Journal of caring sciences.15(1) :44-51.
doi: 10.34172/jcs.026.33500
Original Article
Designing and Determining Psychometric Properties of Meaning of Life Scale in Women with Breast Cancer: A Mixed Method Study
Leila Mokhtari Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Project administration, Validation, Visualization, Writing – original draft, Writing – review & editing, 1 
Abdollah Khorami Markani Conceptualization, Methodology, Resources, Supervision, Visualization, 1
Hamid Reza Khalkhali Formal analysis, Project administration, Validation, 2
Aram Feizi Funding acquisition, Methodology, Resources, Supervision, Validation, Visualization, Writing – review & editing, 2, *
Author information:
1Department of Nursing, Khoy University of medical Sciences, Khoy, Iran
2Patient Safety Research Center, Urmia University of Medical Sciences, Urmia, Iran
Abstract
Introduction:
Due to lack of specific tools for assessing meaning of life in women with breast cancer, this study was conducted to design and determine the psychometric properties of meaning of life scale in women with breast cancer.
Methods:
This sequential exploratory mixed method study was performed in hospitals affiliated to Urmia University of Medical Sciences in three stages: 1) the concept of meaning of life was explained (with 22 women); 2) Item pool was developed; 3) The psychometric properties of the tool was determined using content, face and construct validity (215 women). Sampling adequacy was confirmed by KMO=0.84. The extraction method used was principal component analysis (PCA), and an oblique rotation (oblimin) was applied. Internal consistency reliability and stability was determined.
Results:
First stage led to the formation of a theme entitled "evolution in the process of life" with 7 main categories. Then the primary tool was compiled, face and content validity by quantitative and qualitative method was determined. Construct validity (with 215 women) through exploratory factor analysis led to identifying four factors (better understanding of the value of life, striving for spiritual evolution, atempt to adaptation to disease, mental challenges due to disease) with 37 items in final scale. Cronbach’s alpha coefficient was calculated as 0.95 and intra-class correlation coefficient was calculated as 0.97.
Conclusion:
The findings of this study indicate that the newly developed meaning of life scale for Iranian women with breast cancer demonstrates acceptable content, face, and construct validity, along with good reliability. This culturally adapted and validated instrument can be used by researchers in future studies and psychosocial intervention programs targeting this population.
Keywords: Psychometrics, Meaning of life, Breast cancer, Instrumentation
Copyright and License Information
© 2025 The Author(s).
This work is published by Journal of Caring Sciences as an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/). Non-commercial uses of the work are permitted, provided the original work is properly cited.
Funding Statement
This research is part of PhDdissertation and did not receive any grant from funding agencies in the commercial or not-for-profit sectors. This project was supported by the research deputy of Urmia University of Medical Sciences. The funding body had no role in the design of the study, data collection, analysis, interpretation of data, or writing the manuscript.
Introduction
Breast cancer is the most common cancer in women and accounts for the highest number of cancer-related deaths in women.1 According to World Health Organization (WHO), in 2020, worldwide, 2,261,419 new cases of breast cancer occur in both sexes and at all ages, which is 11.7% of all cancers.2 In 2016, the incidence of this disease in Iranian women was 27.5 per 100,000 3 and one out of eight Iranian women will develop breast cancer during their lifetime.4 With the development of various diagnostic and therapeutic methods for breast cancer, life expectancy of women with this disease has increased.5 However, this disease changes the course of a person’s life and causes them many problems in all aspects of life,6 including quality of life, spiritual well-being and meaning of life (MoL).7 Striving for inner peace is one of the priorities of people with cancer, which is easily achieved through the ability to understand the true MoL and value it. MoL is one of the non-physical determining factors in shaping the quality of life among these patients.8
Viktor Frankl9has described meaning as the manifestation of values based on creativity, experience and attitude. Because cancer is life-threatening and the risk of death is high for these patients, the importance of MoL is highlighted.10 When people have a high sense of MoL, the search for meaning is a positive variable and has a positive relationship with life satisfaction and happiness.8 Moreover, the primary goal in caring for cancer patients, such as other chronic diseases, is to improve their quality of life. Finding meaning of life during the disease is one of the factors that greatly affect the quality of life.11
In the middle range theory of spiritual well-being in illness, factors related to finding MoL are mentioned, including social support, personal faith, severity of illness and stressful life events that ultimately lead to spiritual well-being.12 Zhong et al13 showed that the meaning of life has a moderating role in the relationship between perceived stress, mindfulness and psychological symptoms in the patients with gastric cancer. Considering the role of MoL, psychological symptoms can decrease in these patients. According to the study by Hooker et al14 people who have more MoL are better able to cope with life’s anxiety and challenges, and have a more positive outlook on the future. Thus, MoL is a useful coping skill that makes a person enjoy his/her good times and endure bad situations.
In recent decades, the important role of MoL in the patients with advanced diseases such as cancer has been emphasized10 and the MoL should be included in the evaluations and interventions of the patients with cancer.15 Our investigation indicates that there is currently no specific tool for assessing the MoL among patients suffering from breast cancer. Based on the Consensus-based Standards for the Selection of Measurement Instruments (COSMIN) checklist, the methodological quality of validation studies for existing meaning of life instruments was limited, particularly with regard to content validity and cultural relevance for Iranian women with breast cancer. Some of the available tools were designed when breast cancer was considered an incurable disease.16,17While today, breast cancer can be treated, which can be effective in understanding the MoL for these patients. One of tools have examined only one or two dimensions of the MoL.18 While the instrument designed in this study examines several dimensions of meaning in life in these women; in some of them, patients’ experiences have not been used and the tool has been designed through conceptualization16,19 and in this study, lived experiences of women with breast cancer were used for designing the items of scale. Considering these reasons, designing a tool that specifically and culturally assesses the meaning of life in women with breast cancer seems necessary. It was also necessary to explain the concept of meaning of life and its related components from the perspective of women with breast cancer in order to measure the meaning of life, in addition to measuring the necessary interventions to improve the meaning of life of these patients. Therefore, this study aims to design and determine the psychometric properties of a meaning of life scale in women with breast cancer.
Research Highlights
What is the current knowledge?
What is new here?
-
This study introduces the first culturally grounded, psychometrically validated Life Meaning Scale specifically for Iranian women with breast cancer, developed through in-depth qualitative interviews and fully validated across all psychometric dimensions (content, face, construct validity, reliability, and stability).
Materials and Methods
This study was conducted in 2021 at Urmia University of Medical Sciences as part of a larger sequential exploratory mixed-methods research project at Urmia University of Medical Sciences. Participants in this study were women with breast cancer. Inclusion criteria included willingness to participate in the study and complete the written consent form, being at least 20 years old and having passed at least 6 months from the time of diagnosis. Exclusion criteria also included the patient’s death, exacerbation of the disease in such a way that they were unable to cooperate and lack of knowledge about their disease. First, permission was obtained from Ethics Committee of Urmia University of Medical Sciences with the ethics approval NO.IR.UMSU.REC.1397.277. After explaining the objectives of the study, ensuring the anonymity and confidentiality of information and obtaining informed written consent by the participants, eligible women were selected and studied. In this study, a meaning of life instrument for women with breast cancer was developed and its psychometric properties were evaluated in three stages.
Step 1: Describing the Concept of Meaning of Life from the Perspective of Women with Breast Cancer
In this stage, in order to design the items of meaning of life scale in women with breast cancer, a qualitative contnet analysis study was performed.20 Qualitative content analysis seek to find and examine patterns of sense-making and meaning creation in the communicative characteristics of language, by focusing on the content and underlying themes and meaning that emerge in a text.21 This method contributes to deep exploration of experience and understanding of the data, leading to conclusions about the meaning of these experiences.22
Data collection began with purposive sampling using semi-structured interviews, and continued until data saturation. After 19 interviews, no new category was created, but to ensure data saturation, 3 more interviews were conducted and 22 interviews completed the study data. Interviews were conducted at the patients’ treatment unit, which lasted from 27 min to 76 min, with the average of 45 min. Interviews were carried out at the seven hospitals and oncology centers affiliated to Urmia University of Medical Sciences. Patients are referred to these centers after diagnosis of breast cancer for surgery, chemotherapy and radiotherapy.
When analyzing the content of the interviews, in order to ensure the observance of fidelity in the transmission of the participants’ speech, the sentences were typed verbatim after listening to it for several times, using Microsoft Word 2016. Qualitative data analysis was started by conventional qualitative content analysis method based on Granheim and Landmann’s23-25 series of articles using MAXQDA software (version 10). First, the meaning units were identified and, then, the meaning units were summarized and named with appropriate codes. The codes were placed into subclasses and classes based on the comparison of similarities and differences in them. Finally, the theme was extracted.
To ensure the rigor and trustworthiness of the data, 4 criteria proposed by Guba and Lincoln (1985) were used, which included Credibility, transferability, dependability, and confirmability.26 For this purpose, credibility was proved by prolonged engagement with data, peer check, review by participants, and observing maximum diversity in the selection of participants (In terms of some characteristics, such as age, marital status, educational level, place of residence, disease recurrence, and family socio-economic status). For transferability, clear explanation of the method of interviews and data analysis as well as accurate and in-depth description of the research steps were used. Dependability was proved by using external audit and explaining the details of study steps from the beginning to the end. An external auditor, a researcher with expertise in qualitative methodology but not directly involved in data collection or analysis, was engaged to review the coding process, thematic development, and interpretive rigor to enhance the trustworthiness of the findings. Continuous monitoring from the beginning to the end of the research were used for confirmability.27
Step 2: Developing Items Pool
In this stage, results obtained from the qualitative data of the first stage and reviewing extensive texts of authoritative scientific sources, which included articles and books related to the subject under study, as well as questionnaires and tools in the field of MoL, were used. A review of texts with the Persian and English keywords of MoL, breast cancer, spiritual well-being, MoL questionnaire, MoL inventory in Pubmed, Scopus, Sage, Google Scholar, Elsevier, ProQuest and Web of Sciense databases was performed from 1995 to 2020. A systematic literature review was conducted in accordance with the COSMIN checklist to evaluate instrument development/validation studies and the STROBE checklist to assess observational studies. Studies were eligible for inclusion if they were original quantitative and qualitative research articles or quantitative and qualitative review articles that considered the MoL and breast cancer as the main variables or concepts of the study, and full text of these studies are available. Initially, by removing duplicate articles and examining the titles of the articles, 114 relevant articles were identified. Subsequently, based on relevance and having the inclusion criteria, and considering the accessibility, 55 full-text articles were identified. After studying the content of these articles, 28 articles were included in the literature review. 18 quantitative articles used valid and reliable tools, and a total of 7 tools were identified. Of these tools, 5 tools related to examining the MoL in cancer patients were selected and reviewed. These five instruments include: SMiLE, LEQ, Purpose in Life Questionnaire, The meaning in life questionnaire, Meaning in life following cancer questionnaire. 2 tools were excluded due to insufficient evidence of content validity. Then, the basic items of MoL scale in women with breast cancer were developed. Items pool consisted of 106 items in 7 subcategories.
Step 3: Determining the Psychometric Properties of the Instrument
In this stage, in order to determine the psychometric properties of the instrument, its validity and reliability were determined. The validity of this scale measured and explained MoL in women with breast cancer.28 Reliability of this scale refers to consistency and stability in measuring structures of MoL.29
The qualitative content validity of the instrument was evaluated using the opinions of 13 experts in the field of MoL, oncology, instrument making, spiritual well-being and nursing. Their corrective comments were edited in terms of grammar, use of appropriate words, placement of items in their proper place and proper scoring of items and tools. Quantitative content validity was also determined using content validity ratio (CVR) and content validity index (CVI). To determine the CVR using the opinions of 13 experts, the cut-off point was considered 0.54 based on Lawshe table.30
Face validity was determined qualitatively by conducting interviews with 10 women with breast cancer. In each interview, participants explained whether selected measures’ items and responses were appropriate and acceptable, interpreted accurately and relevant to participants’ experiences. Also patients’ perspectives has been used to determine quantitative face validity by using item impact: items with a score higher than 1.5 were retained. Then, item analysis was performed.The CVI was determined based on the view of Waltz and Bausell31 that items with the CVI above 0.75 were retained and the CVI of all instruments and subscales as well as the Kappa agreement coefficient were calculated for each item.
Exploratory factor analysis (EFA) was used to determine the construct validity. One of the methods for determining the construct validity is factor analysis, the main purpose of which is to reduce the number of variables and, thus, better manage them.32 Exploratory factor analysis used Kaiser-Meyer-Olkin sampling index tests, Bartlett sphericity, principal component analysis, scree plot and direct oblimin rotation33 to classify the variables that were most related to each other. In factor analysis, in order to generalize from the sample to population, the ratio of 10 subjects per item is conventionally desirable and the ratios of at least 3 subjects per item are considered acceptable; the average of 5 subjects per item is considered.34 In this study, according to 51 items for exploratory factor analysis, 215 eligible women with breast cancer were selected by the convenience sampling from hospitals affiliated to universities of medical sciences in northwest of Iran and completed a questionnaire.
To determine the reliability of the instrument, two methods of internal consistency and stability reliability were used. In the internal consistency reliability, Cronbach’s alpha coefficient was considered acceptable above 0.70. The reliability of stability was also determined with the sample of 30 people with interval of 2 weeks using the intra-class correlation coefficient; the reliability coefficient higher than 0.70 was acceptable.29
Results
The mean (SD) age of the participants in the first phase of the study was 47.77(11.71) years old. The majority of them were married (86.40%), housewife (77.30%), graduated (40.90%) and had two children (54.50%). Results of qualitative data analysis led to extracting a main theme called “evolution in the process of life” and 7 main categories that included a “better understanding of the value of life”, “life expectancy”, “adaptation to disease”, “mental challenges due to disease”, “life satisfaction despite disease”, “support and cooperation of others in dealing with the disease” and “striving for spiritual evolution “.
In the second stage, the tool items were designed and developed, of which 93 items were extracted from qualitative study and 13 items from text review. The primary instrument with 106 items in 7 subscales was prepared based on the categories extracted in the qualitative study. These 7 subscales included “better understanding of the value of life” (13 items), “life expectancy” (15 items), “Atempt to adaptation to disease” (15 items), “mental challenges due to disease” (16 items), “life satisfaction despite disease” (16 items), “support and cooperation of others in dealing with the disease” (13 items) and “striving for spiritual evolution “ (18 items).
In the third step, the psychometric properties of the instrument were determined. In the qualitative content validity stage, the opinions of the experts applied and 15 items were revised. In the stage of determining the content validity ratio, 33 items with the CVR numerical value of less than 0.54 were removed and a tool with 73 items was prepared to check the content validity index. After determining the content validity index, 9 items had the score less than 0.70, which were removed. Finally, the tool with 64 items was prepared for face validity. The CVI of the scale and subscales with the method of calculating the means is presented in the Table 1.
In the qualitative face validity, 5 items were reviewed and approved by the participants. In the quantitative face validity, 5 items were removed due to the item impact of less than 1.5 and the instrument with 59 items was prepared to perform the item analysis. In this stage, 8 items were deleted due to the corrected item-total correlation coefficient lower than 0.30. The instrument was prepared with 51 items to perform the construct validity.
In order to evaluate the construct validity, the tool was completed by 215 women with breast cancer. Average age of women in this stage was 50.19 ± 9.65 years old. The majority of them were married (83.30%), housewives (90.20%), graduates (28.80%) and from middle class (55.80%). Results indicated that the sample was adequate for factor analysis. The Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy was 0.84, and Bartlett’s test of sphericity was statistically significant (χ2 = 5608.294, df = 1275, P< 0.001), confirming the suitability of the correlation matrix for factor analysis.
In order to extract the factors and to determine the number of factors in this study, method of principal component analysis, method of eigenvalue, explained variance and Scree plot (Figure 1) were used. Four factors were identified; 51 primary extracted items explained 66.28% of the variance before rotation. The first factor was 23.94%, the second factor was 10.48%, the third factor was 4.56% and the fourth factor was 3.84% of the total variance. Considering a factor load of less than 0.4 and a direct oblimin rotation, 12 items were excluded because they failed to reach the minimum factor loading threshold of 0.40 and exhibited theoretical inconsistency with the underlying constructs of the extracted factors. On the other hand, there was no cross loading that required re-exploratory factor analysis.
After construct validity, internal consistency reliability was performed, during which two items were removed. To determine the stability reliability, a test–retest was performed and the coefficient of intra-class correlation (ICC) between the scores obtained from two times of completing the instrument by 30 women with the interval of 2 weeks was calculated using the two-way mixed model and at 95% confidence. The ICC absolute agreement was calculated. Results for both internal consistency (Cronbach’s alpha) and stability (ICC) of the scale and its subscales are presented in Table 2.
Table 1.
The CVI of the scale and subscales
|
Subscales
|
CVI
|
| Better understanding of the value of life |
0.86 |
| Life expectancy |
0.84 |
| Atempt to adaptation to disease |
0.84 |
| Mental challenges due to disease |
0.87 |
| Life satisfaction despite disease |
0.80 |
| Support and cooperation of others in dealing with the disease |
0.91 |
| Striving for spiritual evolution |
0.88 |
|
Scale
|
0.86 |
Table 2.
Reliability coefficients (Cronbach’s alpha and ICC) for the scale and subscales
|
Subscales
|
Cronbach's alpha coefficients
|
ICC
|
95% confidence interval
|
sig
|
| Better understanding of the value of life |
0.89 |
0.94 |
0.91-0.97 |
P < 0.001 |
| Striving for spiritual evolution |
0.92 |
0.96 |
0.94-0.98 |
P < 0.001 |
| Atempt to adaptation to disease |
0.91 |
0.95 |
0.92-0.97 |
P < 0.001 |
| Mental challenges due to disease |
0.81 |
0.89 |
0.82-0.94 |
P < 0.001 |
|
Scale
|
0.95 |
0.97 |
0.95-0.98 |
P < 0.001 |
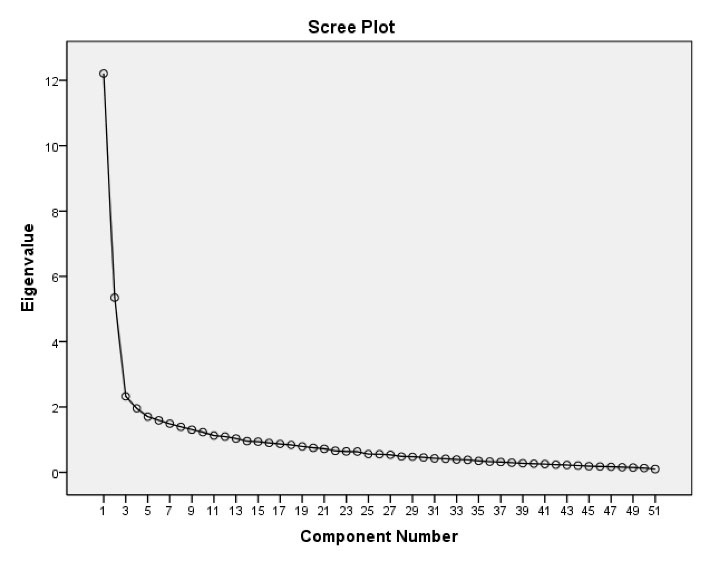
Figure 1.
Scree plot of meaning of life scale in women with breast cancer
.
Scree plot of meaning of life scale in women with breast cancer
Finally, the Meaning of Life (MoL) scale for women with breast cancer was finalized with four subscales and 37 items. The first subscale, “Better understanding of the value of life,” includes 9 items. The second subscale, “Striving for spiritual evolution,” consists of 13 items. The third subscale, “Attempt to adaptation to disease,” contains 11 items. The fourth subscale, “Mental challenges due to disease,” comprises 4 items.
Responses were recorded on a 5-point Likert scale ranging from always (5) to never (1). For the fourth subscale, scoring was reverse-coded due to the negatively worded items (i.e., never = 5, always = 1).
The total possible score on the scale ranges from 37 to 185. Subscale score ranges are as follows:
Better understanding of the value of life: 9–45
Striving for spiritual evolution: 13–65
Attempt to adaptation to disease: 11–55
Mental challenges due to disease: 4–20
Higher total scores indicate a higher level of perceived meaning in life.
In this study, the floor effect was 0.50% and the ceiling effect was 0.90% for the whole instrument, both below the recommended threshold of 15%.35 Additionally, 100% of the items were completed by all participants, indicating high feasibility of the instrument.
Discussion
This study developed and validated a culturally grounded Meaning of Life (MoL) scale for Iranian women with breast cancer, resulting in a 37-item instrument with four core dimensions: (1) better understanding of the value of life, (2) striving for spiritual evolution, (3) attempt to adaptation to disease, and (4) mental challenges due to disease. Notably, three categories identified in the qualitative phase—namely life expectancy, life satisfaction despite disease, and support from others—did not emerge as distinct factors in the final structure. This suggests that, within this population, these experiences may be deeply interwoven with spiritual and existential processes rather than operating as separate constructs. For instance, hope for the future (life expectancy) and gratitude amid suffering (life satisfaction) appeared to be expressions of a broader spiritual orientation, consistent with Islamic and Iranian cultural values that emphasize reliance on God (tawakkul), patience (sabr), and finding meaning through adversity.
The final structure of the MoL scale reflects a holistic understanding of meaning, making among Iranian women facing breast cancer. While widely used instruments such as the Meaning in Life Questionnaire (MLQ) distinguish between “presence of meaning” and “search for meaning”18, and the Purpose in Life (PIL) scale emphasizes goal-directedness and existential clarity36, our scale captures meaning as a dynamic, spiritually embedded process deeply rooted in Islamic and Iranian cultural contexts. Notably, the subscale “Striving for spiritual evolution” emerged as a central and robust dimension (CVI = 0.88; Cronbach’s α = 0.92), encompassing concepts such as trust in God (tawakkul), sincerity, and seeking divine closeness, elements rarely explicit in Western MoL measures. Similarly, “Mental challenges due to disease” uniquely acknowledges the emotional burden of cancer (e.g., fear of recurrence, body image concerns) not as a deficit, but as an integral part of the meaning-making journey. This integration of spiritual striving with existential struggle offers a culturally resonant framework that extends beyond individualistic or cognitive models of meaning, aligning instead with the collectivist and faith-centered worldview prevalent among Iranian women confronting life-threatening illness.
To evaluate the reliability, the internal consistency reliability was used by Cronbach’s alpha coefficient (0.95), which indicated the appropriate internal consistency of its items29. Calculating the Cronbach’s alpha coefficient is the best indicator for assessing reliability, which ranges from 0 to 1. The instrument has complete reliability when the score is equal to one and is, in fact, an estimate of the degree of correlation between the variables that make up the structure or instrument. Moreover, the reliability of stability was determined by retesting. Results obtained from two tests at two-week intervals showed high stability of the MoL scale in women with breast cancer (0.97)29. The concept of stability means achieving the same scores in a single group of people in two different time stages. The test is performed in a single group of subjects at two different times and obtains a correlation coefficient, which is called the stability coefficient. In all the related instrumentation studies, both types of reliability are examined and reported.18,28
One of the tools used to measure the MoL is the mening in life scale (MiLS), which was developed by Jim et al20 and has 20 items and four dimensions that include harmony and peace; life perspective, purpose and goals; confusion and lessened meaning; and benefits of spirituality which are related to each other. This scale is scored as a five-point Likert scale from 1 (strongly disagree) to 5 (strongly agree) and item 16 is inverse that is suitable for use in the patients with cancer. In this study, they examined and confirmed MoL scale in terms of content and construct validity (divergent, convergent and individual differences). Its internal stability was reported to be 0.93 using Cronbach’s alpha coefficient for the whole instrument and its retest reliability was reported to be 0.80 for the whole instrument using 43 samples of the first group with an interval of 2 weeks. However, this scale has been prepared through conceptualization and based on available texts; so, patients’ experiences in instrument design have not been taken into account. In designing quantitative tools, especially when a new structure is proposed, methods such as reviewing texts alone may not be sufficient; on the other hand, due to the limited knowledge of the researcher, it is better to do more studies to explain the concept. Given that the MoL is a multidimensional and abstract concept and varies from person to person, it is recommended to collect qualitative data to explain the concept and design tools for its measurement.37 Furthermore, this scale is not specific to measuring the MoL in women with breast cancer. However, the instrument designed in the present study is dedicated to measuring the MoL in women with breast cancer. Through a qualitative interview with women with breast cancer, a review of the designed texts and all psychometric steps of the instrument are reviewed and approved.
Limitations and Strengths
Since one of the characteristics of qualitative research is the non-generalizability of their results, in this study, because the participants were only related to a geographical area, the generalizability of the results is limited. However, in order to control it, appropriate sampling strategies were used, which included a combination of time, place and sampling with maximum variety and data collection methods. Due to the COVID-19 pandemic, the number of patients referring to medical centers had decreased significantly, which also prolonged the sampling process in the quantitative part of the study for performing EFA. The lack of a confirmatory factor analysis (CFA) due to time constraints was another limitation of this study that could have affected the results of the study.
One of the advantages of this study was conducting interviews with women with breast cancer and the use of their experiences in designing the scales’ items. Also, all the steps related to the determining psychometric properties of the scale in this study were carried out with extreme accuracy. The results of the analysis showed that 100% of the items were answered by the participants and there were no unanswered items, which shows the ease of use of the scale, which is another advantage of this study.
Conclusion
This study developed and validated a 37-item MoL scale for Iranian women with breast cancer, demonstrating strong psychometric properties. Grounded in participants lived experiences and culturally informed dimensions, particularly spiritual evolution and existential adaptation, the scale offer a contextually relevant tool for assessing meaning in this vulnerable population. While further validation in diverse samples is warranted, the instrument holds promise for use in clinical screening, spiritual care planning, and research on existential well-being in oncology settings. The results of this study, which originate from the lived experiences of women with breast cancer, can be useful and used by professional peers, nursing authorities, and managers in the health sector. Also, the findings of this study have applications in the fields of education, clinical practice, management, and research. Since the use of this scale can identify possible shortcomings, it is recommended to design and conduct quantitative studies using this tool. Furthermore, to increase the understanding of the meaning of life in these women, intervention studies should be designed, so that their results can be used to improve the understanding of the meaning of life and the quality of life of women with breast cancer.
Acknowledgments
The authors would like to express their deepest gratitude to the Department of Research of the Urmia University of Medical Sciences, all participants of the study, and estimable colleagues, especially in Omid and Imam Khomeini Hospital of Urmia and Shahid Madani Hospital of Khoy.
Competing Interests
All authors declare that they have no conflict of interests.
Data Accessibility
The datasets generated and analyzed during the current study are not publicly available due to ethical restrictions and confidentiality agreements with participants, as the data contain sensitive personal and health-related information. However, anonymized data may be made available from the corresponding author upon reasonable request and with prior approval from the Institutional Ethics Committee.
Ethical Approval
The study was approved by the Research Council and Ethics Committee of the Urmia University of Medical Science [IR.UMSU.REC.1397.277]. Signed informed consent obtained and all documents kept private and confidential.
References
- Obeagu EI, Obeagu GU. Breast cancer: A review of risk factors and diagnosis. Medicine (Baltimore) 2024; 103(3):e36905. doi: 10.1097/md.0000000000036905 [Crossref] [ Google Scholar]
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 2021; 71(3):209-49. doi: 10.3322/caac.21660 [Crossref] [ Google Scholar]
- Khoramdad M, Solaymani-Dodaran M, Kabir A, Ghahremanzadeh N, Hashemi EO, Fahimfar N. Breast cancer risk factors in Iranian women: a systematic review and meta-analysis of matched case-control studies. Eur J Med Res 2022; 27(1):311. doi: 10.1186/s40001-022-00952-0 [Crossref] [ Google Scholar]
- Ataeinia B, Saeedi Moghaddam S, Shabani M, Gohari K, Sheidaei A, Rezaei N. National and Subnational Incidence, Mortality, and Years of Life Lost Due to Breast Cancer in Iran: Trends and Age-Period-Cohort Analysis Since 1990. Front Oncol 2021; 11:561376. doi: 10.3389/fonc.2021.561376 [Crossref] [ Google Scholar]
- Global Burden of Disease Cancer C. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2017: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncology 2019; 5(12):1749-68. doi: 10.1001/jamaoncol.2019.2996 [Crossref] [ Google Scholar]
- Wang J, Wu SG. Breast Cancer: An Overview of Current Therapeutic Strategies, Challenge, and Perspectives. Breast Cancer (Dove Med Press) 2023; 15:721-30. doi: 10.2147/bctt.S432526 [Crossref] [ Google Scholar]
- Jadidi A, Ameri F. Social Support and Meaning of Life in Women with Breast Cancer. Ethiop J Health Sci 2022; 32(4):709-14. doi: 10.4314/ejhs.v32i4.6 [Crossref] [ Google Scholar]
- Bernard M, Strasser F, Gamondi C, Braunschweig G, Forster M, Kaspers-Elekes K. Relationship Between Spirituality, Meaning in Life, Psychological Distress, Wish for Hastened Death, and Their Influence on Quality of Life in Palliative Care Patients. J Pain Symptom Manage 2017; 54(4):514-22. doi: 10.1016/j.jpainsymman.2017.07.019 [Crossref] [ Google Scholar]
- Frankl VE. Man’s search for meaning: Beacon Press; 2017.
- Mokhtari M, Feizi A, Khorami Markani A, Mokhtari L. Relationship of Spiritual Well-being with Meaning of Life and Social Support in Women with Breast Cancer. Iran-J-of-Breast-Dis 2025; 17(4):136. doi: 10.61186/ijbd.17.4.136 [Crossref] [ Google Scholar]
- Sibeoni J, Picard C, Orri M, Labey M, Bousquet G, Verneuil L. Patients’ quality of life during active cancer treatment: a qualitative study. BMC Cancer 2018; 18(1):951. doi: 10.1186/s12885-018-4868-6 [Crossref] [ Google Scholar]
- Travelbee J. A Middle–range theory of spiritual wellbeing in illness. Jones & Bartlett Publisher, Sudbury; 2007.
- Zhong M, Zhang Q, Bao J, Xu W. Relationships Between Meaning in Life, Dispositional Mindfulness, Perceived Stress, and Psychological Symptoms Among Chinese Patients With Gastrointestinal Cancer. J Nerv Ment Dis 2019; 207(1):34-7. doi: 10.1097/nmd.0000000000000922 [Crossref] [ Google Scholar]
- Hooker SA, Masters KS, Park CL. A meaningful life is a healthy life: A conceptual model linking meaning and meaning salience to health. Rev Gen Psychol 2018; 22(1):11-24. doi: 10.1037/gpr0000115 [Crossref] [ Google Scholar]
- Kelada L, Zamir O. What Promotes Positive Parenting During Breast Cancer? A Cross-Sectional Analysis of Social Support, Emotion Regulation, and Meaning in Life. Int J Behav Med 2024; 31(4):595-604. doi: 10.1007/s12529-023-10196-9 [Crossref] [ Google Scholar]
- Fegg MJ, Kramer M, L’Hoste S, Borasio GD. The Schedule for Meaning in Life Evaluation (SMiLE): validation of a new instrument for meaning-in-life research. J Pain Symptom Manage 2008; 35(4):356-64. doi: 10.1016/j.jpainsymman.2007.05.007 [Crossref] [ Google Scholar]
- Salmon P, Manzi F, Valori RM. Measuring the meaning of life for patients with incurable cancer: the life evaluation questionnaire (LEQ). Eur J Cancer 1996; 32a(5):755-60. doi: 10.1016/0959-8049(95)00643-5 [Crossref] [ Google Scholar]
- Steger MF, Frazier P, Oishi S, Kaler M. The meaning in life questionnaire: Assessing the presence of and search for meaning in life. J Couns Psychol 2006; 53(1):80-93. doi: 10.1037/0022-0167.53.1.80 [Crossref] [ Google Scholar]
- Jim HS, Purnell JQ, Richardson SA, Golden-Kreutz D, Andersen BL. Measuring meaning in life following cancer. Qual Life Res 2006; 15(8):1355-71. doi: 10.1007/s11136-006-0028-6 [Crossref] [ Google Scholar]
- Mokhtari L, Markani AK, Khalkhali HR, Feizi A. The perceived social support by Iranian women with breast cancer: a qualitative study. Support Care Cancer 2022; 30(1):941-9. doi: 10.1007/s00520-021-06478-1 [Crossref] [ Google Scholar]
- Preiser R, García MM, Hill L, Klein L. Qualitative content analysis. The Routledge handbook of research methods for social-ecological systems: Routledge; 2021. p. 270-81.
- Corbin J, Strauss, A. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory. 4th ed. Thousand Oaks, CA: Sage Publications. 2015.
- Graneheim UH, Lindgren BM, Lundman B. Methodological challenges in qualitative content analysis: A discussion paper. Nurse Educ Today 2017; 56:29-34. doi: 10.1016/j.nedt.2017.06.002 [Crossref] [ Google Scholar]
- Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today 2004; 24(2):105-12. doi: 10.1016/j.nedt.2003.10.001 [Crossref] [ Google Scholar]
- Lindgren BM, Lundman B, Graneheim UH. Abstraction and interpretation during the qualitative content analysis process. Int J Nurs Stud 2020; 108:103632. doi: 10.1016/j.ijnurstu.2020.103632 [Crossref] [ Google Scholar]
- Lincoln Y, Guba E. But Is It Rigorous? Trustworthiness and Authenticity in Naturalistic Evaluation. New Directions for Program Evaluation 2004; 1986:73-84. doi: 10.1002/ev.1427 [Crossref] [ Google Scholar]
- Mokhtari L, Feizi A, Khalkhali HR, Khorami Markani A. Lived Experience of Women Suffering from Breast Cancer about Meaning of Life: Evidences from Society of Iranian Women. Health Educ Health Promot 2022; 10(1):43-50. [ Google Scholar]
- Polit DF, Beck CT. Essentials of nursing research: Appraising evidence for nursing practice: Lippincott Williams & Wilkins; 2010.
- Polit DF, Yang F. Measurement and the measurement of change: a primer for the health professions: Wolters Kluwer Philadelphia, PA; 2016.
- Lawshe CH. A quantitative approach to content validity. Pers Psychol 1975; 28(4):563-75. [ Google Scholar]
- Waltz CF, Strickland OL, Lenz ER. Measurement in nursing and health research: Springer publishing company; 2010.
- Streiner D, Norman GR, Cairney J. Health measurement scales: a practical guide to their development and use. Aust NZJ Public Health. 2024.
- Watkins MW. Exploratory Factor Analysis: A Guide to Best Practice. Journal of Black Psychology 2018; 44(3):219-46. doi: 10.1177/0095798418771807 [Crossref] [ Google Scholar]
- Munro BH. Statistical methods for health care research: lippincott williams & wilkins; 2005.
- Mokkink LB, Terwee CB, Patrick DL, Alonso J, Stratford PW, Knol DL, et al. COSMIN checklist manual. Amsterdam: University Medical Center. 2012.
- Crumbaugh JC, Maholick LT. An experimental study in existentialism: the psychometric approach to frankl’s concept of noogenic neurosis. J Clin Psychol 1964; 20:200-7. doi: 10.1002/1097-4679(196404)20:2<200::aid-jclp2270200203>3.0.co;2-u [Crossref] [ Google Scholar]
- DeVellis RF, Thorpe CT. Scale development: Theory and applications. Sage publications; 2021.