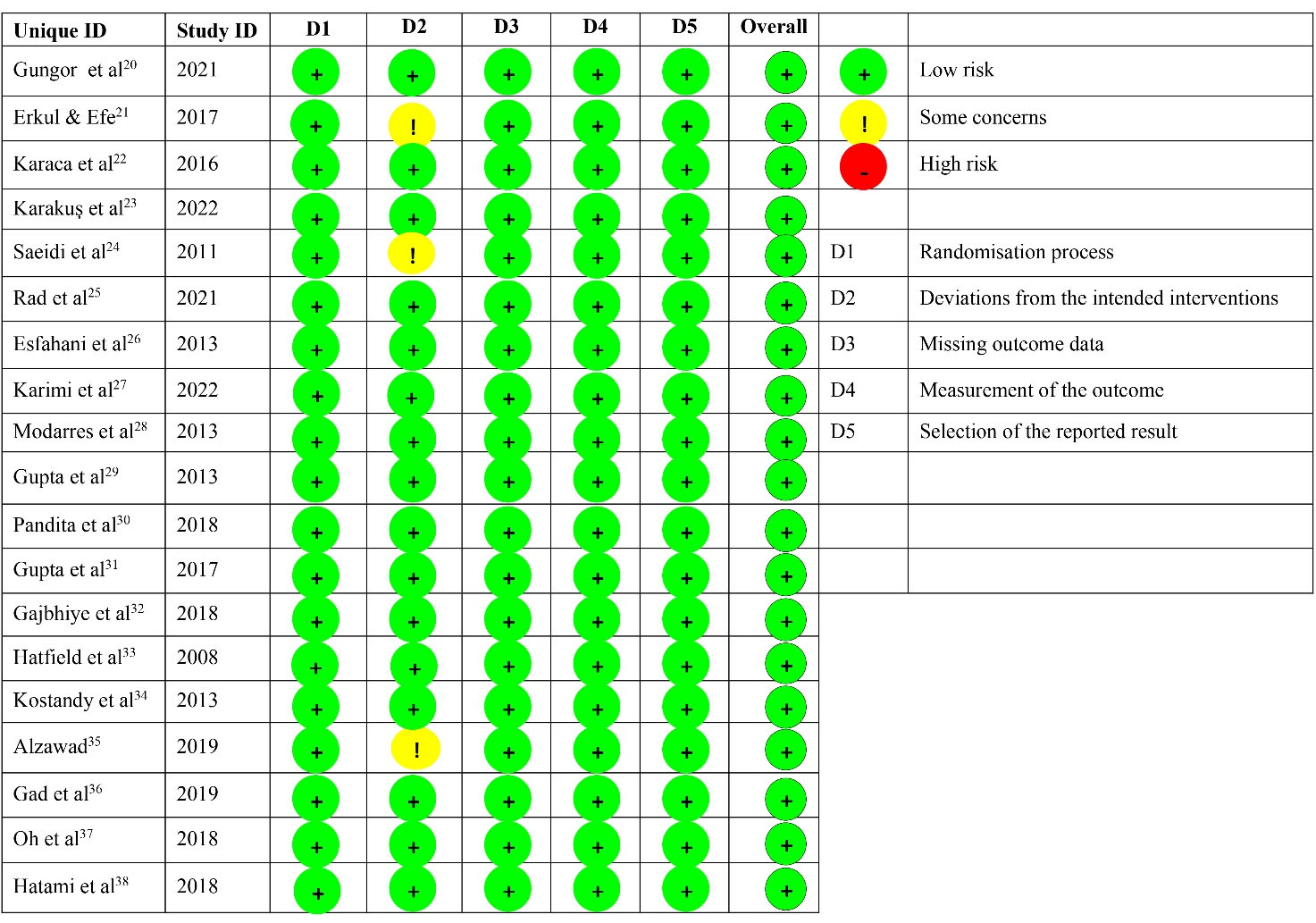
Figure 21.
The risk of bias assessment
.
The risk of bias assessment
Statistical Analysis
The included studies were coded and entered into the Microsoft Excel spreadsheet before being transferred to RevMan software Version 4.4.1. The individual study mean difference and weights were calculated by standardized mean difference (SMD) after adjusting standard deviation. Heterogeneity among studies was assessed using the I2 test, categorizing the I2 values as high ( > 75%), medium (50-75%), and low ( < 50%) heterogeneity. (20) A random effects model was employed due to the observed heterogeneity. SMDs were calculated with 95% confidence intervals (95% CI) for continuous variables reported in forest plots. The heterogenicity was minimize through subgroup analysis of primary (vaccination pain) and secondary outcomes (duration of cry and heart beats). The pooled data were analyzed and reported using RevMan 5 software version 4.1 (The Cochrane Collaboration, 11-13 Cavendish Square, London, W1G 0AN, United Kingdom) and Stata software 17 (StataCorp LLC, Lakeway Drive, College Station, Texas, USA).
Table 1.
Study characteristics
|
Name of authors, year & Country
|
Research design
|
Sample size
|
GA/ BW/present age in months/vaccine & site
|
Study criteria
|
Interventions
|
Pain assessment scales and cut off scores
|
The quality
of a body of
evidence and grading *
|
| Güngör et al 2021, Turkey |
RCT |
T:96 EG1:31 EG2:32 CG:33 |
38-38.6 weeks/NR/2-4/Pneumococcal/IM |
Healthy infants who on EBF visited family healthcare centers for routine vaccinations. |
EG1: Heat & cold application given. CG: As usual care given |
FLACC Mild: 0 4; Moderate: 5-6 Severe: 7-10. |
High |
| Erkul & Efe 2017, Turkey |
RCT |
T:100 EG:50 CG:50 |
38-42 weeks/2.5 kg/2/ DPT or Hep-B/ IM |
The mothers were agreed to breastfeeding for 30 minutes prior to vaccination. |
EG: BF & sucrose given simultaneously during vaccination. CG: Usual care given during vaccination. |
NIPS Mild = 1-3 Moderate = 4-6 Severe = 7-10 |
Moderate |
| Karaca Ciftci et al 2016, Turkey |
RCT |
T = 70 EG = 35 CG = 35 |
37-42 weeks/3.4 kg/30-42 days/Hep B/IM |
Infants without pain medication before vaccination were included. Preterm were excluded. |
EG; The muscle was held with the nurse’s left hand, area was flicked with the right-hand during vaccination.CG: Usual care |
NIPS mild = 1-3 moderate = 4-6 severe = 7-10 |
High |
| Karakuş Türker and Gözen 2022, Turkey |
RCT |
T = 70 EG = 35 CG = 35 |
37-42 weeks/2.5- 4 kg/1 day/Hep-B/IM |
Full-term with normal Apgar were included. Preterm with skin lesions were excluded. |
EG:BF given during vaccination.CG: Skin-to-skin contact with their mothers |
NIPS Mild = 1-3 Moderate = 4-6 Severe = 7-10 |
High |
| Saeidi et al 2011, Iran |
RCT |
T = 60 EG:30 CG:30 |
37-42 weeks/2.5 to 4 kg /NR/ DPT/Hep/IM |
Healthy infants with normal Apgar scores who had not been fed for the last 30 minutes were included. |
EG: Infants to the mother chest for skin to skin contact for 2 minutes before & 3 minutes after vaccination.CG: Usual care |
NIPS Mild = 1-3 Moderate = 4-6 Severe = 7-10 |
High |
| Akbarian Rad et al 2021, Iran |
RCT |
T = 90 EG1:30 EG2:30 CG:30 |
28-37 weeks/2.5 kg.(Avg)/3/Hep B/IM |
Parents who willing to give consent were included. Infants w received sedatives were excluded. |
EG1:2ml mother breast milk exposed that stimulated through smell.CG:2 ml of distilled water. |
PIPPMild:0-6 Moderate:7-12 Severe:13- 21 |
High |
| Savabi Esfahani et al2013, Iran |
RCT |
T = 96 EG1:32 EG2:32 CG:32 |
NR/NR/6-12/ Hep B/IM |
Infant seeking routine vaccination were included. Infants who cry prior to vaccination or open wounds were excluded. |
EG1: BF given during vaccination.EG2: Massage of the middle or ring finger of the infants’ palm or sole of the injected side for 60 sec.CG: Usual care |
NIPS Mild = 1-3 Moderate = 4-6 Severe = 7-10 pain. |
High |
| Karimi et al2022, Iran |
RCT |
T = 171 EG1 = 55 EG2 = 57 CG = 59 |
NR/NR/4/ Pentavalent/IM |
Healthy infants not received analgesics for the past 48 h were included. The parents unwilling to provide consent were excluded. |
EG1: BF given before vaccination EG2(SS):2cc Dextrose 50% was slowly poured during vaccination. CG: Usual care |
MBPS A total score ranged from 0-8. Higher score increases pain intensity. |
High |
| Modarres et al2013, Iran |
RCT |
T = 130 EG = 65 CG = 65 |
37-42 weeks/2.5-4 kg /1 day/ Hep B/IM |
Infants with normal Apgar & being EBF were included. Infants with congenital anomalies were excluded. |
EG: Neonates were BF during two minutes before, during, & after Hep B vaccination. CG: Usual Care |
DAN. Higher score indicates pain. |
High |
| Gupta et al2013, India |
RCT |
T:96 EG1:33 EG2:31 CG -32 |
NR/NR/3/ DPT/IM |
EBF infants were came for routine vaccination. Prenatal, perinatal asphyxia, & infants with medical illness were excluded. |
EG1: BF & 1 g of EMLA cream applied.EG2: 1 g of EMLA cream with 2 ml distilled water given.CG: One gram of placebo cream applied at vaccine site prior 2 minutes. |
MFCS Mild = 1-3 Moderate = 4-6 Severe = 7-10 |
High |
| Pandita et al2018, India |
RCT |
T = 61 EG = 32 CG = 29 |
37.7 weeks/2.9 kg/1/ DPT/IM |
Healthy Infants referred for immunization were included. Birth asphyxia, who received analgesics were excluded. |
EG: The skin-to skin contact, prior and during vaccination, and after 5 min post vaccination.CG: Usual care |
NIPS T = 0-7 Mild = 1-3 Moderate = 4-6 Severe = 7-10 |
High |
| Gupta et al2017, India |
RCT |
T:90 EG1:30 EG2:30 CG:30 |
> 37/NR/1.7/DPT/IM |
Infants on EBF came for vaccination. Similarly, delayed cry, birth asphyxia & IUGR were excluded. |
EG1: BF & 1 g of EMLA cream was applied at vaccine site prior 2min.EG2: 1 g of EMLA cream with 2 ml distilled water CG:1 g of placebo cream. |
MFCS and NIPS, Mild = 1-3 Moderate = 4-6 Severe = 7-10 |
High |
| Gajbhiye et al2018, India |
RCT |
T = 150 EG1 = 50 EG2:50 CG = 50 |
37-42 weeks/2.59 to 2.73 kg/1-2 day/ Hep B/IM |
Infants on EBF & parents given consent were included. Formula-fed infants & exposed to opioids were excluded. |
EG1: A 1 mL of 25%oral sucrose EG2:BF was started two minutes prior to vaccination and continued till the end of injection.CG: Usual care |
PIPP Mild:0-6 Moderate: 7-12 Severe: 13- 21 |
High |
| Hatfield et al2008, USA |
RCT |
T = 83 EG = 38 CG = 45 |
37-42 weeks/2.5 kg/ 2 – 4/ Hep-B/IM |
Infants with no sign’s illness were included. Infants who fed or using pacifiers were excluded. |
EG: Oral sucrose solution (0.6 mL/kg) was calculated based on BW given prior vaccination.CG: Usual care |
UWCH Higher scores indicate pain. |
Moderate |
| Kostandy et al2013, USA |
RCT |
T-36 EG = 17 CG = 19 |
39.7 weeks /3.3 kg/1-2 days/Hep B/IM |
Healthy infants with normal Apgar scores whose parents consented to participate were included, |
EG: neonates were placed prone and skin to skin on their mother’s chest in her bed CG: Usual care. |
ABSS Mild:0 4; Moderate: 5-6; Severe: 7 -10. |
High |
| Alzawad 2019, Saudi Arabia |
RCT |
T:60 EG1:20 EG2:20 CG:20 |
NR/NR/2 – 12/ DPT or Hep-B/ IM |
Infants scheduled for routine immunization & without illnesses were included. |
EG1: BF given before during vaccination. EG2: Sucrose solution given before during vaccination.CG: Sterile water given. |
FLACC Mild:0 4Moderate: 5-6 Severe: 7 -10 |
Moderate |
| Gad et al 2019, Egypt |
RCT |
T = 120 EG1 = 40 EG2 = 40 CG = 40 |
NR/NR/NR/DPT/IM |
Healthy breastfed infants came for vaccination were included. Infants who received analgesics in the 24 hours prior to vaccination were excluded |
EG1: Initiate BF 1 min before & continue throughout the procedure. EG2: Administered 2 mL 25% sucrose in same manner.CG: Administering 2 mL sterile water 1 min before injection |
FLACC Mild:0 4 Moderate: 5-6 Severe: 7 -10 |
High |
| Oh et al 2018, Korea |
RCT |
T = 116 EG1;29 EG2:30 EG3:30 CG = 27 |
39weeks/3.2 kg/1day/ Hep B/IM |
Infants with normal Apgar score were included, Infants with repeated serum glucose monitoring, were excluded. |
EG1: 10% dextrose (1 mL), EG2:20% dextrose, EG3:40% dextrose solution given during vaccination.CG: Sterile water |
NFCS, NIPS, and PIPP scales in all groups. Higher scores increase pain intensity. |
High |
| Hatami Bavarsad et al 2018, Iran |
RCT |
T = 50 EG = 25 CG = 25 |
39.1 weeks/3.1 kg/1 day/ Hep B/IM |
Infants with normal Apgar & BF prior 2 hours were included. Infants with congenital anomalies excluded |
EG: BF given prior, during vaccination CG: routinely care. |
DAN Higher score indicates pain. |
High |
Abbreviations: RCT: randomized control trials, T: total, EG: Experimental group, CG: Control group. BF: breast feeding, H/o: History of. IM: intra muscular, NR: not reported: DPT: Diphtheria, Pertussis & Tetanus, EBF: exclusively breastfed; NIPS: Neonatal Infant Pain Scale, MFCS: Modified Neonatal Facial Coding Score, UWCH: University of Wisconsin Children’s Hospitals: sensorial saturation, DAN: Douleur Aiguë du Nouveauné, ABSS: Abstainers Behavioral State Scale. PIPP: Premature Infant Pain Profile
* High grading: Further research is very unlikely to change confidence in the estimate of effect. Moderate: Further research is likely to have an important impact on confidence in the estimate of effect and may change the estimate. Low: Further research is very likely to have an important impact on confidence in the estimate of effect and is likely to change the estimate. Very low: Any estimate of effect is very uncertain
Results
This systematic review and meta-analysis included 19 original RCTs that evaluated the effectiveness of non-pharmacological interventions in reducing vaccination pain among infants . A total of 1739 infants visited health centers for routine vaccination, out of which 1055 received non-pharmacological interventions, while 684 infants in control group received standardized care. The gestational age of infants ranged from 28 weeks to 42 weeks, and their birth weight ranged from 2.5 kg to 4 kg. The age of infants during vaccination ranged from 24 hours to 4 months, and all of them received intramuscular vaccines like hepatitis B, DPT, and pentavalent vaccine. Most studies used breastfeeding as an intervention in experimental groups, followed by sucrose solution, skin-to-skin contact, massage, heat and cold application, and flip application. The primary outcome of the included studies was vaccination pain. The original RCTs were conducted in different parts of the world, including Turkey,Iran,India, USA,Saudi Arabia,Egypt, Korea,respectively.
Eleven studies evaluated the effectiveness of breastfeeding on vaccine pain in infants. The study included 430 infants in the intervention group and 434 infants in the control group. This meta-anslysis was carried out based on standard mean difference(SMD) of vaccine related pain at 95% confidence intervals(CI) [SMD(95% CI) -3.28(-4.16,-2.4),p=0.0, I2=5%].Similarly, six studies evaluated the effectiveness of sucrose solution on vaccine pain before and during vaccination, the intervention group received 1-3 mL drops of sucrose solution. The intervention group has a lower pain threshold than the control group
[SMD, (95% CI)] [-2.22 (-3.68, -0.75), P = 0.0, I= 97%].Three studies evaluated the effectiveness of KMC. The review found that skin to skin contact reduced pain threshold in infants [SMD, (95% CI)] [-1.1 (-2.18, -0.02), P = 0.0, I= 89%].Another study reported hot and cold application [SMD, (95% CI)] [-1.14 (-2.86,0.58), P = 0.0, I = 95%]. The intervention group reported using the massage and flick application reduced the vaccination pain into 0.85 and 1 times, respectively. Overall subgroup analysis revealed that nonpharmacological interventions more effective and found statically significant to reduce vaccination in infants [SMD, (95% CI)] [-2.36 (-2.91, -1.8), P = 0.00, I = 95%] .
Four studies examined the effectiveness of breastfeeding and sucrose solution on vaccine pain.36 A total of 332 patients took part in the review, with 165 infants in the breastfeeding groups and 167 sucrose groups. The findings revealed that breastfeeding was a more effective intervention in reducing pain in the intervention group and was statistically significant. [SMD, (95% CI)] [-0.35(-1.21, 0.5), P = 0.00, I= 93%]. Compared to the KMC and massage groups, breastfeeding is an effective intervention in reducing infants’ pain. The reduction of vaccine pain that is 0.16 times in KMC group and 0. 55 times massage group .
Various pain assessment scales were used to evaluate infants’ pain. Of this, nine studies employed NIPS, with higher scores indicating greater pain. However, non-pharmacological interventions have been found to be effective intervention. [SMD, (95% CI)] [-1.72(-2.41, -1.04), P = 0.00, I = 92%].Similarly, four studies used Face, Legs, Activity, Cry, and Consolability (FLACC) scale [SMD, (95% CI)] [-0.97(-1.95, -0.01), P = 0.00, I= 86%], two studies used Douleur Aiguë Nouveau-né (DAN scale) [SMD, (95% CI)] [-4.41(-8.75, -0.07), P = 0.00, Ieach of study reported Adventure Behavior Seeking Scale (ABSS scale) [-1.00 (-1.70, -0.31)] and Wisconsin Children’s Hospital (UWCH, scale) [-2.31(-2.88, -1.75)] for assessing infants’ pain. The intervention group reduced pain threshold than control group .
Ten studies looked at the impact of non-pharmacological interventions on the duration of cry in infants during vaccination. Duration of cry was reduced in intervention group than control group [SMD, (95% CI)] [-1.99(-2.82, -1.15), P = 0.00, I = 95%]. Further, reduced heart rates in intervention group than control group [SMD, (95% CI)] [-4.31 (-6.35, -2.26), P = 0.00, I = 96%].Overall subgroup analysis revealed that nonpharmacological management is an effective intervention on vaccination pain and was found statistically significant [SMD, (95% CI)] [-2.47 (-3.25, -1.69), P = 0.00, I = 96%].
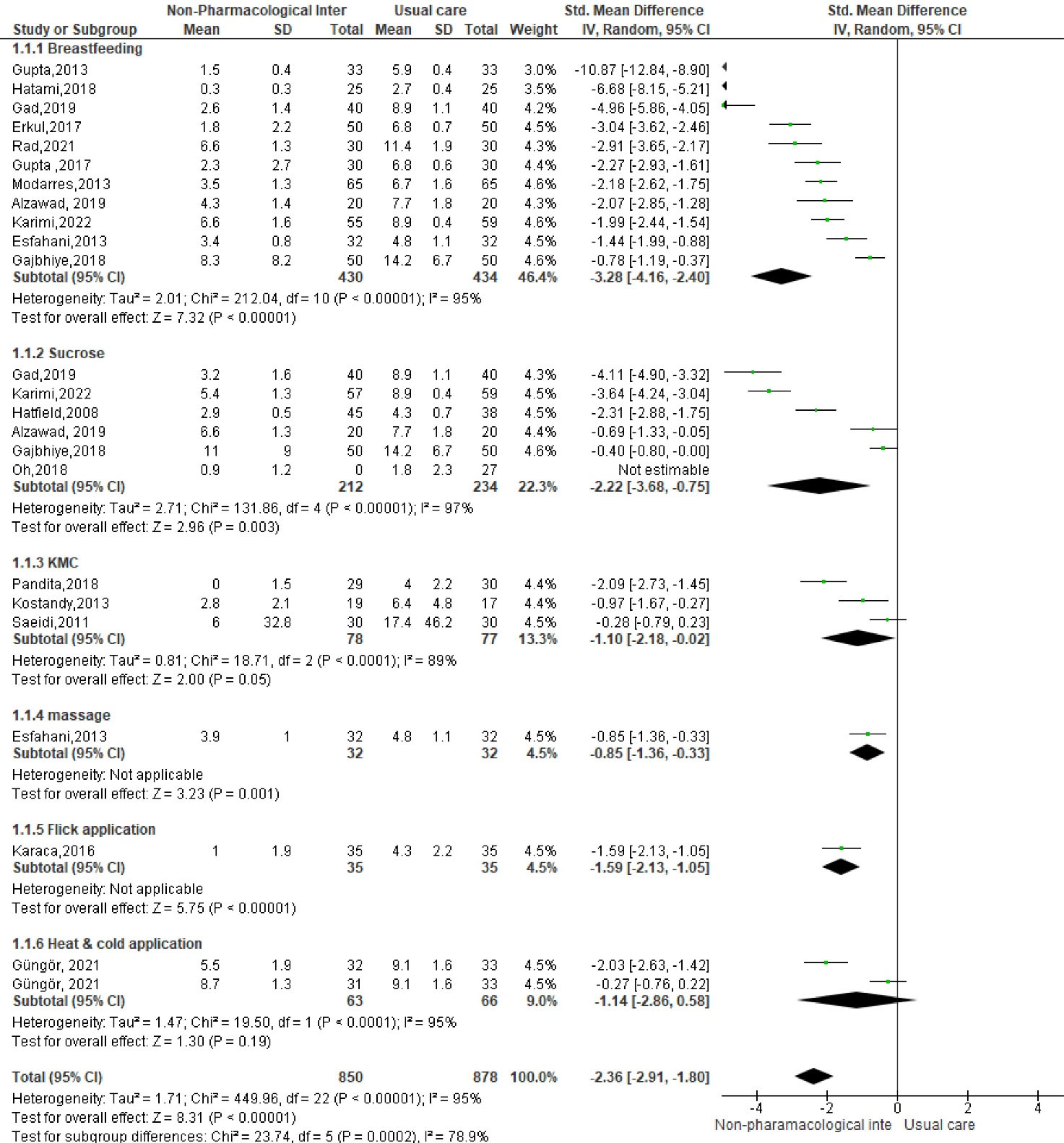
Figure 22.
Forest Plot for no pharmacological interventions
.
Forest Plot for no pharmacological interventions
Meta-regression
Regression analysis of meta-analysis was performed to understand the relationship between effect sizes and covariates. Non pharmacological intervention is a moderator and residual heterogeneity was calculated using random effects. The I2 value was 98.05%, indicating a heterogeneity among the studies. Conversely, the R2 value assesses the proportion of variance explained by the study variables. The Chi-square (χ2) value was 2.00, with a p-value of 0.008 and suggested that the regression model fit is equivalent to the z test, where the χ2 value is the square of the Z value. Additionally, 7.66% of the variance between studies was accounted. The regression coefficient for non-pharmacological interventions was 0.352, and the intercept was 3.41, respectively. The test statistic for residual heterogeneity (Qres) was 451.88 with a P value of 0.000, further indicating significant heterogeneity among the residuals. Hence present meta-analysis confirmed that random effect model appropriate to address heterogenicity.
Galbraith Plots
The Galbraith plot is a graphical representation that illustrates study-specific effect sizes and their precisions, as well as the overall effect size, while also helping to detect potential outliers. The plot features two horizontal lines: the green line represents the reference line, indicating no effect, while the red line is the regression line. The slope of the red line reflects the overall effect size and the standardized log risk ratio for each study. Circles above the green line indicate an increased risk in the intervention groups. However, no studies were reported above the reference line in this analysis. In the present meta-analysis, most circles were found within the shaded region, except for one study, which suggested that the included studies appeared within 95% of the CI. The Galbraith plot concluded that the majority of studies are appeared inside shaded region, indicating considerable heterogeneity among the effect sizes in the present meta-analysis. .
The study did not find any evidence of publication bias, as determined by Begg’s and Egger’s tests. Details of the publication bias of individual studies was conducted in Stata software and reported in (P > 0.53, i.e., when P value is more than 0.05 implicates low publication bias).
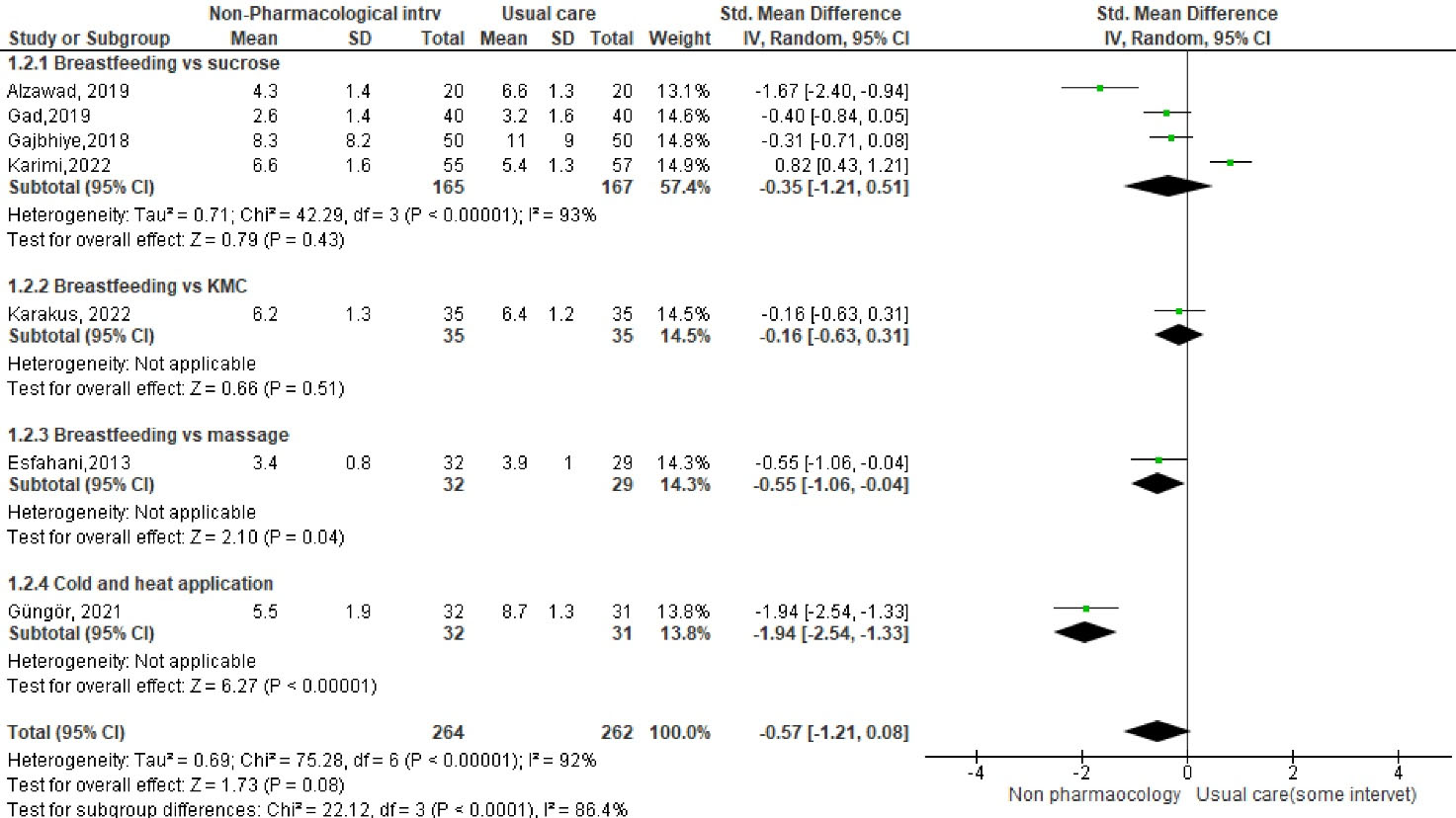
Figure 23.
Forest Plot for effectiveness of breastfeeding and sucrose solution on vaccine pain
.
Forest Plot for effectiveness of breastfeeding and sucrose solution on vaccine pain
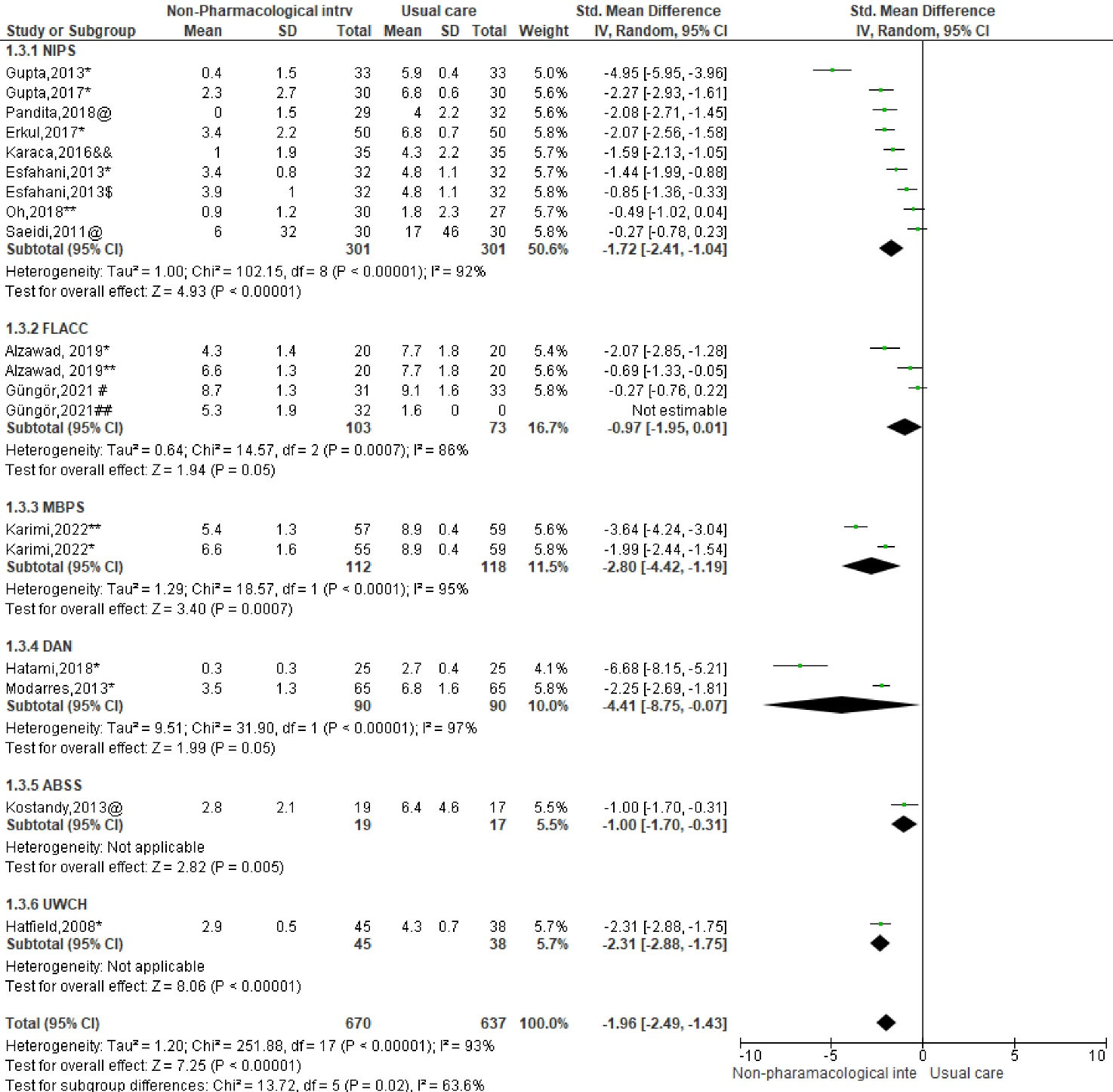
Figure 24.
Forest Plot for infants’ pain
.
Forest Plot for infants’ pain
Discussion
Overall, this systematic review and meta-analysis involving recent RCTs highlighted nonpharmacologic interventions on management of vaccination pain Infants have unique needs and require special attention as they are not simply miniature versions of adults. For this reason, early detection and management of health ailments are essential for their well-being.
It is important to note that minor invasive procedures are performed at the same time or when child in awake. Thus, this approach reduces unnecessary infant disturbance and enhances general health and sleep quality. Although, pain is the unpleasant sensory and emotional experience associated with real or perceived tissue injury. Infants often exposed minor invasive procedures like immunization and routine health checkup.Children definitely do not perceive pain the same way as adults, as their emotional experience is differed than the other age groups. Thus, assessment and management of pain is always challenging to the healthcare workers.
Non-pharmacological management strategies, such as breastfeeding, can provide analgesic effects on children. Present meta-analysis showed that infants in the breastfeeding group experienced less pain (SMD: 3.28) during vaccinations compared to the control group. Therefore, breastfeeding acts as a natural analgesic without any side effects on infants.At present, there are no established protocols for evaluating and treating pain in children. Our research has shown that administering a sucrose solution reduces an infant’s pain (SMD 2.22) times compared to the control group. Therefore, it is necessary to determine the optimal dosage and concentration of sucrose for different conditions to effectively alleviate pain in children. Beside this, KMC is most useful for preterm and helps to improve the emotional bond between the mother and child. Skin to skin contact reduced pain perception of newborn during and after minor invasive procedures. Our review found that infants in KMC group reduced the pain (SMD: 1.1) than control group. Similarly, heat and cold application, massage and flip application act like analgesic effects. Compare to the other non-pharmacological interventions breastfeeding is most efficient analgesics effects.When compared between breastfeeding and sucrose solution, breastfeeding group reduced the pain (SMD: 0.35), similarly in KMC, breastfeeding reduced the (SMD: 0.16), massage group (SMD: 0.55). Although, cold application reduced the pain threshold (SMD: 1.94) than heat application.
In addition, non-pharmacological interventions impact on the duration of cry and heart rates. Although these components are usually included in pain assessment scales.It appears that the duration of cry was longer in the control group compared to the intervention group. Additionally, the heart rate was reduced in the intervention group during and after vaccination.
Primary studies of existing review employed different pain assessment tools based on development age. However, selection of appropriate pain assessment scale is important that yield accurate information. Education and regular skill training on pain management can positively impact on children. Additionally, parents allowed to involved in their child’s care and can promote a sense of trust between the child and healthcare provider.
This is the first systematic review and meta-analysis that assesses the effectiveness of non-pharmacological interventions in reducing intramuscular vaccination pain among infants. The strengths of this review are that all the data retrieved from RCTs were published in reputable journals. However, this review has some limitations. Most of the RCTs did not report the time and duration of interventions, and failed to report criteria for controlling extraneous variables. Lastly, the authors did not state the validity, reliability, sensitivity, and specificity of data collection instruments in their studies.
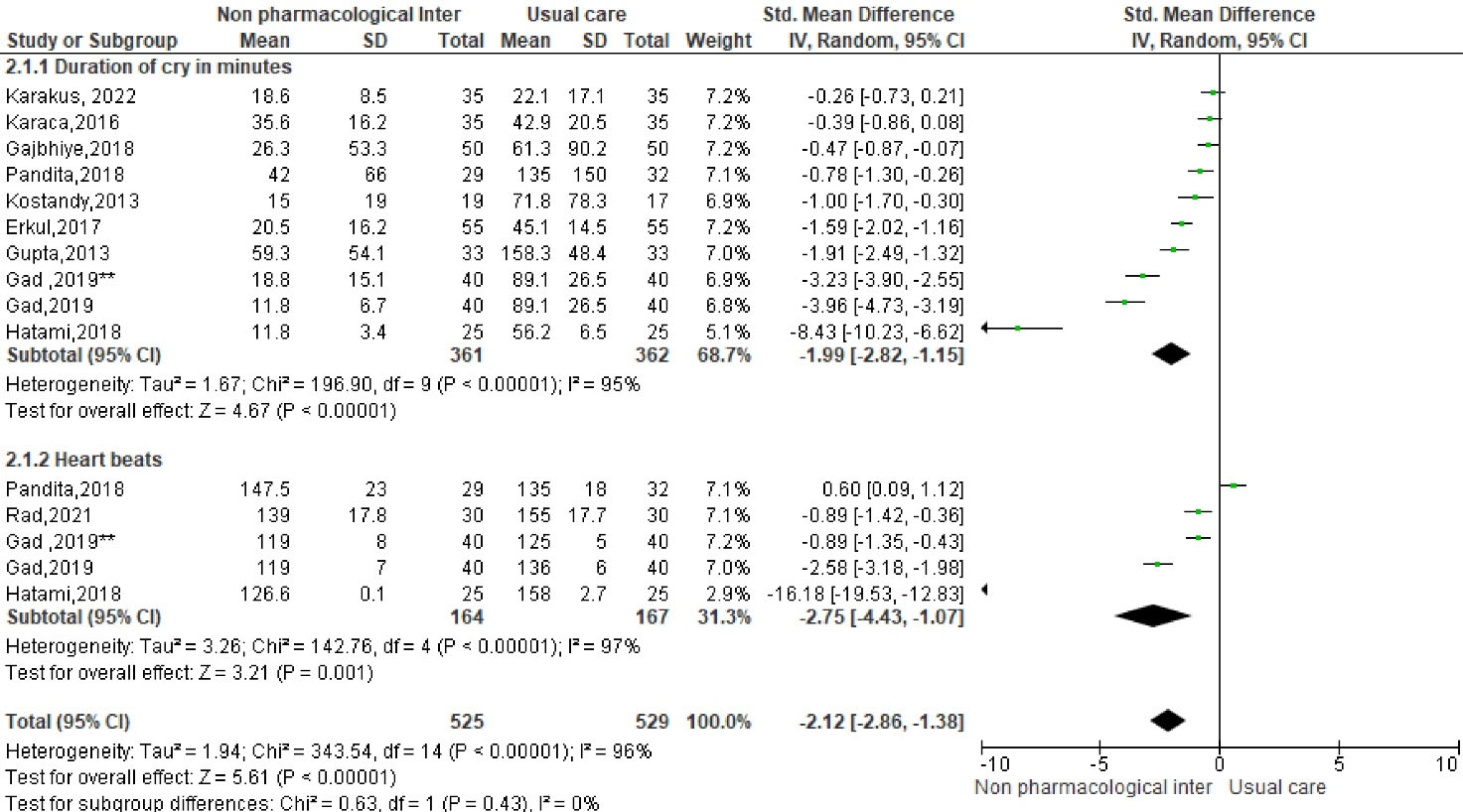
Figure 25.
Forest Plot for nonpharmacological management
.
Forest Plot for nonpharmacological management
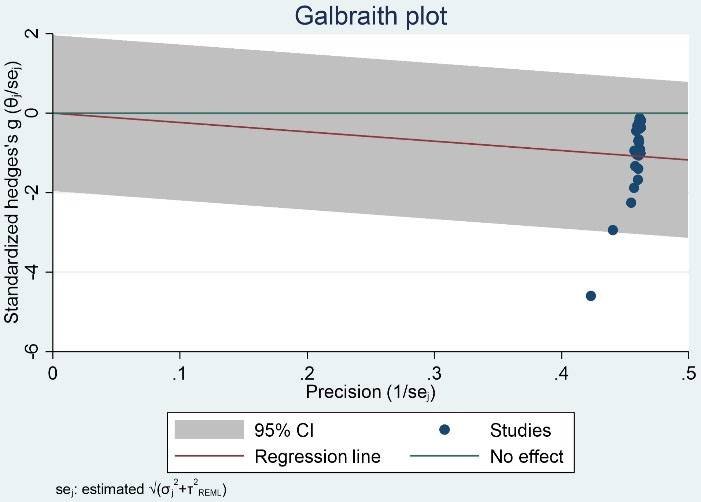
Figure 26.
Galbraith plots: explain the study-specific affect sizes, there precisions, the overall affect size, and detecting potential outliers
.
Galbraith plots: explain the study-specific affect sizes, there precisions, the overall affect size, and detecting potential outliers
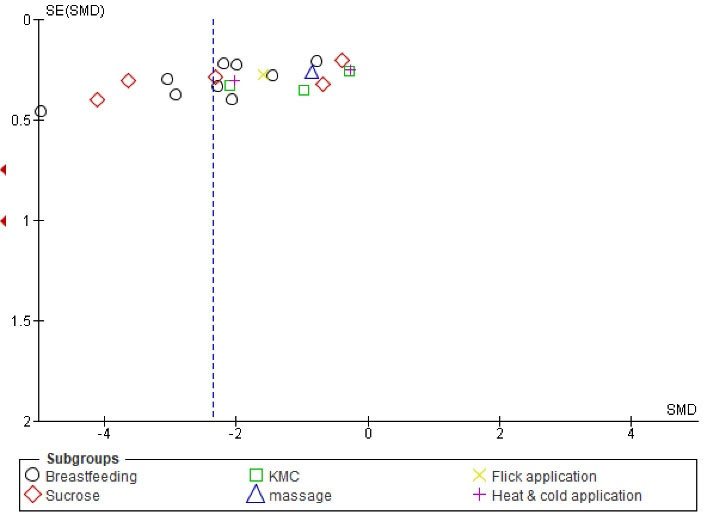
Figure 27.
Begg’s and Egger’s plots
.
Begg’s and Egger’s plots
Table 2.
Meta-regression
|
Effect size (meta_es)
|
Coefficient
|
Standard error
|
z
|
P
>|z|
|
[95% conf. interval]
|
| Non- pharmacological interventions |
0.3525542 |
0.2041004 |
1.73 |
0.084 |
-0.0474753 0.7525837 |
| _cons |
-3.413996 |
0.751591 |
-4.54 |
0.000 |
-4.887087 -1.940905 |
Test of residual homogeneity: Q_res = chi2 (22) = 451.88 Prob > Q_res = 0.000
Method: REML Random-effects meta-regression, Number of obs: 24, tau2 = 4.28, I (%) = 98.05, R-squared (%) = 7.66, Wald chi2 (1) = 2.98, Prob > Chi2: 0.008.
Conclusion
Non-invasive therapies, such as breastfeeding, sucrose solution, and skin-to-skin contact, have been found to have analgesic effects among children. These nonpharmacological interventions are safe and have fewer side effects than pharmacological management. The present study reviews that breastfeeding is the most effective intervention for minor procedural pain management.
Competing Interests
Authors declare none conflict of interest.
Data Availability Statement
Data are available upon reasonable request at the First Author.
Ethical Approval
Not applicable.
Research Highlights
What is the current knowledge?
-
Children are not miniatures of their adults;
-
The threshold of pain perception, body response, and behaviour patterns varied more in children than adults.
-
The appraisal of evidence concerning the effectiveness of non-pharmacological interventions on vaccine related pain in infants are scarcely unexplored.
What is new here?
-
Noninvasive therapies such as breastfeeding, massage, sucrose, KMC, and hot and cold applications were effective interventions in reducing vaccination pain in infants;
-
Studies have proved that nonpharmacological interventions were acted as analgesics among children with fewer side effects.
References
- Simon AK, Hollander GA, McMichael A. Evolution of the immune system in humans from infancy to old age. Proc Biol Sci 2015; 282(1821):20143085. doi: 10.1098/rspb.2014.3085 [Crossref] [ Google Scholar]
- Favaloro EJ, Lippi G. Translational aspects of developmental hemostasis: infants and children are not miniature adults and even adults may be different. Ann Transl Med 2017; 5(10):212. doi: 10.21037/atm.2017.04.18 [Crossref] [ Google Scholar]
- Pettigrew ZJ, Kim M, Becker-Dreps S. Vaccines and immunization. In: Daaleman TP, Helton MR, eds. Chronic Illness Care: Principles and Practice. Cham: Springer International Publishing; 2023. p. 155-79. 10.1007/978-3-031-29171-5_12
- Ford A, Hwang A, Mo AX, Baqar S, Touchette N, Deal C. Meeting summary: global vaccine and immunization research forum, 2021. Vaccine 2023; 41(11):1799-807. doi: 10.1016/j.vaccine.2023.02.028 [Crossref] [ Google Scholar]
- Balasundaram P, Sakr M. Understanding and application of CDC immunization guidelines. In: StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; 2025.
- Kim Y, Kim JH. Using photos for public health communication: A computational analysis of the Centers for Disease Control and Prevention Instagram photos and public responses. Health Informatics J 2020; 26(3):2159-80. doi: 10.1177/1460458219896673 [Crossref] [ Google Scholar]
- Schmitz AK, Vierhaus M, Lohaus A. Pain tolerance in children and adolescents: sex differences and psychosocial influences on pain threshold and endurance. Eur J Pain 2013; 17(1):124-31. doi: 10.1002/j.1532-2149.2012.00169.x [Crossref] [ Google Scholar]
- Ogden SA, Ludlow JT, Alsayouri K. Diphtheria tetanus pertussis (DTaP) vaccine. In: StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; 2025.
- Hall LM, Ediriweera Y, Banks J, Nambiar A, Heal C. Cooling to reduce the pain associated with vaccination: a systematic review. Vaccine 2020; 38(51):8082-9. doi: 10.1016/j.vaccine.2020.11.005 [Crossref] [ Google Scholar]
- Mathews L. Pain in children: neglected, unaddressed and mismanaged. Indian J Palliat Care 2011; 17(Suppl):S70-3. doi: 10.4103/0973-1075.76247 [Crossref] [ Google Scholar]
- Campbell-Yeo M, Eriksson M, Benoit B. Assessment and management of pain in preterm infants: a practice update. Children (Basel) 2022; 9(2):244. doi: 10.3390/children9020244 [Crossref] [ Google Scholar]
- Rahayu TG, Sumartini R, Susila A. Comparison of cold and warm compresses influence toward pain in patients with extremity fractures. In: Selection and Peer-Review Under the Responsibility of the ICHT Conference Committee. KnE Life Sciences; 2019. p. 326-33. 10.18502/kls.v4i13.5262
- Halemani K, Issac A, Mishra P, Dhiraaj S, Mandelia A, Mathias E. Effectiveness of preoperative therapeutic play on anxiety among children undergoing invasive procedure: a systematic review and meta-analysis. Indian J Surg Oncol 2022; 13(4):858-67. doi: 10.1007/s13193-022-01571-1 [Crossref] [ Google Scholar]
- Cignacco E, Hamers JP, Stoffel L, van Lingen RA, Gessler P, McDougall J. Cignacco E, Hamers JP, Stoffel L, van Lingen RA, Gessler P, McDougall J, et alThe efficacy of non-pharmacological interventions in the management of procedural pain in preterm and term neonatesA systematic literature review. Eur J Pain 2007; 11(2):139-52. doi: 10.1016/j.ejpain.2006.02.010 [Crossref] [ Google Scholar]
- García-Valdivieso I, Yáñez-Araque B, Moncunill-Martínez E, Bocos-Reglero MJ, Gómez-Cantarino S. Effect of non-pharmacological methods in the reduction of neonatal pain: systematic review and meta-analysis. Int J Environ Res Public Health 2023; 20(4):3226. doi: 10.3390/ijerph20043226 [Crossref] [ Google Scholar]
- Dhiraaj S, Thimmappa L, Issac A, Halemani K, Mishra P, Mavinatop A. The impact of early enteral nutrition on post-operative hospital stay and complications in infants undergoing congenital cardiac surgery: a systematic review and meta-analysis. J Caring Sci 2023; 12(1):14-24. doi: 10.34172/jcs.2023.31750 [Crossref] [ Google Scholar]
- Queirós I, Moreira T, Pissarra R, Soares H, Guimarães H. Non-pharmacological management of neonatal pain: a systematic review. Minerva Pediatr (Torino) 2023; 75(2):282-95. doi: 10.23736/s2724-5276.22.06871-9 [Crossref] [ Google Scholar]
- Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011; 343:d5928. doi: 10.1136/bmj.d5928 [Crossref] [ Google Scholar]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021; 372:n71. doi: 10.1136/bmj.n71 [Crossref] [ Google Scholar]
- Güngör T, Öztürk Şahin Ö. Analysis of two non-pharmacological pain management methods for vaccine injection pain in infants: a randomized controlled trial. Agri 2021; 33(1):15-22. doi: 10.14744/agri.2020.54289 [Crossref] [ Google Scholar]
- Erkul M, Efe E. Efficacy of breastfeeding on babies’ pain during vaccinations. Breastfeed Med 2017; 12:110-5. doi: 10.1089/bfm.2016.0141 [Crossref] [ Google Scholar]
- Karaca Ciftci E, Kardas Ozdemir F, Aydın D. Effect of flick application on pain level and duration of crying during infant vaccination. Ital J Pediatr 2016; 42:8. doi: 10.1186/s13052-016-0218-y [Crossref] [ Google Scholar]
- Karakuş Türker T, Gözen D. The effect of kangaroo care and breastfeeding on reducing the pain due to hepatitis B vaccine injection in newborn infants: a comparative analysis. J Pediatr Res 2022; 9(3):252-8. doi: 10.4274/jpr.galenos.2022.26539 [Crossref] [ Google Scholar]
- Saeidi R, Asnaashari Z, Amirnejad M, Esmaeili H, Gholami Robatsangi M. Use of “kangaroo care” to alleviate the intensity of vaccination pain in newborns. Iran J Pediatr 2011; 21(1):99-102. [ Google Scholar]
- Akbarian Rad Z, Aziznejadroshan P, Saebi Amiri A, Gholinia Ahangar H, Valizadehchari Z. The effect of inhaling mother’s breast milk odor on the behavioral responses to pain caused by hepatitis B vaccine in preterm infants: a randomized clinical trial. BMC Pediatr 2021; 21(1):61. doi: 10.1186/s12887-021-02519-0 [Crossref] [ Google Scholar]
- Savabi Esfahani M, Sheykhi S, Abdeyazdan Z, Jodakee M, Boroumandfar K. A comparative study on vaccination pain in the methods of massage therapy and mothers’ breast-feeding during injection of infants referring to Navabsafavi Health Care Center in Isfahan. Iran J Nurs Midwifery Res 2013; 18(6):494-8. [ Google Scholar]
- Karimi Z, Kazemi Karani N, Momeni E, Afrasiabifar A. The effect of breastfeeding versus sensorial saturation on infants’ behavioral responses of pain following pentavalent vaccination on 4 and 6-month old infants: a randomized controlled clinical trial study. Int J Community Based Nurs Midwifery 2022; 10(2):146-55. doi: 10.30476/ijcbnm.2021.87090.1400 [Crossref] [ Google Scholar]
- Modarres M, Jazayeri A, Rahnama P, Montazeri A. Breastfeeding and pain relief in full-term neonates during immunization injections: a clinical randomized trial. BMC Anesthesiol 2013; 13(1):22. doi: 10.1186/1471-2253-13-22 [Crossref] [ Google Scholar]
- Gupta NK, Upadhyay A, Agarwal A, Goswami G, Kumar J, Sreenivas V. Randomized controlled trial of topical EMLA and breastfeeding for reducing pain during wDPT vaccination. Eur J Pediatr 2013; 172(11):1527-33. doi: 10.1007/s00431-013-2076-6 [Crossref] [ Google Scholar]
- Pandita A, Panghal A, Gupta G, Verma A, Pillai A, Singh A. Is kangaroo mother care effective in alleviating vaccination associated pain in early infantile period? A RCT. Early Hum Dev 2018; 127:69-73. doi: 10.1016/j.earlhumdev.2018.10.001 [Crossref] [ Google Scholar]
- Gupta NK, Upadhyay A, Dwivedi AK, Agarwal A, Jaiswal V, Singh A. Randomized controlled trial of topical EMLA and vapocoolant spray for reducing pain during wDPT vaccination. World J Pediatr 2017; 13(3):236-41. doi: 10.1007/s12519-017-0004-y [Crossref] [ Google Scholar]
- Gajbhiye M, Rao SK, Singh HP. Comparative study between analgesic effect of breast feeding and oral sucrose in full term newborns. J Clin Diagn Res 2018; 12(12):9-12. doi: 10.7860/jcdr/2018/37721.12331 [Crossref] [ Google Scholar]
- Hatfield LA, Gusic ME, Dyer AM, Polomano RC. Analgesic properties of oral sucrose during routine immunizations at 2 and 4 months of age. Pediatrics 2008; 121(2):e327-34. doi: 10.1542/peds.2006-3719 [Crossref] [ Google Scholar]
- Kostandy R, Anderson GC, Good M. Skin-to-skin contact diminishes pain from hepatitis B vaccine injection in healthy full-term neonates. Neonatal Netw 2013; 32(4):274-80. doi: 10.1891/0730-0832.32.4.274 [Crossref] [ Google Scholar]
- Alzawad FH. Effect of breast-feeding vs oral sucrose on pain relief during vaccine intramuscular injection among infants. Am J Nurs Res 2019; 7(5):707-22. doi: 10.12691/ajnr-7-5-5 [Crossref] [ Google Scholar]
- Gad RF, Dowling DA, Abusaad FE, Bassiouny MR, Abd El Aziz MA. Oral sucrose versus breastfeeding in managing infants’ immunization-related pain: a randomized controlled trial. MCN Am J Matern Child Nurs 2019; 44(2):108-14. doi: 10.1097/nmc.0000000000000512 [Crossref] [ Google Scholar]
- Oh SH, Kim IA, Jin H. Optimal dextrose concentration for pain control in healthy newborns during hepatitis B vaccination. Neonatal Med 2018; 25(2):72-7. doi: 10.5385/nm.2018.25.2.72 [Crossref] [ Google Scholar]
- Hatami Bavarsad Z, Hemati K, Sayehmiri K, Asadollahi P, Abangah G, Azizi M. Effects of breast milk on pain severity during muscular injection of hepatitis B vaccine in neonates in a teaching hospital in Iran. Arch Pediatr 2018; 25(6):365-70. doi: 10.1016/j.arcped.2018.06.001 [Crossref] [ Google Scholar]
- Alzahrani S, Hasan AA. Transformational leadership style on nursing job satisfaction amongst nurses in hospital settings: findings from systematic review. Glob J Health Sci 2019; 11(6):25-52. doi: 10.5539/gjhs.v11n6p25 [Crossref] [ Google Scholar]
- Reynolds GD. Infant visual attention and object recognition. Behav Brain Res 2015; 285:34-43. doi: 10.1016/j.bbr.2015.01.015 [Crossref] [ Google Scholar]
- Iyer MS, Way DP, Schumacher DJ, Lo CB, Leslie LK. How general pediatricians learn procedures: implications for training and practice. Med Educ Online 2021; 26(1):1985935. doi: 10.1080/10872981.2021.1985935 [Crossref] [ Google Scholar]
- Raja SN, Carr DB, Cohen M, Finnerup NB, Flor H, Gibson S. The revised International Association for the Study of Pain definition of pain: concepts, challenges, and compromises. Pain 2020; 161(9):1976-82. doi: 10.1097/j.pain.0000000000001939 [Crossref] [ Google Scholar]
- Issac A, Dhiraaj S, Halemani K, Thimmappa L, Mishra P, Kumar B. Efficacy of early enteral nutrition on gastrointestinal surgery outcomes: a systematic review and meta-analysis. Eur J Pediatr Surg 2023; 33(6):454-62. doi: 10.1055/s-0043-1760837 [Crossref] [ Google Scholar]
- Harrison D, Reszel J, Bueno M, Sampson M, Shah VS, Taddio A. Breastfeeding for procedural pain in infants beyond the neonatal period. Cochrane Database Syst Rev 2016; 10(10):CD011248. doi: 10.1002/14651858.CD011248.pub2 [Crossref] [ Google Scholar]
- Gurung A, Bajracharya S. Effectiveness of breastfeeding for pain relief in infants during vaccination at Bharatpur. Int J Community Med Public Health 2022; 9(1):59-65. doi: 10.18203/2394-6040.ijcmph20214981 [Crossref] [ Google Scholar]
- Gai N, Naser B, Hanley J, Peliowski A, Hayes J, Aoyama K. A practical guide to acute pain management in children. J Anesth 2020; 34(3):421-33. doi: 10.1007/s00540-020-02767-x [Crossref] [ Google Scholar]
- Shetty AP, Halemani K, Issac A, Thimmappa L, Shashidhara YN, Mathias E. Effectiveness of the application of lanolin, Aloe vera, and peppermint on nipple pain and nipple trauma in lactating mothers: a systematic review and meta-analysis. Matern Child Health J 2024; 28(12):2013-25. doi: 10.1007/s10995-024-04006-1 [Crossref] [ Google Scholar]
- Holsti L, Grunau RE. Considerations for using sucrose to reduce procedural pain in preterm infants. Pediatrics 2010; 125(5):1042-7. doi: 10.1542/peds.2009-2445 [Crossref] [ Google Scholar]
- Bueno M, Ballantyne M, Campbell-Yeo M, Estabrooks CA, Gibbins S, Harrison D. The effectiveness of repeated sucrose for procedural pain in neonates in a longitudinal observational study. Front Pain Res (Lausanne) 2023; 4:1110502. doi: 10.3389/fpain.2023.1110502 [Crossref] [ Google Scholar]
- Campbell-Yeo ML, Disher TC, Benoit BL, Johnston CC. Understanding kangaroo care and its benefits to preterm infants. Pediatric Health Med Ther 2015; 6:15-32. doi: 10.2147/phmt.S51869 [Crossref] [ Google Scholar]
- Zhang Y, Deng Q, Zhu B, Li Q, Wang F, Wang H. Neonatal intensive care nurses’ knowledge and beliefs regarding kangaroo care in China: a national survey. BMJ Open 2018; 8(8):e021740. doi: 10.1136/bmjopen-2018-021740 [Crossref] [ Google Scholar]
- Koukou Z, Theodoridou A, Taousani E, Antonakou A, Panteris E, Papadopoulou SS. Effectiveness of non-pharmacological methods, such as breastfeeding, to mitigate pain in NICU infants. Children (Basel) 2022; 9(10):1568. doi: 10.3390/children9101568 [Crossref] [ Google Scholar]
- Sahebihag MH, Hosseinzadeh M, Mohammadpourasl A, Kosha A. The effect of breastfeeding, oral sucrose and combination of oral sucrose and breastfeeding in infant’s pain relief during vaccination. Iran J Nurs Midwifery Res 2011; 16(1):1-7. [ Google Scholar]
- Fillingim RB, Loeser JD, Baron R, Edwards RR. Assessment of chronic pain: domains, methods, and mechanisms. J Pain 2016; 17(9 Suppl):T10-20. doi: 10.1016/j.jpain.2015.08.010 [Crossref] [ Google Scholar]
- Hookway L, Lewis J, Brown A. The challenges of medically complex breastfed children and their families: a systematic review. Matern Child Nutr 2021; 17(4):e13182. doi: 10.1111/mcn.13182 [Crossref] [ Google Scholar]
- Berger SE, Baria AT. Assessing pain research: a narrative review of emerging pain methods, their technosocial implications, and opportunities for multidisciplinary approaches. Front Pain Res (Lausanne) 2022; 3:896276. doi: 10.3389/fpain.2022.896276 [Crossref] [ Google Scholar]
- Vitale E, De Angelis LR. Breastfeeding as an analgesic method during vaccinations. Minerva Ginecol 2020; 72(4):229-35. doi: 10.23736/s0026-4784.20.04569-4 [Crossref] [ Google Scholar]