Journal of caring sciences. 14(4):293-302.
doi: 10.34172/jcs.025.33570
Systematic Review
The Effect of Evening Primrose Oil on Menopausal Symptoms Management: A Systematic Review and Meta-Analysis
Mona Larki Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Validation, Writing – original draft, Writing – review & editing, 1, 2 
Solmaz Mohammadi Data curation, Investigation, Methodology, Validation, Visualization, Writing – original draft, Writing – review & editing, 3
Somayeh Makvandi Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing, 4, *
Author information:
1Nursing and Midwifery Care Research Center, Mashhad University of Medical Sciences, Mashhad, Iran
2Department of Midwifery, School of Nursing and Midwifery, Mashhad University of Medical Sciences, Mashhad, Iran
3Department of Midwifery, Reproductive Health Promotion Research Center, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
4Department of Midwifery, Menopause Andropause Research Center, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
Abstract
Introduction:
Many women avoid hormone therapy due to the health risks, deciding to pursue herbal alternatives. This meta-analysis aimed to determine the effectiveness of evening primrose oil (EPO) in managing menopausal symptoms.
Methods:
A comprehensive literature review was conducted until February 7,2024, without any limitations on language or time, using electronic databases such as PubMed, Web of Science, Scopus, and the Cochrane Library to collect randomized clinical trials. The methodological quality of the included trials was assessed using the Cochrane Risk of Bias 2 (ROB2) tool. The GRADEpro evaluated the quality of the evidence, and the RevMan 5.4 performed the data analysis.
Results:
Six randomized controlled trials (RCTs) were included in this study. The meta-analysis of 450 women revealed, however, that the women in the EPO group experienced a mean decrease of 2.13 in the number of hot flashes per day compared to the control group. Still, it was not statistically significant. Women who received EPO also experienced a significant reduction in the duration of hot flashes compared to those who did not supplement. The EPO group experienced a 0.19 reduction in hot flash intensity, but this reduction was not statistically significant. The evidence grading was moderate to low.
Conclusion:
EPO reduces menopausal symptoms, but to understand the effectiveness of this option, we need to conduct further research with rigorous methodological standards so that menopausal women can make decisions that improve their quality of life in the menopause period.
Keywords: Menopause, Evening primrose oil, Complementary therapies, Women’s health services
Copyright and License Information
© 2025 The Author(s).
This work is published by Journal of Caring Sciences as an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/). Non-commercial uses of the work are permitted, provided the original work is properly cited.
Funding Statement
This article was funded by Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran.
Introduction
Menopause is an important physiological phenomenon in women’s lives.1 It is a natural process that typically occurs between 45 and 52, characterized by hormonal changes and the cessation of the menstrual period.2 Projections indicate that by 2030, the population of postmenopausal women will reach 1.2 billion, with an annual increase of 47 million new cases.3 Vasomotor symptoms, psychological symptoms, musculoskeletal pain, osteoporosis, sleep problems, and genitourinary symptoms are among the problematic symptoms encountered by these women.4,5 The main symptoms of menopause are vasomotor symptoms (like hot flashes and night sweats). More than 80% of women seek treatment for these symptoms,6 which can persist for 5 to 7 years or even longer.1 These symptoms are associated with sleep disturbances, mood changes, decreased cognitive function, and reduced quality of life.2,7 Vaginal dryness and dyspareunia (painful intercourse) affect approximately one-third of postmenopausal women. These issues can persist over an extended period.8 Around one-third of women experience poor sleep during the menopausal transition.9
Hormone therapy (HT) can effectively treat menstrual symptoms.10 However, many women rarely use HT due to its associated health risks.11 More than 60% of women believe that complementary and alternative medicines (CAM) can effectively alleviate menopause symptoms, with approximately 51% using these alternative approaches.12 Among the herbal remedies utilized in CAM therapies are Cimicifuga racemosa, licorice, valerian, soy, sage, ginseng, black cohosh, and evening primrose oil (EPO).3,13-15 Evening primrose belongs to the family Onagraceae.16 It is a rich source of essential fatty acids, including gamma-linolenic acid and phytosterols.17,18 Some studies suggest that EPO is effective in relieving the symptoms of menopausal vasomotor issues,18,19 but evidence for its use is inadequate. It seems that the need for an updated and comprehensive review is underscored by the rapid advancements in the field of menopausal symptom management. The sole meta-analysis conducted in this field pertains to the study of Christelle et al20 with a search extending up to 2019. A fundamental flaw identified in their Forest plot is the inappropriate amalgamation of heterogeneous studies. The plot conflated randomized controlled trials (RCTs) with placebo control groups with those employing black cohosh as the control, comparing them against EPO as an intervention (as seen in the RCT by Mehrpooya et al21). It also merged studies where the intervention was not solely EPO but included Lady’s capsule—a blend of several herbs with EPO being just one component with placebo-controlled trials (as in the study by Yakoot et al22). This conflation of disparate studies leads to a compromised synthesis of data. Therefore, in the current research, we have endeavored to rectify this error by excluding such conflated comparisons and incorporating more recent studies postdating the previous meta-analysis. By doing so, we provide a current and thorough understanding of the effect of EPO on alleviating menopausal symptoms. This endeavor not only reflects the ongoing scientific discourse but also addresses the practical implications for clinical practice. This study aimed to evaluate the impact of EPO on the management of menopausal symptoms, offering insights that could significantly improve the quality of life for postmenopausal women.
Materials and Methods
This research project has received approval from the Research Ethics Committee of Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran (Ref. No: IR.AJUMS.REC.1402.643). This approval ensures that the study adheres to the highest ethical standards. Additionally, the research plan has been recognized for its merit and potential by Ahvaz Jundishapur University of Medical Sciences’ Grant Committee.
This systematic review and meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to ensure transparency and rigor in the reporting of the study.23
A comprehensive search strategy was developed to identify relevant studies. The following databases were searched from inception to 7 February 2024: PubMed, Web of Science, Cochrane Library, and Scopus. Additionally, due to the majority of our final studies being derived from trials conducted in Iran, the following Iranian databases were also searched: IranMedex, SID, and Magiran Furthermore, we explored the Iranian Registry of Clinical Trials (IRCT) to identify additional articles. This comprehensive search strategy was employed to ensure a thorough inclusion of relevant literature. The search terms included variations of “evening primrose oil,” “menopausal symptoms,” and related keywords (Supplementary file 1).
Two independent reviewers screened the titles and abstracts of the retrieved articles to identify potentially relevant studies. Full texts of selected articles were then assessed for eligibility based on predetermined inclusion and exclusion criteria.
Clarifying the Study’s Objective: A PICO Framework Approach
To ensure a structured and focused approach to our systematic review and meta-analysis, we employed the PICO framework. This methodology allows for a clear delineation of the research question, guiding the inclusion and exclusion criteria for relevant studies:
Participants: The review included peri- and postmenopausal women experiencing menopausal symptoms who are participants in the included studies.
Interventions: The primary intervention of interest was the administration of EPO.
Comparators: The comparators were placebo or no treatment conditions, as reported by the included RCTs.
Outcomes: The outcomes of interest included the severity and frequency of menopausal symptoms such as hot flashes, night sweats, psychological symptoms, specific activities, and hormonal levels.
Data extraction was performed independently by two reviewers using a standardized data extraction form. The following information was extracted from each study: study characteristics (author, year of publication), participant characteristics, intervention details, control or comparison, outcomes assessed, tools, and findings.
The methodological quality of the included studies was assessed using an appropriate tool of Cochrane Risk of Bias 2 (RoB2) tool.24 It is a standardized method for assessing the risk of bias in RCTs included in systematic reviews and meta-analyses. The RoB2 tool assesses bias across five key domains: bias arising from the randomization process, bias due to deviations from intended interventions, bias due to missing outcome data, bias in the measurement of the outcome, and bias in the selection of the reported result. For each domain, the RoB2 tool provides specific signaling questions that guide reviewers in assessing the risk of bias. These questions help reviewers evaluate the adequacy of randomization, blinding, handling of missing data, and other factors that could affect the validity of study results. Based on assessments within each domain, an overall risk of bias judgment was made for each included study. Studies could be rated as high risk, with some concerns, or low risk based on the assessment.
The difference in means (MD) of quantitative data was computed. This effect size helps quantify the magnitude of change between groups or conditions. When the same outcome was assessed in various ways in articles included in the meta-analysis, standardized mean difference (SMD) was applied. Forest plots were utilized to graphically display the estimated data for the effect size. These plots help visualize the results from individual studies and their overall impact on the meta-analysis. A P value of 0.05 was determined to be statistically significant. This threshold indicates whether the observed effect size is likely due to chance or represents a true difference. The I2 statistic was employed to evaluate heterogeneity, indicating the proportion of total variance attributable to it. However, the selection between fixed-effects and random-effects models was not predicated on I2 values alone. While I2 values below 50% may suggest moderate heterogeneity and values above 50% indicate substantial heterogeneity, the choice of model was informed by the characteristics of the studies and the nature of the meta-analysis.25,26 The fixed-effects model was considered when studies were homogenous in terms of participants, interventions, outcomes, and methodologies. In contrast, the random-effects model was applied under the assumption of varying true effect sizes across studies.27 Publication bias was not evaluated due to the small number of included studies (less than 10 studies). The RevMan 5.4 software (Cochrane Collaboration, Oxford) was used for all analyses. Findings that could not be meta-analyzed were reported qualitatively.
To determine the quality of evidence for outcomes, we employed the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) tool. This tool categorizes systematic reviews or meta-analyses into four groups: ‘high,’ ‘moderate,’ ‘low,’ and ‘very low.’ We started with a ‘high’ grade and downgraded it if we found bias, inconsistency (I2 statistics > 50%), indirectness (intervention differences), imprecision (95% CI includes 1.0), or publication bias. Conversely, if there was a significant intervention effect or if all reasonable biases would reduce the amount of the intervention’s effect in the event of a dose-response association, the rating was raised.28 Two researchers independently performed the GRADE assessment and resolved any discrepancies through discussion.
Our meta-analysis was carried out in strict compliance with research ethics. Since we relied on previously published studies, no direct involvement of human or animal participants was required in our study. Nonetheless, we verified that each study included had received the necessary ethical clearance from their respective ethics committees or institutional review boards.
Results
Characteristics of the Included Studies
In the initial search of the databases, 282 articles were entered into the EndNote 20 software. After the data abstraction process, 65 full-text articles were carefully reviewed. Finally, 6 RCTs18,29-33were included in the systematic review and 4 of them were incorporated into the meta-analysis.18,31-33 (Figure 1).
Five studies were published in English18,29-32and one in Farsi.33 The RCTs were published between 199431 and 2023.30 The sample size varied from 5631 to 18929 participants per study. One trial was conducted in the UK31 and five trials in Iran.18,29,30,32,33 In all studies, EPO was used in comparison with Placebo. All the studies had two arms, except the study by Ghavi et al30 which had three arms, and EPO and fennel were compared with placebo. Other information is given in Table 1.
Risk of Bias Assessment
The risk of biased judgment for included studies and the bias graph across all trials are presented in Table 2 and Figure 2. The overall risk of bias was low for three RCTs,29,32,33 with some concerns for two RCTs,18,30, and high for one RCT.31 All trials were assessed as having a low risk of bias in two domains: deviations from intended interventions and measurement of the outcome. The domain with the most bias was the selection of the reported result, with two studies being judged to have some concerns.
The Findings of the Meta-analysis
Frequency of Hot Flashes
Figure 3 shows the forest plot of EPO effect on the frequency of hot flashes. The meta-analysis of 450 women revealed that however the women in the EPO group experienced a mean decrease of2.13 in the number of hot flashes per day compared to the control group, but it was not statistically significant (MD = -2.13, 95% CI -4.26 to 0.001, P = 0.05). Due to the significant heterogeneity, the random effect model was used (Chi2 = 25.79, I2 = 84%, P < 0.0001), and the publication bias was not evaluated due to the small number of RCTs.
Duration of Hot Flashes
The impact of EPO on the duration of hot flashes in menopausal women is depicted in Figure 4. Women who supplemented with EPO saw a notable decrease in the duration of hot flashes compared to those who did not supplement (SMD = -0.39, 95% CI -0.76 to -0.02, P = 0.04). A random effects model was employed due to substantial heterogeneity detected across the studies (Chi2 = 9.71, I2 = 69%, P = 0.02). Publication bias was not assessed due to the limited number of studies available.
The Intensity of Hot Flashes
Figure 5 displays the forest plot illustrating the impact of EPO on the intensity of hot flashes. According to a fixed-effect model, the intensity of hot flashes was reduced by 0.19 in the EPO group, but this reduction was not statistically significant (SMD = -0.19, 95% CI -0.45 to 0.08, P = 0.16). No substantial heterogeneity was observed (Chi2 = 0.82, I2 = 0%, P = 0.37).
Other Effects of EPO on Menopausal Symptoms
The Effect of EPO on Menopause Rating Scale (MRS) Score
In a clinical trial conducted by Ghavi et al30 involving 125 menopausal women, it was observed that the average MRS score significantly decreased in the fennel and EPO groups compared to the placebo group. However, this difference was only statistically significant in the psychological aspect, with no significant changes in the physical and urogenital dimensions post-intervention. The disparity in the mean MRS score between the fennel and EPO groups post-intervention was not statistically significant. Another study by Sharif et al29 focused on assessing the impact of EPO on psychological symptoms of menopause, specifically depressive moods, irritability, anxiety, and mental and physical exhaustion. The results indicated a notable improvement in the intervention group’s outcome measures in terms of within-group changes in mean values. Furthermore, the intervention group experienced a significant reduction in symptoms compared to the control group in terms of mean differences in psychological scores.
The Effect of Hot Flashes after Receiving EPO on Specific Activities
Farzaneh et al’s study18 demonstrated significant differences in certain subscales of the Hot Flash Related Daily Interference Scale (HFRDIS) between the intervention and control groups. Over the 6 weeks, all subscales showed improvement in both groups. Notably, the EPO group exhibited greater enhancements in three subscales: social activity, relations with others, and sexuality.
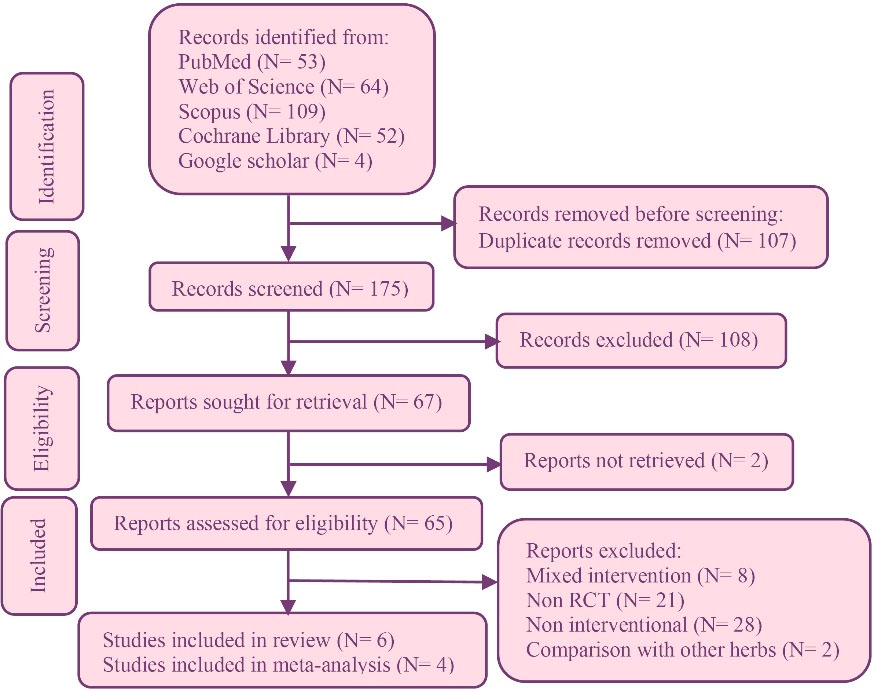
Figure 1.
PRISMA 2020 flow diagram for systematic reviews
.
PRISMA 2020 flow diagram for systematic reviews
Table 1.
Characteristics of the included studies
|
Author, year
|
Country
|
Randomization /concealment
|
Blinding
|
Participants
|
Control
|
Intervention
|
Outcome(s)
|
Tool(s)
|
Finding(s)
|
Chenoy et al31
1994 |
United Kingdom |
NI/NI |
Double-blinded |
Menopausal women who had hot flushes at least three a day and who had raised gonadotrophin concentrations or had had amenorrhea for at least 6 months, or both. |
N = 28
Placebo |
N = 28
Gelatin capsule contained 500 mg EPO with 10 mg natural vitamin E (Scotia 05027) twice a day for 6 month–s |
Change in the number of hot flashes or sweating episodes in a month. |
Diary cards |
EPO had no benefit over placebo in the alleviation of vasomotor symptoms |
Farzaneh et al18
2013 |
Iran |
computer-generated randomization/ drugs were packed in similar boxes marked with
patient number |
Double-blinded |
The eligible subjects were natural postmenopausal women, over 40 years of age, with no menstrual period in 12 months before enrollment, who had a self-reported history of hot flashes (more than four times per day) with no previous therapy for it. |
N = 28
Placebo |
N = 28
Soft gelatin capsules containing 500 mg EPO extracted from seeds of the plant Oenothera biennis (Nutri Primrose, Nutri Century, Toronto, Canada), two capsules per day for the following 6 weeks |
Frequency, duration, and severity of hot flashes occurring over 24 hours
Impact of hot flashes on specific activities |
Numeric rating scale
HFRDIS |
All 3 characteristics of hot flash were ameliorated in the EPO arm, only its severity was significantly better in this arm compared with the placebo group.
Improvement in social activities, relations with others, and sexuality was significantly superior in the EPO group to the placebo group |
Ghavi et al30
2023 |
Iran |
table of random numbers/ boxes of identical
shape and format |
Triple-
blinded |
Menopausal women of 45-60 years of age, who were married, their menses had ceased for at least 1 year, had no specific disease, did not take any medication, had no sensitivity to honey, had no addiction, were not using sedation techniques |
N = 40
Placebo |
N = 42
1000 mg soft capsules containing 70-140 mg of gamolenic acid obtained from evening primrose seeds with concentrations of 7-14% (Barij Essence Pharmaceutical Company, Kashan, Iran), 2 capsules daily for 8 weeks. |
Results of hormonal
assessment
Menopause -specific health-related
quality of life |
Lab tests
MRS |
Both fennel and EPO can significantly change FSH, estradiol, and psychological menopausal symptoms in postmenopausal women. |
N = 43
Pearl-shaped pills of fennel (30 mg) |
Kazemi et al32
2021 |
Iran |
NI/ opaque closed packages |
Single-Blind |
At least a year after the last menstrual cessation, no acute and chronic illnesses, no herbal medication since three months before the intervention, no previous allergy to medicinal herbs, affliction from or a history of breast cancer and genital cancer |
N = 83
Placebo |
N = 80
1000 mg EPO, which was produced by Barij Essence Pharmaceutical Company (Mashhad Ardehal, Iran), was used twice a day for 8 weeks |
Duration, severity, and frequency of hot flashes during 24 hours per week
The intensity of night sweat |
Wiklund Vasomotor Symptom
subscale score was used to measure hot flashes and night sweats |
The mean score of duration, frequency, and severity of hot flashes did not significantly decrease in both groups after the intervention.
The EPO group had lower frequency and severity of night sweats after the intervention than the control group. |
Motaghi Dastenaei et al33
2017 |
Iran |
NI/ opaque closed packages |
Triple-blinded |
Healthy menopausal women, without the use of hormonal drugs and underlying diseases, normal pap smear results in the past year, complaining of menopausal symptoms and having minimal reading and writing literacy. |
N = 46
Placebo |
N = 44
EPO pearl, 1 g, twice a day for one month |
Duration, severity, and frequency of hot flashes during 24 hours |
Kupperman Index |
Significant reduction in the duration, severity, and frequency of hot flushes in the EPO group compared to the control group |
Sharif and Darsareh29
2020 |
Iran |
NI/ similar capsules in size, shape, and color in coded packages |
Double-blinded |
Menopausal women with amenorrhea for at least 1 year; normal pap smear test results in the last year; no history of malignancies or chronic medical conditions; no history of drug addiction; and no history of mental disorders. |
N = 95
Placebo |
N = 94
1000 mg of EPO capsules (Nature Life Co, Coquitlam, BC, Canada) daily after the baseline visit until the follow-up for 8 weeks |
Changes in
psychological symptoms of menopause |
MRS |
The psychological symptoms were significantly alleviated in the EPO group compared with the control group. |
NI: No information, EPO: Evening primrose oil, HFRDIS: Hot Flash Related Daily Interference Scale, MRS: Menopause Rating Scale.
Table 2.
Risk of bias judgment for included studies
|
Author, year
|
D1
|
D2
|
D3
|
D4
|
D5
|
Overall
|
| Chenoy et al311994 |
Some concerns |
Low |
Low |
Low |
Some concerns |
High |
| Farzaneh et al18 2013 |
Low |
Low |
Some concerns |
Low |
Low |
Some concerns |
| Ghavi et al30 2023 |
Low |
Low |
Low |
Low |
Some concerns |
Some concerns |
| Kazemi et al32 2021 |
Low |
Low |
low |
Low |
Low |
Low |
| Motaghi Dastenaei et al33 2017 |
Low |
Low |
Low |
Low |
Low |
Low |
| Sharif and Darsareh29 2020 |
Low |
Low |
Low |
Low |
Low |
Low |
D1: Bias arising from the randomization process; D2: Bias due to deviations from intended interventions; D3: Bias due to missing outcome data; D4: Bias in the measurement of the outcome; D5: Bias in the selection of the reported result.
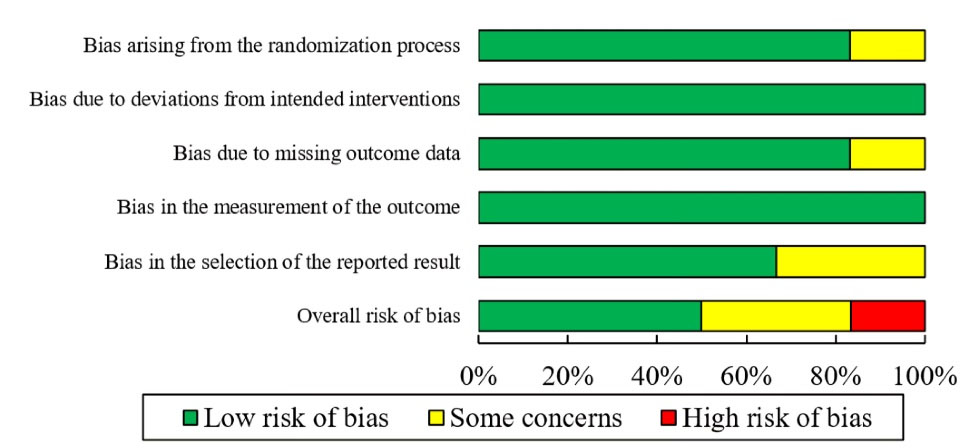
Figure 2.
Risk of bias graph across all included studies
.
Risk of bias graph across all included studies
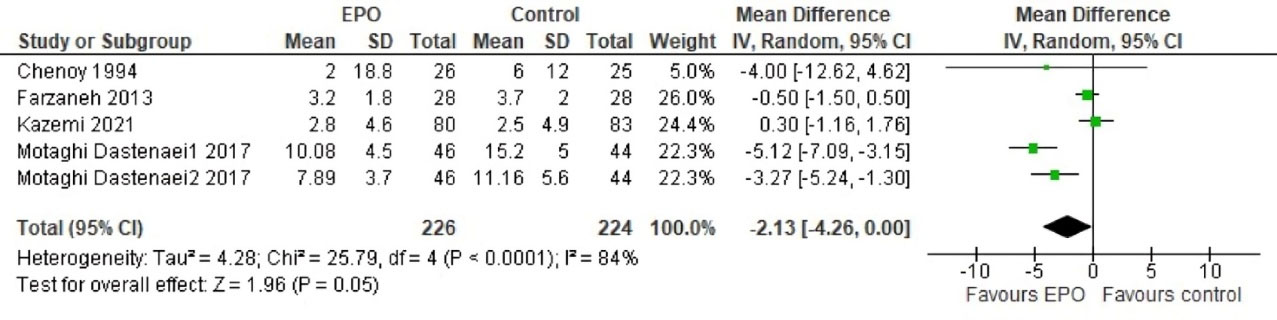
Figure 3.
Forest plot of EPO effect on the frequency of hot flashes
.
Forest plot of EPO effect on the frequency of hot flashes
The Effect of EPO on Hormonal Levels
In a three-arm trial30 comparing EPO and fennel to a placebo, hormonal changes were assessed. The results indicated significant alterations in mean levels of follicle-stimulating hormone (FSH) and estradiol in the fennel and EPO groups compared to the placebo group. Specifically, FSH levels decreased, and estradiol levels increased significantly in the intervention groups compared to the placebo group. However, there was no significant difference in the mean FSH score between the fennel and EPO groups.
The Effect of EPO on Night Sweats
A study32 evaluating the effects of EPO on night sweats revealed that the intervention group experienced a reduction in both the frequency and severity of night sweats post-intervention compared to the control group. These differences were statistically significant.
Grading of the Evidence
The evidence grading for the frequency of hot flashes was deemed moderate, following a single downgrade owing to inconsistency across studies. In a similar vein, the evidence grading for the intensity of hot flashes was also categorized as moderate, with one downgrade due to imprecision in the reported outcomes. As for the duration of hot flashes, the evidence was rated as low; this was the result of two downgrades, one for inconsistency and another for imprecision in the data (Table 3).
Discussion
This study aimed to determine the effect of EPO on menopausal symptoms. The current systematic review includes six studies. Analysis of the four studies included showed that EPO use in women with menopause, compared with placebo, resulted in a significant reduction in the duration of hot flashes. But it did not make significant differences in the intensity or frequency of hot flashes compared to placebo. Women in the EPO group experienced a mean decrease of 2.13 in the number of hot flashes per day compared to the control group. The intensity of hot flashes also decreased by 0.19 in the EPO group compared to the control group.
EPO is rich in omega-6 essential fatty acids, particularly linoleic acid and gamma-linolenic acid, which have antioxidant and anti-inflammatory properties.34,35 The impact of omega-3 on immune cells directly as well as indirectly on the formation of eicosanoid molecules, such as prostaglandins, cytokines, and cytokine mediators.36 Implementing a comprehensive approach to menopausal management that includes a combination of lifestyle, hormonal, and non-hormonal therapies is critical for improving afflicted women’s quality of life. However, many individuals choose non-hormonal treatments or face risks associated with HT.37
Christelle et al20 conducted a study exploring the effectiveness of EPO as a treatment for menopausal symptoms in perimenopausal and postmenopausal women. The analysis of five RCTs involving 402 postmenopausal and perimenopausal women revealed that EPO may reduce the overall severity of menopausal symptoms but does not significantly decrease both the severity and frequency of vasomotor complaints. A limitation of Christelle et al’s study was the lack of uniform interventions across the experimental and control groups in the analyzed studies, hindering direct comparisons. For instance, the control group in the Mehrpooya et al21study received 40 mg of black cohosh, while the intervention in Yakoot et al22 study included EPO + damiana + Panax ginseng + royal jelly. In contrast, remining studies solely utilized EPO as the intervention.
Numerous systematic reviews have investigated CAM for menopausal symptoms has been the subject of numerous systematic reviews. However, these reviews only included one RCT that utilized EPO38-40and another review that included two.41
A result of two studies investigating the effect of EPO on the psychological symptoms of menopausal women found significant improvements in the psychological symptoms after treatment compared to placebo.29,30 There was not sufficient data to conduct a meta-analysis on this variable; therefore, additional trials are necessary to provide accurate conclusions regarding the utilization of EPO in healthcare settings.
A study has reported on the impact of EPO on hormone levels. In this study, findings showed that FSH levels decreased and estradiol levels increased significantly in the intervention groups compared to the placebo group. However, there was no significant difference in the mean FSH score between the fennel and EPO groups.30
A 2020 meta-analysis of six RCTs demonstrated that oral EPO at doses of ≤ 4 g/day substantially reduces blood triglyceride levels and increases high-density lipoprotein (HDL) levels in hyperlipidemic individuals.42 In a review by Faghani Aghoozi et al19 summarizing research on the effects of EPO on obstetric conditions such as polycystic ovarian syndrome (PCOS), postpartum blues, menopausal disorders, mastalgia, and prolonged pregnancy, it was concluded that EPO has benefits in improving premenstrual syndrome, postpartum depression, hormonal issues in PCOS, the lipid profile of gestational diabetes, and menopausal hormone replacement therapy. Considering the insights from the meta-analysis, there is a call for well-designed trials with robust methodologies to further explore the effects of oral EPO on menopausal symptoms.
There was a mixed level of bias in the evaluation of the studies that were included. Also, for outcomes such as frequency, duration, and intensity of hot flashes, the GRADE assessment found that the evidence quality was moderate to low. These gradings reflect the need for more rigorous and consistent research methodologies in future studies. The moderate grading indicates that while the results are likely to be reliable, there may be some variability that could affect the confidence in the effect estimates. The low grading for the duration of hot flashes suggests that the current evidence is limited and further research is necessary to draw more definitive conclusions. Subsequent studies must address these methodological concerns to enhance the quality and clarity of evidence in this domain.
Our review benefits from a comprehensive and systematic literature search, ensuring the identification of relevant publications. Also, to minimize bias, we implemented multiple steps, including involving two authors in various processes (search, identification, screening, inclusion, data extraction), GRADE evaluations, and risk assessments. Additionally, the assignment of a third review author to address challenges and reevaluate adds rigor to the process.
All included studies were conducted in Iran, except for one in the UK. As a result, generalizing findings to the global population may be unrealistic due to geographical and ethnic variations. The limited number of samples and reliance on self-reported questionnaires in most studies pose limitations. Short-term outcomes were the primary focus, and data on the long-term consequences of EPO are lacking. Substantial heterogeneity among the publications in this meta-analysis warrants caution when interpreting findings. Furthermore, the limited number of included articles restricted a comprehensive analysis of relevant variables and future trials should compare EPO across menopausal causes, stages, and ethnicities.
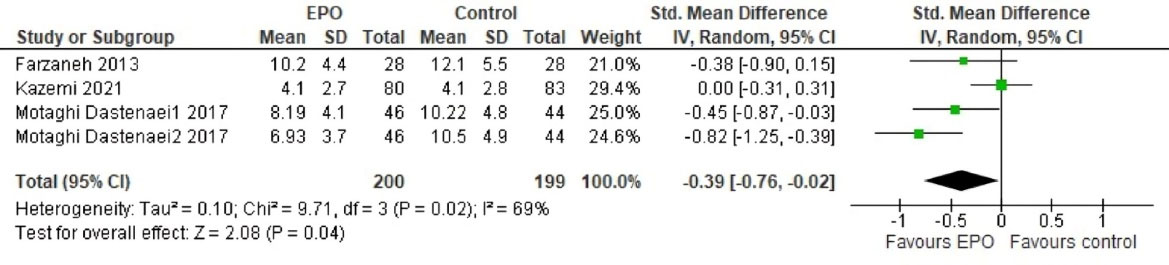
Figure 4.
Forest plot of EPO effect on the duration of hot flashes
.
Forest plot of EPO effect on the duration of hot flashes

Figure 5.
Forest plot of EPO effect on the intensity of hot flashes
.
Forest plot of EPO effect on the intensity of hot flashes
Table 3.
GRADE evidence profiles for outcomes among the trials included in the systematic review
|
Certainty assessment
|
No. of patients
|
Effect
|
Certainty
|
Importance
|
|
No.
|
Study design
|
Risk of bias
|
Inconsistency
|
Indirectness
|
Imprecision
|
Other considerations
|
Epo
|
Comparison
|
Relativ (95% CI)
|
Absolute (95% CI)
|
|
|
|
Frequency of hot flashes
|
| 5 |
randomised trials |
not serious |
seriousa |
not serious |
not serious |
none |
226 |
224 |
- |
MD 2.13 lower
(4.26 lower to 0 ) |
⨁⨁⨁◯ Moderate |
CRITICAL |
|
Duration of hot flashes
|
| 4 |
randomised trials |
not serious |
seriousa |
not serious |
seriousb |
none |
200 |
199 |
- |
SMD 0.39 SD lower
(0.76 lower to 0.02 lower) |
⨁⨁◯◯ Low |
CRITICAL |
|
Intensity of hot flashes
|
| 2 |
randomised trials |
not serious |
not serious |
not serious |
seriousb |
none |
108 |
111 |
- |
SMD 0.19 SD lower (0.45 lower to 0.08 higher) |
⨁⨁⨁◯ Moderate |
CRITICAL |
CI: confidence interval; MD: mean difference; SMD: standardised mean difference.
aThe direction of findings is opposite in some studies and high heterogeneity has been found between studies;
b The optimal information size (OIS) criterion is not meet.
Conclusion
While EPO has demonstrated effectiveness in reducing menopausal symptoms, it is essential to exercise caution when using it in therapy. Providing women with counseling to improve their quality of life during menopause requires a comprehensive understanding of the safety and efficacy of EPO as a therapeutic option for managing menopausal symptoms. Therefore, we recommend conducting further research while adhering to rigorous methodological guidelines to enhance the decision-making process.
Competing Interests
The authors affirm that there are no conflicts of interest related to the publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.
Research Highlights
What is the current knowledge?
-
The main symptoms of menopause are vasomotor symptoms (like hot flashes and night sweats).
-
Most women seek treatment for vasomotor symptoms during menopause, which affects more than 80% of them.
What is new here?
-
EPO, an herbal product, has been found to decrease the duration of hot flashes.
-
Women in the EPO group experienced a decrease in the frequency and intensity of hot flashes compared with the control group; however, these differences were not statistically significant.
Supplementary File
Supplementary file 1. The strategy of searching the main databases
(pdf)
Acknowledgements
We would like to express our appreciation to the Ahvaz Jundishapur University of Medical Sciences for their approval and support in the development of this study. During the preparation of this manuscript, the authors utilized artificial intelligence (AI) tools to enhance the clarity and language quality of the text.
References
- Islam RM, Rana J, Katha S, Hossain MA, Salekin SU, Chowdhury AT. Menopause in low and middle-income countries: a scoping review of knowledge, symptoms and management. Climacteric 2025; 28(3):242-79. doi: 10.1080/13697137.2025.2509254 [Crossref] [ Google Scholar]
- Monteleone P, Mascagni G, Giannini A, Genazzani AR, Simoncini T. Symptoms of menopause - global prevalence, physiology and implications. Nat Rev Endocrinol 2018; 14(4):199-215. doi: 10.1038/nrendo.2017.180 [Crossref] [ Google Scholar]
- Johnson A, Roberts L, Elkins G. Complementary and alternative medicine for menopause. J Evid Based Integr Med 2019; 24:2515690x19829380. doi: 10.1177/2515690x19829380 [Crossref] [ Google Scholar]
- Sussman M, Trocio J, Best C, Mirkin S, Bushmakin AG, Yood R. Prevalence of menopausal symptoms among mid-life women: findings from electronic medical records. BMC Womens Health 2015; 15:58. doi: 10.1186/s12905-015-0217-y [Crossref] [ Google Scholar]
- El Hajj A, Wardy N, Haidar S, Bourgi D, Haddad ME, Chammas DE. Menopausal symptoms, physical activity level and quality of life of women living in the Mediterranean region. PLoS One 2020; 15(3):e0230515. doi: 10.1371/journal.pone.0230515 [Crossref] [ Google Scholar]
- Gartoulla P, Bell RJ, Worsley R, Davis SR. Moderate-severely bothersome vasomotor symptoms are associated with lowered psychological general wellbeing in women at midlife. Maturitas 2015; 81(4):487-92. doi: 10.1016/j.maturitas.2015.06.004 [Crossref] [ Google Scholar]
- Makvandi S, Bastami A, Zargar Shoushtari S, Yazdizadeh H, Etemadpour Y, Taghavifar SA. Quality of life and its related factors in postmenopausal women referred to Ahvaz East Health Center, Iran, 2012. Iran J Obstet Gynecol Infertil 2013; 16(59):6-13. doi: 10.22038/ijogi.2013.1498 [Crossref] [ Google Scholar]
- Alvisi S, Gava G, Orsili I, Giacomelli G, Baldassarre M, Seracchioli R. Vaginal health in menopausal women. Medicina (Kaunas) 2019; 55(10):615. doi: 10.3390/medicina55100615 [Crossref] [ Google Scholar]
- Baker FC, Lampio L, Saaresranta T, Polo-Kantola P. Sleep and sleep disorders in the menopausal transition. Sleep Med Clin 2018; 13(3):443-56. doi: 10.1016/j.jsmc.2018.04.011 [Crossref] [ Google Scholar]
- Flores VA, Pal L, Manson JE. Hormone therapy in menopause: concepts, controversies, and approach to treatment. Endocr Rev 2021; 42(6):720-52. doi: 10.1210/endrev/bnab011 [Crossref] [ Google Scholar]
- Genazzani AR, Monteleone P, Giannini A, Simoncini T. Hormone therapy in the postmenopausal years: considering benefits and risks in clinical practice. Hum Reprod Update 2021; 27(6):1115-50. doi: 10.1093/humupd/dmab026 [Crossref] [ Google Scholar]
- Pinkerton JV. Hormone therapy for postmenopausal women. N Engl J Med 2020; 382(5):446-55. doi: 10.1056/NEJMcp1714787 [Crossref] [ Google Scholar]
- Ebrahimi A, Tayebi N, Fatemeh A, Akbarzadeh M. Investigation of the role of herbal medicine, acupressure, and acupuncture in the menopausal symptoms: an evidence-based systematic review study. J Family Med Prim Care 2020; 9(6):2638-49. doi: 10.4103/jfmpc.jfmpc_1094_19 [Crossref] [ Google Scholar]
- Kargozar R, Azizi H, Salari R. A review of effective herbal medicines in controlling menopausal symptoms. Electron Physician 2017; 9(11):5826-33. doi: 10.19082/5826 [Crossref] [ Google Scholar]
- Karimi L, Larki M, Mohammadi S, Safyari M, Makvandi S. Aromatherapy for the management of menopause symptoms: an updated systematic review and meta-analysis. J Caring Sci 2025; 14(1):58-71. doi: 10.34172/jcs.025.33474 [Crossref] [ Google Scholar]
- Timoszuk M, Bielawska K, Skrzydlewska E. Evening primrose (Oenothera biennis) biological activity dependent on chemical composition. Antioxidants (Basel) 2018; 7(8):108. doi: 10.3390/antiox7080108 [Crossref] [ Google Scholar]
- Montserrat-de la Paz S, Fernández-Arche MA, Ángel-Martín M, García-Giménez MD. Montserrat-de la Paz S, Fernández-Arche MA, Ángel-Martín M, García-Giménez MDPhytochemical characterization of potential nutraceutical ingredients from evening primrose oil (Oenothera biennis L). Phytochem Lett 2014; 8:158-62. doi: 10.1016/j.phytol.2013.08.008 [Crossref] [ Google Scholar]
- Farzaneh F, Fatehi S, Sohrabi MR, Alizadeh K. The effect of oral evening primrose oil on menopausal hot flashes: a randomized clinical trial. Arch Gynecol Obstet 2013; 288(5):1075-9. doi: 10.1007/s00404-013-2852-6 [Crossref] [ Google Scholar]
- Faghani Aghoozi M, Fayazi S, Mohammadi S, Tehranian N, Amerian M. The effects of evening primrose on clinical obstetrics of Iran: a review study. Sci J Nurs Midwifery Paramed Fac 2019; 5(3):15-28. [ Google Scholar]
- Christelle K, Zulkfili MM, Noor NM, Draman N. The effects of evening primrose oil on menopausal symptoms: a systematic review and meta-analysis of randomized controlled trials. Curr Womens Health Rev 2020; 16(4):265-76. doi: 10.2174/1573404816999200702162750 [Crossref] [ Google Scholar]
- Mehrpooya M, Rabiee S, Larki-Harchegani A, Fallahian AM, Moradi A, Ataei S. A comparative study on the effect of “black cohosh” and “evening primrose oil” on menopausal hot flashes. J Educ Health Promot 2018; 7:36. doi: 10.4103/jehp.jehp_81_17 [Crossref] [ Google Scholar]
- Yakoot M, Salem A, Omar AM. Effectiveness of a herbal formula in women with menopausal syndrome. Forsch Komplementmed 2011; 18(5):264-8. doi: 10.1159/000333430 [Crossref] [ Google Scholar]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021; 372:n71. doi: 10.1136/bmj.n71 [Crossref] [ Google Scholar]
- Flemyng E, Moore TH, Boutron I, Higgins JP, Hróbjartsson A, Nejstgaard CH. Using Risk of Bias 2 to assess results from randomised controlled trials: guidance from Cochrane. BMJ Evid Based Med 2023; 28(4):260-6. doi: 10.1136/bmjebm-2022-112102 [Crossref] [ Google Scholar]
- Bell A, Fairbrother M, Jones K. Fixed and random effects models: making an informed choice. Qual Quant 2019; 53(2):1051-74. doi: 10.1007/s11135-018-0802-x [Crossref] [ Google Scholar]
- Maitra S. Fixed-effect versus random-effect model in meta-analysis: how to decide?. Indian J Anaesth 2025; 69(1):143-6. doi: 10.4103/ija.ija_1203_24 [Crossref] [ Google Scholar]
- Zhai C, Guyatt G. Fixed-effect and random-effects models in meta-analysis. Chin Med J (Engl) 2024; 137(1):1-4. doi: 10.1097/cm9.0000000000002814 [Crossref] [ Google Scholar]
- Guyatt GH, Oxman AD, Kunz R, Vist GE, Falck-Ytter Y, Schünemann HJ. What is “quality of evidence” and why is it important to clinicians?. BMJ 2008; 336(7651):995-8. doi: 10.1136/bmj.39490.551019.BE [Crossref] [ Google Scholar]
- Sharif SN, Darsareh F. Impact of evening primrose oil consumption on psychological symptoms of postmenopausal women: a randomized double-blinded placebo-controlled clinical trial. Menopause 2020; 27(2):194-8. doi: 10.1097/gme.0000000000001434 [Crossref] [ Google Scholar]
- Ghavi F, Shakeri F, Farahnaz H, Abdolahian S. Comparison of the effect of fennel and evening primrose oil on menopausal problems and hormonal levels: a randomized controlled trial. Iran J Nurs Midwifery Res 2023; 28(4):430-5. doi: 10.4103/ijnmr.ijnmr_149_22 [Crossref] [ Google Scholar]
- Chenoy R, Hussain S, Tayob Y, O’Brien PM, Moss MY, Morse PF. Effect of oral gamolenic acid from evening primrose oil on menopausal flushing. BMJ 1994; 308(6927):501-3. doi: 10.1136/bmj.308.6927.501 [Crossref] [ Google Scholar]
- Kazemi F, Masoumi SZ, Shayan A, Oshvandi K. The effect of evening primrose oil capsule on hot flashes and night sweats in postmenopausal women: a single-blind randomized controlled trial. J Menopausal Med 2021; 27(1):8-14. doi: 10.6118/jmm.20033 [Crossref] [ Google Scholar]
- Motaghi Dastenaei B, Safdari F, Jafarzadeh L, Raisi Dehkordi Z, Taghizadeh M, Nikzad M. The effect of evening primrose on hot flashes in menopausal women. Iran J Obstet Gynecol Infertil 2017; 20(10):62-8. doi: 10.22038/ijogi.2017.10157 [Crossref] [ Google Scholar]
- Bayles B, Usatine R. Evening primrose oil. Am Fam Physician 2009; 80(12):1405-8. [ Google Scholar]
- Granica S, Czerwińska ME, Piwowarski JP, Ziaja M, Kiss AK. Chemical composition, antioxidative and anti-inflammatory activity of extracts prepared from aerial parts of Oenothera biennis L. and Oenothera paradoxa Hudziok obtained after seeds cultivation. J Agric Food Chem 2013; 61(4):801-10. doi: 10.1021/jf304002h [Crossref] [ Google Scholar]
- Hamazaki K. Role of omega-3 polyunsaturated fatty acids in mental health-studies from Japan. J Oleo Sci 2019; 68(6):511-5. doi: 10.5650/jos.ess19008 [Crossref] [ Google Scholar]
- Al Wattar BH, Talaulikar V. Non-oestrogen-based and complementary therapies for menopause. Best Pract Res Clin Endocrinol Metab 2024; 38(1):101819. doi: 10.1016/j.beem.2023.101819 [Crossref] [ Google Scholar]
- Huntley AL, Ernst E. A systematic review of herbal medicinal products for the treatment of menopausal symptoms. Menopause 2003; 10(5):465-76. doi: 10.1097/01.Gme.0000058147.24036.B0 [Crossref] [ Google Scholar]
- Kronenberg F, Fugh-Berman A. Complementary and alternative medicine for menopausal symptoms: a review of randomized, controlled trials. Ann Intern Med 2002; 137(10):805-13. doi: 10.7326/0003-4819-137-10-200211190-00009 [Crossref] [ Google Scholar]
- Nedrow A, Miller J, Walker M, Nygren P, Huffman LH, Nelson HD. Complementary and alternative therapies for the management of menopause-related symptoms: a systematic evidence review. Arch Intern Med 2006; 166(14):1453-65. doi: 10.1001/archinte.166.14.1453 [Crossref] [ Google Scholar]
- Mehrnoush V, Darsareh F, Roozbeh N, Ziraeie A. Efficacy of the complementary and alternative therapies for the management of psychological symptoms of menopause: a systematic review of randomized controlled trials. J Menopausal Med 2021; 27(3):115-31. doi: 10.6118/jmm.21022 [Crossref] [ Google Scholar]
- Khorshidi M, Zarezadeh M, Moradi Moghaddam O, Emami MR, Kord-Varkaneh H, Mousavi SM. Effect of evening primrose oil supplementation on lipid profile: a systematic review and meta-analysis of randomized clinical trials. Phytother Res 2020; 34(10):2628-38. doi: 10.1002/ptr.6716 [Crossref] [ Google Scholar]