Journal of caring sciences. 14(4):278-292.
doi: 10.34172/jcs.025.33580
Review Article
Social Stigma Associated with COVID-19 in Healthcare Workers: A Concept Analysis
Akram Sadat Sadat Hoseini Conceptualization, Methodology, Supervision, 1 
Anahita Divani Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Validation, Writing – original draft, Writing – review & editing, 2
Javad Nadali Conceptualization, Formal analysis, Investigation, Writing – review & editing, 3, 4 Leily Zare 5, *
Author information:
1Department of Pediatrics & NICU, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran
2Department of Medical Surgical, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran
3Student Research Committee, School of Nursing and Midwifery, Golestan University of Medical Sciences, Gorgan, Iran
4Department of Nursing, School of Nursing and Midwifery, Shahroud University of Medical Sciences, Shahroud, Iran
5Department of Medical Surgical, School of Nursing and Midwifery, Ardabil University of Medical Sciences, Ardabil, Iran
Abstract
Introduction:
Despite the presence of "COVID-19-related social stigma" in health literature, there is no clear definition of this concept in healthcare setting. It is often confused with related terms such as shame, discrimination, and prejudice, leading to imprecise research questions and ineffective evaluations. The aim of this study was to elucidate the concept of social stigma associated with COVID-19 in healthcare workers using Rodgers’ evolutionary concept analysis method.
Methods:
Rodgers’ evolutionary method of concept analysis was employed to clarify COVID-19-related social stigma in healthcare workers. A literature review was conducted using key terms "COVID-19", "social stigma", and related terms in PubMed, Scopus, Cochrane, ProQuest databases, and Google Scholar from January 2019 to September 2024. Among 3993 studies found, 46 were selected for analysis. Data were analyzed using thematic analysis.
Results:
COVID-19-related social stigma among healthcare workers is a multidimensional concept characterized by three primary attributes: Alienation, Humiliation, and Ignorance. The antecedents identified include Fear, Fake news, and the Contagious Nature of the virus. Consequences of this stigma encompass Psychological Issues, Feelings of Worthlessness, Impaired Functionality, and Job Attrition.
Conclusion:
Social stigmatization associated with COVID-19 exerts significant pressure on healthcare workers. It is crucial to understand the factors that exacerbate this issue. Identifying the dimensions of this stigma can provide valuable insights for policymakers and the media. The implementation of preventive measures, such as clear protocols tailored to the public’s educational level and addressing fears of contamination, can improve the situation and reduce the financial strain caused by the loss of healthcare personnel, ultimately enhancing the quality of care.
Keywords: Social stigma, COVID-19, Healthcare workers, Concept analysis, Rodgers
Copyright and License Information
© 2025 The Author(s).
This work is published by Journal of Caring Sciences as an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/). Non-commercial uses of the work are permitted, provided the original work is properly cited.
Funding Statement
None
Introduction
Stigma is a Greek term originally referring to physical marks such as burns or scars that indicate the adverse conditions of an individual. It arises as a result of unfavorable social diagnoses, predictions, and judgments.1Stigmatized people feel rejected, blamed, and worthless. Social stigma is a complex phenomenon with related consequences varying based on the type of disease and the social conditions of the affected people.2,3
In the health system, stigma refers to any labeling or discrimination against individuals with a specific disease.4 Infectious diseases such as acquired immunodeficiency disorder, Ebola, H1N1 flu, and COVID-19 may fuel social stigma.5,6 From smallpox in the 19th century to COVID-19 in the 21st century, epidemics and pandemics have always been associated with stigma.7 During the COVID-19 pandemic, health care providers caring for affected patients faced stigma, possibly due to the infection and fear of contact.6
Stigma can ensure safety by avoiding the source of infection, but it can also lead to direr consequences.8 It is important to distinguish between evading the source of infection and judging people based on their characteristics.9 During the COVID-19 pandemic, health workers faced many stressful events, including stigma, which negatively impacted their relationships, satisfaction, self-efficacy, and physical and mental health.6,10
During the COVID-19 outbreak, like in previous pandemics, healthcare workers were shunned, ostracized, and avoided. While they received public recognition, they also faced stigma, which can create undue pressure. This poses a threat to the lives of those affected by the disease and to the health workers themselves.6 There have been numerous reports of health workers being socially stigmatized worldwide, from being denied the use of public transportation to being insulted on the street to being excluded from rental housing.11 According to a meta-analysis,12 4.10% to 83.80% of healthcare professionals worldwide, including in Iran,13 experience stigma during COVID-19, indicating considerable variation among countries mainly due to differences in healthcare infrastructure and social support. It is worth noting that this phenomenon is more common in low- and middle-income countries.
COVID-19-associated social stigma is often attributed to false beliefs and a lack of awareness within society, and it is frequently overlooked14 and ambiguously used instead of other related concepts such as shame, discrimination, and prejudice.15 This can lead to imprecise research questions, methodology, inefficient research tools, and ineffective evaluation of the concept16 so it is necessary to unpack it. Given the potential long-term effects of COVID-19 social stigma on healthcare workers beyond the pandemic,6 enhancing research to delineate this concept is essential. Such investigations could enrich the understanding of various facets of this phenomenon. Recommendations, including the development of clear educational protocols aimed at mitigating social stigma and enhancing community awareness, may be instrumental for policymakers and healthcare managers in alleviating the negative consequences of social stigma and improving the working conditions for healthcare professionals. The ability to inform and address stigmatizing behaviors of society can help improve the quality of healthcare.17 Given the context-dependent nature of the phenomenon, Rodgers’ method was selected18 to explore the variable concept of healthcare workers’ social stigma, which may continue to evolve with the emergence of COVID-19. The aim of this study was to elucidate the concept of social stigma associated with COVID-19 in healthcare workers using Rodgers’ evolutionary concept analysis method.
Materials and Methods
Due to the variable nature of Covid-19 associated social stigma, Rogers’ seven-step evolutionary model was chosen as the preferred method for analyzing this ever-evolving concept. The steps include: 1) determining the desired concept, 2) identifying alternative terms and related applications of the concept, 3) determining and selecting the scope (suitable set and sample) of data collection, 4) identifying the attributes of the concept, 5) outlining the sources, antecedents, and consequences, 6) specifying the concepts associated with the desired concept, and 7) providing an appropriate example of the concept if needed.19
We followed the guidelines of the PRISMA Extended Program for Scoping Review (PRISMA-ScR).20 We searched databases such as PubMed, Scopus, Web of Science, and Cochrane. In addition, we included relevant grey literature (e.g., theses, dissertations, and conference papers) by searching electronic databases like ProQuest Dissertation and Theses Global, Web of Science, and Google Scholar to retrieve the maximum number of relevant studies. The relevant search terms for “COVID-19” and “social stigma” were found through MeSH, Emtree, and Cochrane platforms. An appropriate search syntax was adopted for PubMed and then customized for other databases (Supplementary file). The search was conducted from January 2019 to September 2024. Additionally, the reference lists of key studies were examined to discover other potentially relevant articles. All studies identified from the literature search were uploaded into Endnote, and duplications were removed. In the screening stage, two reviewers (A.D, and L.Z) independently assessed the title, abstract, and full texts of each study based on the inclusion and exclusion criteria. Any disagreements between the reviewers or uncertainties about particular study details were resolved through discussion or with a third reviewer. Observational-analytic studies (descriptive or cross-sectional studies), case-control studies (retrospective or prospective), and cohort studies that examined social stigma in healthcare workers during COVID-19, Case reports/series, letters, and editorials, written in English and Persian between 2019 and 2024, were included in this study. Studies focused on populations other than healthcare workers were excluded. Out of the 3993 articles obtained, 46 studies were selected based on the inclusion criteria (Figure 1). The selected articles were then coded based on their characteristics, procedures, consequences, contents, and relevant or alternative terms using Rogers’ evolutionary method. To ensure the validity of coding, the data was reviewed by two researchers (A.D, and L.Z). The extracted data were classified, and thematic analysis was used to determine the attributes, antecedents, and consequences (Table 1).
Thematic analysis was guided by Rodgers’ evolutionary concept analysis methodology.19 The process began with a systematic literature review, from which data were extracted and analyzed to identify recurrent themes and define the characteristics (attributes) of the concept. This involved a rigorous and iterative process of comparing and synthesizing findings to distill the essential, related, and borderline attributes that constitute the concept’s core structure.
To further refine the conceptual boundaries, model, borderline, and contrary cases were constructed. The analysis culminated in identifying the antecedents and consequences of the concept, leading to the formulation of a comprehensive operational definition. This structured thematic process ensured a nuanced and systematic exploration of the concept’s evolution and application within the contemporary scholarly context.
Ethical Consideration
This study was a conceptual analysis based exclusively on a systematic review of published literature. As such, it did not involve direct interaction with human subjects, collection of primary personal data, or any experimental procedures that would necessitate a formal ethical approval code from an institutional review board. The methodology relied on the critical analysis and synthesis of existing texts in the public domain. Furthermore, the single personal experience cited in the manuscript is that of the researcher themselves (A.D) provided with full consciousness and consent for its use in this academic context. This reflexive account is included to illuminate the conceptual analysis and is not presented as generalizable data. Every effort has been made to ensure the integrity of the research process, including transparent reporting and adherence to principles of intellectual honesty.
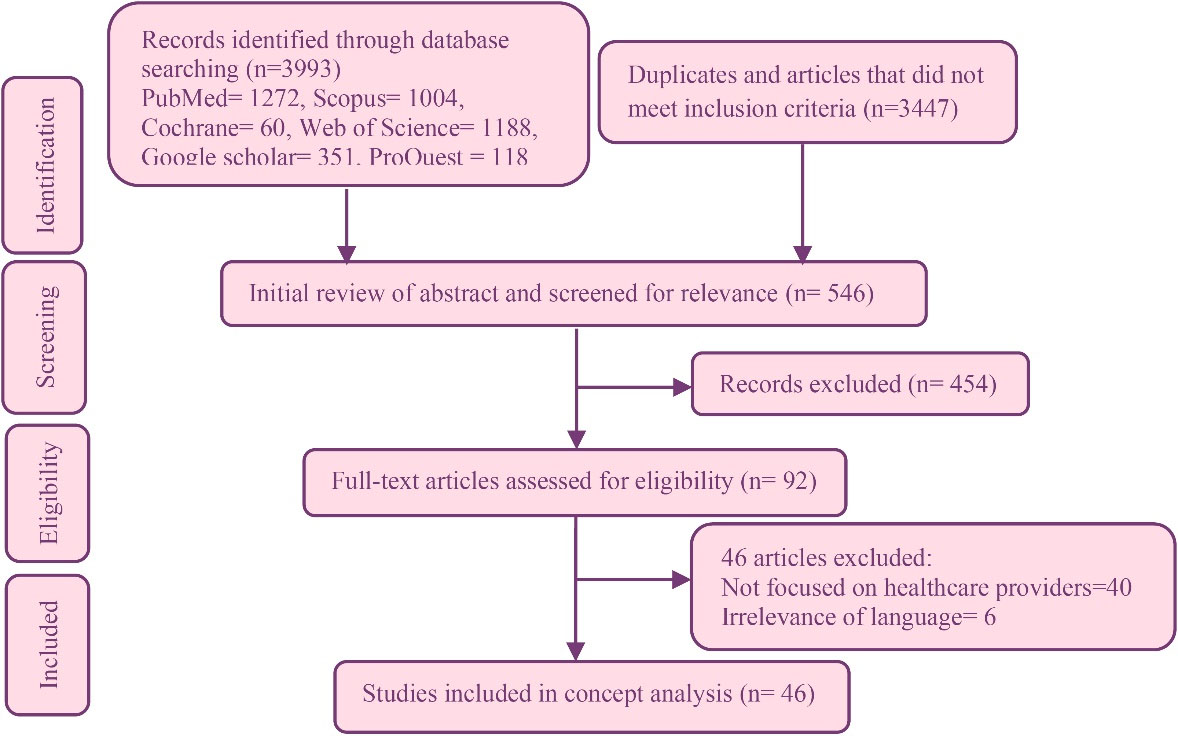
Figure 1.
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources
.
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources
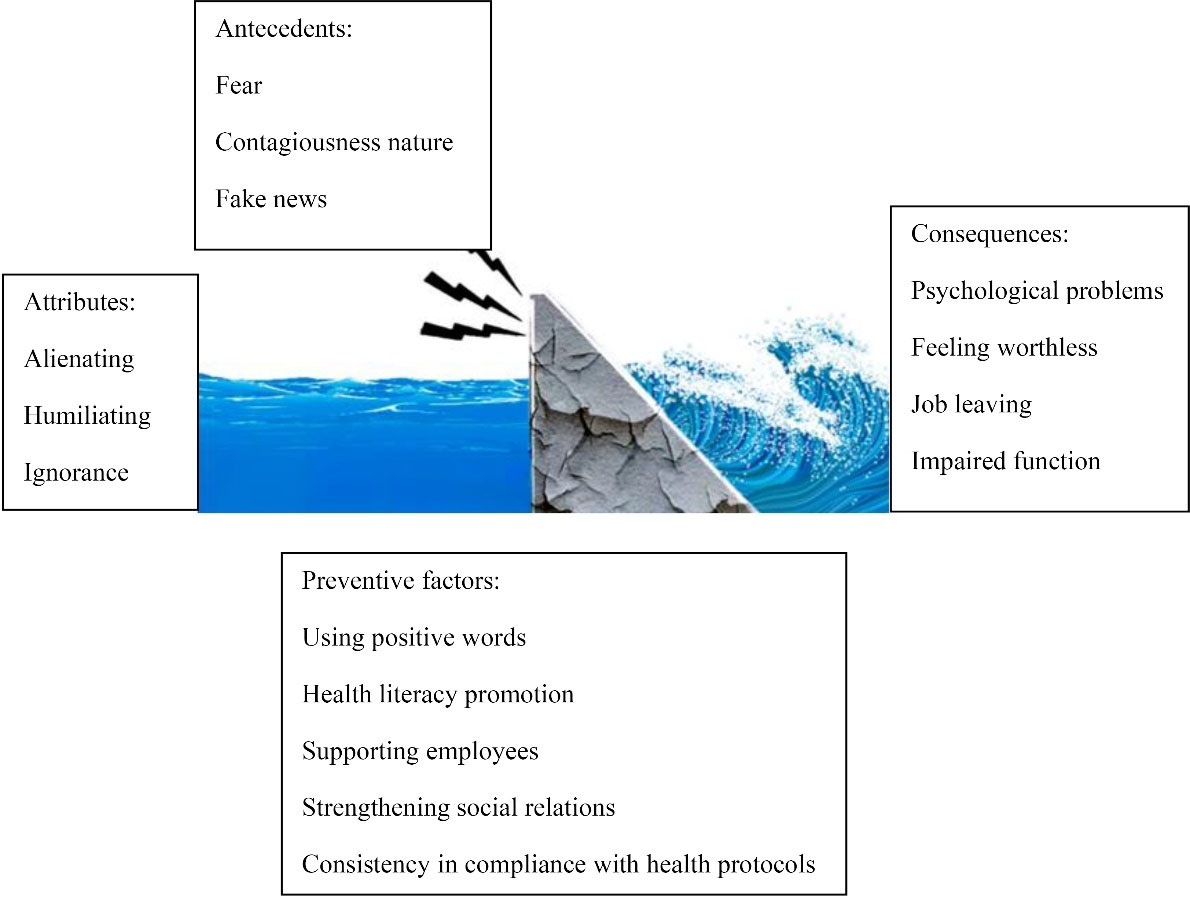
Figure 2.
Water dam model illustrating the extracted attributes, antecedents, consequences, and preventive factors related to the social stigma associated with COVID-19 in healthcare workers
.
Water dam model illustrating the extracted attributes, antecedents, consequences, and preventive factors related to the social stigma associated with COVID-19 in healthcare workers
Results
The Determination of the Desired Concept
In the first step, the ‘significance’ of the chosen concept is a central aspect. ‘Significance’ entails that the chosen concept should be associated with a purposeful human goal in an actual case or praxis, leading to problem-solving.19 According to this description, in this study, the social stigma related to COVID-19 among healthcare workers has been selected as the desired concept for analysis. The purposeful human goal related to this concept is to promote understanding of the impact this concept is having on healthcare workers during the pandemic and lay the foundation for addressing the issue.
The Identification of Alternative Terms and Related Applications of the Concept
In this study, it was found during the analysis process that the concept of social stigma can be replaced by concepts such as shame, discrimination, and prejudice. In terms of related applications of the concept, it can be applied to emotional and psychological support, alleviating loneliness and anxiety, and paving the way for policy development to reduce social stigma and create a safer environment for healthcare activities. Educating society about stigma and its effects may lead to a decrease in fear and discrimination towards healthcare workers, ultimately improving service quality, and helping with workforce recruitment and retention. Additionally, increasing awareness about social stigma and improving responses to health crises can support the well-being of healthcare workers.
The Concept of Social Stigma
The Oxford Dictionary defines stigma as “a mark by which a slave, criminal, etc. is shown, a stain on a good name or an attribute related to a person’s reputation”.65 The APA Dictionary of Psychology defines stigma as “a negative social attitude toward an individual characteristic that may be mental, physical, or a social defect”.4 The term “social stigma” basically refers to the act of addressing people with unfavorable words.66 From a sociological point of view, the concept of stigma was first introduced by Goffman. He believed that stigmatization is caused by human interactions and there is an unfavorable difference or a negative characteristic in the target person.4 Link and Phelan introduced the stigma model, which conceptualizes stigma as a multifaceted process characterized by the acts of labeling and categorizing individuals, linking human differences to negative attributes, reinforcing social divisions between “us” and “them,” and ultimately resulting in status loss and discriminatory practices.67
Building on this, psychologist Patrick Corrigan conceptualizes social stigma as a multifaceted phenomenon comprised of stereotypes (negative beliefs, such as associating mental illness with danger), prejudice (the endorsement of these beliefs, leading to fear or anger), and discrimination (the resulting unfair behavior and denial of opportunities). He crucially distinguishes between public stigma, which is society’s negative reaction, and self-stigma, where individuals internalize these prejudices, leading to diminished self-worth and the “why try” effect. Corrigan further emphasizes that stigma is not merely an individual attitude but is embedded in structural and institutional policies. To combat it, he advocates for three primary approaches—protest, education, and most effectively, direct social contact with individuals in recovery—thereby framing stigma reduction as a practical, evidence-based endeavor essential for social justice and equity.68
Stigma is associated with any unusual health conditions, whether acute or chronic, life-threatening conditions, epidemics, and even weaknesses in the self-management of a disease can be followed by stigma related to the affected person and their caregivers.69 Although social stigmatization of health workers was widespread during the COVID-19 era, little attention was paid to this burdensome condition. Some of the obvious social manifestations of this phenomenon were that people believed that health workers should be prevented from showing their faces in public. They also expected that health workers should be placed in special lounges and separated from their families to avoid transmission of infections.29
Table 1.
Included studies characteristics, and thematic matrix of attributes, antecedents, and consequences mentioned in included articles
|
Author, study type
|
Sample
|
Feature
|
Antecedent
|
Consequence
|
Ramaci et al6
Cross-sectional correlational study |
273 healthcare workers |
NR |
NR |
Stigma has a great impact on employee performance. It may also affect employee compliance and management practices |
Alhouri et al10
Cross-sectional study |
683 healthcare workers |
Harmfulness, inferiority, and Avoidance |
NR |
psychological discomfort (depression-anxiety-stress) |
Grover et al21
Letter to the Editor reporting two case reports |
Two female, health care worker |
Social exclusion, quarantine, maintaining physical distance, using electronic means of communication instead of face-to-face communication, speaking in a derogatory tone. |
Fear of getting sick |
Severe adjustment disorders, thoughts of self-harm, worthlessness in the care of COVID-19 patients |
Adiukwu et al22
Viewpoint article |
No empirical participant sample |
Addressing health workers with words with negative connotations |
Emergence of rumors about COVID-19 |
Impaired mental health of health care providers, need to honor employees |
Kalateh Sadati et al23
thematic analysis study |
24 nurses |
One of the extracted themes was social stigma |
The global epidemic of COVID-19 |
The possibility of impaired mental health in health workers |
Ransing et al24
Letter to the Editor |
No participant sample |
Ignorance of the rights of others due to lack of information or lack of anti-discrimination laws |
Fear of becoming sick and being quarantined |
Healthcare workers experience some degree of stigma. |
Roelen et al25
conceptual review |
No primary sample |
Healthcare workers were not allowed to use public transport and had to vacate the rented houses |
Wide spread of false information about the COVID disease (infodemic), fear of infection |
NR |
Chew et al26
Longitudinal survey |
Residents in training/ n = 274 at baseline, and n = 221 at 3-month follow-up |
NR |
NR |
All residents reported lower perceived stress and stigma compared to baseline |
Shiu et al27
cross-sectional study |
Of the 1421 consented respondents, 357 identified as physicians while 1064 identified as nurses. |
The stigma of COVID-19 and burnout symptoms had a positive correlation.
There was a significant relationship between stigma and profession, which was more severe in physicians than in nurses |
NR |
Participants reported significant levels of stigma |
Mostafa et al28
Cross-sectional study |
509 physicians |
In the review of stigma subscales, "concern with public attitude" was mentioned as the most common source of concern |
NR |
More than a quarter of participants reported severe levels of stigma associated with COVID-19 |
Taylor et al29
Cross-sectional online survey |
3,551 non–healthcare-worker adults |
People who stigmatized HCWs tended to avoid others as well.، avoiding HCWs, imposing severe restrictions on HCWs, such as separating them their community and family |
Fear of infection, HCW stigma is associated with stress and fear of COVID syndrome |
Participation in altruistic support for HCWs (eg, clapping and cheering) was not associated with stigmatizing attitudes |
Singh and Subedi 30
Letter to the Editor |
no primary study sample |
Refusing to speak to healthcare workers and eat with them in a restaurant or cafe |
False information at the community level |
Healthcare workers face a loss of position |
Do Duy et al31
Cross-sectional survey |
61 health-care workers |
The highest level of stigma was found in the context of "negative self-image" and "concern about public perception". In stigmatized healthcare workers, the most common feeling was feeling guilty towards family members and friends, as well as avoiding contact with society |
NR |
NR |
Asadi-Aliabadi et al32
commentary article |
None |
NR |
NR |
Appreciating the role of health care providers can reduce the stigma against them |
Adatara et al33
Descriptive qualitative study |
15 frontline nurses |
NR |
NR |
Frustration so that wanted to resign as frontline nurses |
Taremwa et al34
thematic analysis |
14 frontline healthcare providers |
NR |
Fear of infection and the perception of HCWs being carriers of the disease |
NR |
Memis 35
Descriptive cross-sectional study |
307 nurses |
NR |
NR |
increased professional commitment |
Spruijt et al36
Qualitative study |
53 frontline HCWs |
scolding, discrimination, avoidance, (self-) isolation, and exclusion |
fear of infection and the perception of HCWs being carriers of the disease |
feelings of depression, loneliness, isolation, and the desire to quit job |
Lim et al37
Cross-sectional online survey |
1252 healthcare workers |
being shunned and avoided by families |
NR |
NR |
Tekin et al38
Descriptive, cross-sectional study |
1132 healthcare professionals |
discrimination and status deprivation |
NR |
Depression, insomnia |
Bisenius et al39
Cross-sectional online survey |
371 German adults (final analytic sample) who met "high risk" criteria: recent contact with a confirmed COVID-19 case, symptoms compatible with COVID-19, or return from a high-risk area. |
NR |
fear |
psychological distress |
Osman et al40
Cross-sectional study |
565 Egyptian healthcare providers |
people were moving away from them and unhappiness of their families |
Worry from contracting COVID-19 at work (severe worry), Poor Knowledge |
NR |
Aghaei et al41
Qualitative study |
15 people with persistent COVID-19 symptoms, including 5 health care providers |
NR |
NR |
"Internalize the stigma," “self-blaming," and "fear of being a judge." |
Cruz-Torres and Martín Del Campo-Ríos42
Quantitative, cross-sectional, correlational |
286 Mexican residents (general population), of whom ≈5 worked in a hospital and ≈74 had relatives who worked in a hospital. |
NR |
perceived risk of contagion
social fabric diminishment of the communities |
NR |
Abuhammad et al43
Cross-sectional, survey-based study |
777 Arabic-speaking Jordanian adults with chronic conditions |
NR |
hearing news all time |
NR |
Huarcaya-Victoria et al44
Observational, cross-sectional, correlational survey study |
310 physicians |
NR |
NR |
Depressive symptoms, anxiety, and distress. |
Khoo et al45
Longitudinal qualitative study |
21 frontline primary healthcare workers |
NR |
perceived risk of infection |
NR |
Alfaifi et al46
Analytical cross-sectional study |
Total participants: 301
Quarantined non-healthcare workers: 133
Quarantined healthcare workers: 124
Medical staff working at the quarantine facility: 44 |
NR |
NR |
depression, anxiety, and stress symptoms |
Alnahdi et al47
Cross-sectional, web-based self-administered survey |
407 healthcare workers |
NR |
Ever taking COVID-19 test, gender (being female) |
>Professional burnout |
Soubra et al48
Explorative qualitative study using grounded theory methodology |
20 frontline health and social care workers |
people did not feel safe around them, were not invited to events |
NR |
Difficult coping process |
Al Mutair et al49
Qualitative, cross-sectional phenomenological study |
10 healthcare providers |
treated like criminals, avoiding and running away from them |
NR |
feelings of guilt, fear becoming carriers of the disease |
Hossain et al50
Descriptive qualitative study |
32 frontline healthcare professionals |
Family refused to visit them, avoiding to be close to them |
NR |
Lower work performance |
Kealeboga et al51
Qualitative case study research |
14 nurses working at two COVID-19 care sites |
Not welcome in society |
Working in isolation center |
increased emotions of loneliness, decrease in social connections, psychological stress |
Turki et al52
Cross-sectional web-based survey. |
250 Tunisian healthcare workers |
verbal aggression, physical aggression, avoidance |
pathognomonic symptoms of COVID or taking COVID test |
NR |
Mediavilla et al53
Cross-sectional baseline analysis |
2,053 healthcare workers (inpatient and outpatient staff) |
NR |
NR |
Depression, psychological distress, death thoughts |
Alajmi et al54
Analytical cross-sectional survey. |
226 healthcare workers |
Family avoidance |
NR |
Decrease in overall wellbeing |
Almomani et al55
Descriptive qualitative study |
Twelve nurses providing direct care to patients with COVID-19 |
Avoidance, social isolation |
NR |
Decrease Willingness to work, feeling isolated |
Yufika et al56
Cross-sectional study |
288 health care workers |
NR |
lower education, close contact, lack of adequate protection and protocol |
NR |
Jeleff et al57
Exploratory qualitative study |
30 healthcare workers. |
Avoidance |
NR |
cautious about their behavior |
Tsukuda et al58
Inductive qualitative content analysis |
10 female registered nurses |
being avoided, treated as “dirty” |
NR |
feeling guilty, Nondisclosure |
Sachdeva et al59
cross-sectional study |
150 health care workers |
forced to leave the neighborhood |
NR |
negative image of themselves and feeling guilty, Nondisclosure |
O’Regan-Hyde et al60
Scoping review of qualitative research |
52 included qualitative studies |
altered reactions from society, being excluded from colleagues, family, and community events |
Fear of infection |
NR |
Shetty et al61
Descriptive qualitative study |
Ten registered nurses |
|
lack of awareness |
NR |
Marpaung62
A qualitative descriptive study |
Thirty-three nurses from both urban and rural settings |
feeling shunned, avoided, and rejected |
Being afraid of the threats of COVID-19, false information |
NR |
Ali et al63
Descriptive correlational study design. |
230 nurses |
NR |
|
Decreased self-esteem, lower role efficacy |
Negarandeh et al64
Scoping review |
77 included studies (76 articles + 1 thesis) |
violence and deprivation of social rights |
fear, misinformation, and negative self-image |
adverse biopsychosocial, occupational, and economic consequences |
Shame
Shame is defined as a feeling of sadness, embarrassment, and guilt after committing a wrong or foolish act.70It is a social emotion that is typically experienced following failures, shortcomings, and moral or social transgressions. People feel ashamed when they fail to meet societal or moral expectations and others become aware of this failure, or there is a potential for their awareness. In these situations, individuals may consider the opinions of those who view them negatively or disapprove of them.71 Various conceptualizations of stigma and shame are discussed in the literature, with stigma being described as an outward manifestation of shame. If shame is viewed as an internal response to experiencing stigma, it can be seen as an emotional consequence of stigma.72
Prejudice
Social stigma is defined as a three-component concept that encompasses discrimination, stereotyping, and prejudice.73 Prejudice has been mainly conceptualized as a negative attitude held by someone in relation to the value of specific groups of people, and as a background belief that leads to discrimination as a behavior.74 As claimed by Corrigan, social stigma can have cognitive, affective, and behavioral aspects, with negative attitudes being dominant in the cognitive aspect.73
Discrimination
According to Corrigan’s progressive model of self-stigma, both self-stigma (the negative internalized attitudes that people may have about their own condition) and perceived stigma (concerns the expected reaction of others) consist of three elements: stereotypes, prejudice, and discrimination. Discrimination is defined as a behavioral response to prejudice towards a specific person or group and has been distinguished from stigma by Corrigan’s model.73 Although Corrigan has defined discrimination as a component of stigma, Goffman noted that stigma, as a cognitive-based phenomenon, enables various forms of discrimination that ultimately limit individuals’ opportunities.75 Therefore, these two concepts are distinct but not separate. Furthermore, in contrast to stigma, which is conceptualized with three dimensions including affective, cognitive, and behavioral,73 discrimination has a behavioral nature. It can be concluded that discrimination is the visible face of stigma or enacted stigma.
Determining and Selecting the Appropriate Scope (Set and Sample) of Data Collection
Following PRISMA-ScR, a literature review was conducted using the keywords “COVID-19” and “social stigma” across various databases. Out of 3,993 studies found, 46 were selected for analysis, and data were examined using thematic analysis.
Identifying the Attributes of the Concept
Attributes are the factors that shape the actual definition of a concept and influence its evolution.18 In almost all of the studies mentioned, the consequences of social stigma had a negative impact. In fact, social stigma among healthcare providers during the COVID-19 pandemic has specific characteristics that have been influenced by the current traumatic conditions, resulting in negative outcomes (Table 2). In this study, three major attributes of the concept were identified: alienation, humiliation, and ignorance.
Alienating
An important issue associated with the psychological experience of physically ill individuals is social alienation. In these situations, interactions with friends and family may be strained or unpleasant. The social isolation that individuals experience as a result of their illnesses can lead to anxiety, depression, low self-esteem, and feelings of social stigma. Conversely, those caring for these patients also face social isolation due to their close proximity to them. Diseases vary significantly in terms of their origins (whether caused by contagion or genetics), nature, locus of control (whether the disease can be managed through behavior or not), and the patient’s gender, ethnicity, or age. The origin of a disease is a key factor in the social stigmatization of physical illnesses. Several studies have shown that the belief that the onset of a disease is controllable leads to increased levels of social isolation. This perceived disruption of social relationships largely contributes to the reasons for social rejection. During COVID-19, individuals tried to avoid any contact with the healthcare workers because they were in close and direct contact with patients. This imposed severe restrictions on the healthcare workers.76
Table 2.
Antecedents, features, consequences, and preventive factors extracted from studies
|
Analysis unit category
|
| Antecedents |
| Fear |
| Fake news |
| Contagious nature |
| Attributes |
| Alienating |
| Humiliating |
| Ignorance |
| Consequences |
| Psychological problems |
| Feeling worthless |
| Impaired function |
| Leaving the job |
| Preventive factors |
| Using positive words |
| Health literacy promotion |
| Supporting employees |
| Strengthening social relations |
| Consistency in compliance with health protocols |
Humiliation
Embarrassment, shame, guilt, and humiliation all reflect the presence of value systems. Shame and guilt typically stem from self-evaluation, while embarrassment and humiliation are often the result of external evaluation. Humiliation does not always involve violence or coercion; it can occur through passive means such as being ignored, taken for granted, or denied certain rights or privileges. People can also feel humiliated through rejection, abandonment, abuse, or betrayal.77 it was found that despite facing life-threatening situations, medical staff often willingly cared for patients whose families were sometimes hesitant to do so. Despite their altruistic actions, cases of humiliation against healthcare workers, both at work and at home, have been reported. For example, they have been shunned by family members or subjected to harsh conversations.21,30 Overall, employees providing healthcare to COVID-19 patients have faced derogatory remarks in social interactions, reflecting negative attitudes towards them.
Ignorance
Information ignorance causes many problems in the COVID-19 pandemic. Many people were afraid to even approach healthcare workers or did not want to talk to them. Without good health literacy, individuals are unable to effectively distinguish facts from fictions and can permit unreliable information to influence their behaviors. This can be harmful not only to the individual, but also to the whole society.78 One of the reasons leading to the discriminatory behavior of the general public towards medical workers, despite their outstanding performance, could be their insufficient knowledge of and lack of familiarity with human rights. Any humiliation and insult in dealing with others, including health workers, is considered as a violation of rights. Health workers expressed their most serious concerns about the public attitude. Lack of information plays a major role in posing this challenge. Poor health literacy, both morally and behaviorally, can cause communication problems.79 In general, due to the lack of sufficient information about the nature of the disease and its mode of transmission, the society has experienced extreme fear, which has led to healthcare workers being considered as carriers of the disease and avoided the health care providers. Lack of information, both in form of being unaware of people’s rights or not knowing the nature of the disease, has caused verbal and non-verbal violent behaviors against health care providers. People in the society have kept their physical distance from health workers in an unusually discriminatory manner so that they have been stigmatized in their social relations. A study on conceptualizing the stigma associated with head lice disease,80 showed lack of information about the nature of the disease and its mode of transmission as one of the disease-associated stigma features.
Outlining the Sources, Antecedents, and Consequences of the Target Concept
Antecedents are the situations or contexts in which a concept occurs. The history of social stigma associated with COVID-19 in healthcare workers include fear of becoming infected, the contagiousness of the disease, and the spread of fake news.
Fear of Becoming Infected and Contagiousness of the Disease
Fear is directly related to the level of contagion as well as the complication and mortality of COVID-19. At high levels of fear, people may not think properly and rationally when responding to COVID-19.81 In communities with higher cases of COVID-19, there is an obvious fear,82 which can indicate that during the peak stages of disease, the condition may deteriorate. The level of social stigma in healthcare workers is related to the fear driven by COVID-19.29 Fear is a basic emotion that is activated in response to a perceived threat with physical, interpersonal, cognitive, and behavioral characteristics.83 Fear of contracting a disease destroys interpersonal relationships with health workers and is considered one of the reasons for stigmatizing them.
Fake News
Fake news can spread through our culture like a contagious disease.84 It has been identified as a growing issue during the pandemic by public health organizations like the World Health Organization. It is crucial to minimize the impact of factors like political or commercial influences during COVID-19, as this can serve as a remedy to this problem.85 The dissemination of misinformation among the public contributes to the social stigmatization of health service providers. For example, public transport drivers may refuse to provide services to health care workers, and landlords may end contracts with tenants who work in hospitals.
Consequences
Consequences result from experiencing a phenomenon.18 In this study, they included having psychological problems, feeling worthless and dysfunctional, and leaving the job.
Psychological Problems
The unknown nature of COVID-19 has had a significant impact on people’s mental health. The psychological effects linked to the fear of COVID-19 are deemed more dangerous than the disease itself. Anxiety, fear, and stress have led individuals to stockpile surgical masks, use hand sanitizers excessively, and overly protect themselves and their loved ones from COVID-19. People are constantly washing their hands, diligently cleaning their homes, and are wary of anyone who coughs or sneezes. Psychologists have also confirmed that this situation can lead to mental distress for healthcare workers.86
Feeling Worthless
Health care providers felt devalued after receiving messages indicating social stigma for providing services to patients with COVID-19. They stated that working in the COVID-19 departments was so demoralizing that they preferred to change their workplaces.21
Job Leaving
Although most health service providers consider their roles to be constructive and supportive during the COVID-19 pandemic,86 stigmatizing behaviors significantly impact their well-being, performance, and job satisfaction. This influence is so strong that some providers may even choose to leave their jobs.30
Water Dam Model
Given the exploration of different dimensions of COVID-19 related social stigma in health care staff, anti-stigma factors can be seen as a dam to the main characteristics of stigma. The stronger the dam is, the better it will stand against the pressure of water. Not only will it prevent flooding, but it also will be benefited the potential energy of the water. In addition to standing in front of the water, this dam resists a number of external factors that can be compared to the precursors of social stigma. If the pressure of these external factors, which are the antecedents of stigma, exceeds the resistance of the dam, which has the protective and anti-stigma potential in the society, it will cause the dam to be weakened and damaged. In this context, the water which shows the stigmatized features remained behind the dam and its potential was used to encourage the public to comply with health protocols as much as possible, such as maintaining physical distance, using personal protective equipment, and visiting medical centers early on in case of symptoms of illness. The water has currently become a raging slap that destroys and carries away everything in its path. The consequences of social stigma are like this flood, which can even lead to resignation. In general, it is reasonable that the public and officials be aware of the stigma associated with COVID-19 in healthcare workers by considering its characteristics, antecedents and consequences so that they can successfully take steps in planning and promoting anti-stigma features in the society (Figure 2).
Specifying the Concepts Associated with the Desired Concept
The most common related concepts include shame, self-concept, and self-efficacy.
Shame is defined as a feeling of sadness, embarrassment, and guilt after doing something perceived as wrong or stupid.87,88 Social stigma is seen as an external sign, while shame is an internal feeling.72 Therefore, shame can be characterized by feelings such as self-hatred, embarrassment, defeat, and hopelessness that result from social stigma.
Self-concept is defined as one’s perception of themselves.89 It is constantly changing based on events and feedback individuals receive in their daily lives. Positive self-concept can act as a defense mechanism against the destructive behavior of others.90 Therefore, reactions and social behaviors resulting from stigma can negatively impact people’s self-concept and ultimately lead to the internalization of that stigma.
Self-efficacy refers to a person’s ability to perform at an expected level, which is influenced by events and, in turn, influences those events. The social-cognitive model of internalized stigma emphasizes a significant correlation between stigmatization and disrupted self-efficacy.91 Consequently, experiencing stigma from society can lower self-efficacy, affecting a person’s performance quality as a destructive factor. Based on the aforementioned cases, factors such as the contagiousness of the disease, fear of contracting it, and fake news about it contribute to the social stigmatization of healthcare workers. This phenomenon is evident in the social exclusion and humiliation of health service providers, as well as a lack of accurate information in society. Ultimately, this stigma leads to negative consequences such as psychological distress among healthcare workers, feelings of worthlessness and ineffectiveness, and ultimately, attrition from their jobs.
Prevention of Social Stigma Associated with COVID-19
Using positive language and avoiding exaggeration when discussing COVID-19 and its complications is crucial. It is important to implement interventions that aim to educate the public and correct their attitudes towards the disease. The media plays a significant role in this effort. Additionally, supporting frontline workers, adhering to health protocols, and implementing measures such as quarantine, testing, and travel restrictions for the entire community are effective ways to prevent the spread of the virus and reduce social stigma. It is also important to strengthen social connections. Rather than promoting social distancing, people should be encouraged to maintain physical distance to help control the spread of the disease.92 The social stigma associated with COVID-19 can increase the burden on healthcare providers, so it is essential to use an information-based approach to prevent stigmatizing behavior towards them in the society. This includes engaging with opinion leaders and taking steps to reduce stigma against healthcare workers.
Providing an Appropriate Example of the Concept
An example is a case identified by the researcher that illustrates the practical application of a concept.19 A.D is a 27-year-old nurse working in the COVID-19 intensive care unit. Upon receiving an order from the nursing office to work in the intensive care department, she faced pressure and negative reactions from people. Friends and family constantly warned her about the highly contagious nature of the disease, stating that most nurses caring for COVID-19 patients became infected and often died. After a few weeks in the intensive care unit, her friends only contacted her through phone calls and avoided visiting in person. Upon returning home, she encountered feelings of obsession and concern from family members about potential contamination of the house, dishes, clothes, etc. Family members repeatedly reminded her to eat alone and stay in her room. When attempting administrative work, employees refused her entry, insisting she make requests over the phone. Despite assuring others of her vaccination status and adherence to hygiene and distancing protocols, many believed these measures were ineffective due to her direct and prolonged contact with COVID-19 patients. After two months in the COVID-19 department, she began experiencing anxiety and burnout from the long hours and patient care. Not only was her work undervalued in society, but she also faced labels and negative feedback from those around her. The pressure from friends and family escalated to the point where she was excluded from family gatherings. She lost motivation to care for COVID-19 patients and contemplated leaving her job to be treated like everyone else.
As exemplified by this example, the stigma associated with COVID-19 among healthcare providers is marked by social exclusion, humiliation, and a lack of information. This concept has both antecedents and consequences. In this case, the antecedents consist of fear, misinformation, and the highly contagious nature of COVID-19. The resulting consequences manifest as psychological issues, feelings of worthlessness, impaired functioning, and a desire to leave their job.
Discussion
The social stigma associated with COVID-19 in healthcare workers is a variable phenomenon that is mostly considered negative. Since the outbreak of COVID-19, lack of information in the society, fear of the disease, rumor spread, and stigmatization of people have been more dangerous than the spread of COVID-19 itself.93
The social rejection of healthcare workers and humiliating behaviors towards them are severe characteristics of COVID-19 associated social stigma in healthcare workers. The humiliating behavior against health workers during other epidemics has been reported94 as it is evident in the outbreak of COVID-19.
In most cases, the characteristics of COVID-19 associated social stigma appear in the context of spreading false news. A systematic review investigating the prevalence of social stigma associated with infectious diseases including COVID-19,12showed that stigmatizing behavior is related to the level of education. Accordingly, those with lower education levels showed more stigmatizing behaviors. This can indicate that by increasing the level of education, the person obtains reliable news from reliable sources, and as a result, stigmatization is reduced. Meanwhile, the high contagiousness of the disease and the fear of contracting disease could act as other important causes.
Khatooni analyzed the concept of stigma in the context of COVID-19 within society using Rogers’ method.95 The study found that social stigma was identified as one of the attributes, leading to psychological issues as a consequence. The similarities noted may be due to the shared concept and context under study. However, there were also differences in the results, which could be because of the different populations studied; while they focused on the general population, we specifically looked at healthcare workers. Criticism was raised regarding their limited search time and restricted database, while we included literature from the beginning of COVID-19 until September 2024. Additionally, we have searched wider databases to include grey literature as well.
If the condition for the presence of COVID-19 associated social stigma is present in the society, its consequences will be also visible. These consequences included psychological problems in employees, the feelings of worthlessness in providing care for patients with COVID-19, and impaired functions among workers. Such consequences, can even lead to leaving the job. According to the relevant literature, the incidence of mental disorders in the stigmatized group in the society are so common that can even lead to the loss of educational and job status.96,97 A study investigated stigma-related experiences of people with severe mental illness and found that the feeling of worthlessness associated with stigma is strongly related to the patients’ previous experiences of empowerment or rejection.98 Consequently, it can be concluded that rejecting people because of the social stigma can make them feel worthless and worsen the situation. A study analyzing the concept of stigma in the patients with head lice, defined the concept of stigma as the presence of disease symptoms, unfair and negative opinions, and shame.80 One of the factors underlying stigma was the negative perception of the disease itself and the affected people, which did not have much convergence with the results of the present study. However, in terms of the beliefs and perceptions of the disease, their findings were similar to the results of the present study. It can be concluded that the wrong perception of the disease is due to the lack of information and low health literacy, and this dissimilarity can be due to the different nature of the disease.
A review study investigated mental illness-related stigma in healthcare workers, demonstrating the concept of stigma in terms of negative attitudes and behaviors, ignorance, and pessimism towards treatment, as well as the dominant culture of that society.99 These findings align with the results of the present study, both highlighting unawareness as a main cause of stigmatizing behavior. The present study’s results indicate that people’s lack of awareness of their rights can justify the occurrence of discriminatory and stigmatizing behavior towards them. Similarly, another study found that healthcare workers’ lack of awareness of patients’ rights and misconceptions about mental illness could trigger their discriminatory behaviors, leading to negative outcomes.100
Furthermore, Betty Neuman’s systemic theory can justify the usefulness of this conceptualization. According to this theory, healthcare workers are considered components of open systems that are in constant exchange of energy with their surroundings. In their interactions with the environment, individuals face various sources of stress, which can be precursors of social stigma. Factors such as emerging epidemics on a large scale, frequent changes in treatment departments, shifts in job status for health workers, high mortality rates, widespread dissemination of often false information without scientific basis, and the high contagiousness of COVID-19 are considered predictors of stress in providing healthcare services. Neuman’s theory suggests that flexible, normal, and resistant lines from the outside to the inside are responsible for protecting the structure and wholeness of a person. If these stressors increase to a point beyond an individual’s tolerance and the triple lines of resistance are broken, the central structure is damaged, leading to the emergence of consequences of social stigma. Based on Neuman’s system theory, as well as the propositions and concepts derived from this study and other similar studies, it can be concluded that identifying the characteristics, antecedents, and consequences of the concept will help in better understanding COVID-19 associated social stigma in healthcare workers. By recognizing these factors, it is possible to control stressors in the work environment of healthcare workers and strengthen their defense lines through policy adoption and implementation.101
Limitations and Directions
The limitations of the present study include only considering English and Persian articles and not always having access to full-text articles. Because this concept is influenced by society’s culture, a hybrid model is recommended for future studies. It is also recommended to investigate the long-term effects of COVID-19-related social stigma on the performance and attrition rates of health professionals. Subsequently, interventions should be developed to address traumatic stigma experiences, and their effectiveness should be investigated through interventional research.
Conclusion
The stigma associated with COVID-19 among health workers is complex and results in social rejection, humiliation, and a lack of information about the disease. Preventive measures could help overcome this stigma. If the factors leading to stigma increase in society or if anti-stigma measures decrease, different dimensions of stigma may arise. It is crucial for people at all levels to be aware of these influential factors during the COVID-19 epidemic to mitigate its damaging consequences. By clarifying the concept of stigma associated with the COVID-19 pandemic, valuable information can be provided to policymakers, health managers, and the media to reduce the financial burden caused by the loss of medical staff, ultimately improving the quality of care. Understanding how the stigma surrounding COVID-19 impacts healthcare workers can have significant implications for both the workers themselves and the healthcare services provided in communities, as well as potential future pandemics. This understanding can also shed light on the challenges faced by healthcare workers during this time, increasing public awareness and potentially leading to the development of support programs within policy-making institutions for future pandemics. Since the implications of COVID-19-related stigma are still not well explored among healthcare workers, there are opportunities for further research using hybrid methods.
Competing Interests
None.
Data Availability Statement
Data cannot be shared openly but are available on request from corresponding author.
Ethical Approval
Not applicable.
Supplementary Files
Supplementary file. Search Syntax
(pdf)
Research Highlights
What is the current knowledge?
What is new here?
-
Demonstrated the COVID-19-related social stigma towards healthcare providers, its characteristics, root causes, and repercussions, along with potential interventions to tackle and diminish social stigma in healthcare environments.
Main findings:
-
COVID-19 stigma among healthcare workers arises from fear, misinformation, and social misconceptions, manifesting through alienation and humiliation, and leading to psychological distress, reduced performance, and job withdrawal.
-
Preventive actions include positive communication, health literacy enhancement, organizational and peer support, and fostering cohesive social and professional relationships.
Acknowledgements
The research team appreciates the Tehran University of Medical Sciences.
References
- Goffman E. Stigma: Notes on the Management of Spoiled Identity. Simon and Schuster; 2009.
- Lv XQ, Feng Y, Li JR, Zhang XQ, Xiang R, Hong JF. Validation of a Chinese version of the short-form Cataldo lung cancer stigma scale. Heart Lung 2022; 51:59-66. doi: 10.1016/j.hrtlng.2021.08.004 [Crossref] [ Google Scholar]
- Özdemir Ö, Kaya Y, Adagide S. Nursing students’ attitudes toward seeking psychological help associated to self-stigma and perceived social stigma. J Caring Sci 2023; 12(4):221-7. doi: 10.34172/jcs.2023.33094 [Crossref] [ Google Scholar]
- Goffman E. Selections from stigma. In: Davis LJ, eds. The Disability Studies Reader. Routledge; 1997.
- Smith-Morris C. Epidemiological placism in public health emergencies: Ebola in two Dallas neighborhoods. Soc Sci Med 2017; 179:106-14. doi: 10.1016/j.socscimed.2017.02.036 [Crossref] [ Google Scholar]
- Ramaci T, Barattucci M, Ledda C, Rapisarda V. Social stigma during COVID-19 and its impact on HCWs outcomes. Sustainability 2020; 12(9):3834. doi: 10.3390/su12093834 [Crossref] [ Google Scholar]
- Pfefferbaum B, North CS. Mental health and the COVID-19 pandemic. N Engl J Med 2020; 383(6):510-2. doi: 10.1056/NEJMp2008017 [Crossref] [ Google Scholar]
- Fischer LS, Mansergh G, Lynch J, Santibanez S. Addressing disease-related stigma during infectious disease outbreaks. Disaster Med Public Health Prep 2019; 13(5-6):989-94. doi: 10.1017/dmp.2018.157 [Crossref] [ Google Scholar]
- Johnson BB. Hazard avoidance, symbolic and practical: the case of Americans’ reported responses to Ebola. J Risk Res 2019; 22(3):346-63. doi: 10.1080/13669877.2017.1378252 [Crossref] [ Google Scholar]
- Alhouri A, Abu Shokor M, Marwa K, Sharabi A, Mohammad Nazir Arrouk D, Al Houri FN. COVID-19 and its impact on healthcare workers: understanding stigma, stress, and quality of life. Cureus 2023; 15(4):e37846. doi: 10.7759/cureus.37846 [Crossref] [ Google Scholar]
- Bhanot D, Singh T, Verma SK, Sharad S. Stigma and discrimination during COVID-19 pandemic. Front Public Health 2020; 8:577018. doi: 10.3389/fpubh.2020.577018 [Crossref] [ Google Scholar]
- Yuan K, Huang XL, Yan W, Zhang YX, Gong YM, Su SZ. A systematic review and meta-analysis on the prevalence of stigma in infectious diseases, including COVID-19: a call to action. Mol Psychiatry 2022; 27(1):19-33. doi: 10.1038/s41380-021-01295-8 [Crossref] [ Google Scholar]
- Zandifar A, Badrfam R, Mohammadian Khonsari N, Mohammadi MR, Asayesh H, Qorbani M. Prevalence and associated factors of posttraumatic stress symptoms and stigma among health care workers in contact with COVID-19 patients. Iran J Psychiatry 2020; 15(4):340-50. doi: 10.18502/ijps.v15i4.4303 [Crossref] [ Google Scholar]
- Dye TD, Alcantara L, Siddiqi S, Barbosu M, Sharma S, Panko T. Risk of COVID-19-related bullying, harassment and stigma among healthcare workers: an analytical cross-sectional global study. BMJ Open 2020; 10(12):e046620. doi: 10.1136/bmjopen-2020-046620 [Crossref] [ Google Scholar]
- Salih MH, Landers T. The concept analysis of stigma towards chronic illness patient. Hospice and Palliative Medicine International Journal 2019; 3(4):132-6. doi: 10.15406/hpmij.2019.03.00166 [Crossref] [ Google Scholar]
- Beecher C, Devane D, White M, Greene R, Dowling M. Concept development in nursing and midwifery: an overview of methodological approaches. Int J Nurs Pract 2019; 25(1):e12702. doi: 10.1111/ijn.12702 [Crossref] [ Google Scholar]
- Nyblade L, Stockton MA, Giger K, Bond V, Ekstrand ML, Lean RM. Stigma in health facilities: why it matters and how we can change it. BMC Med 2019; 17(1):25. doi: 10.1186/s12916-019-1256-2 [Crossref] [ Google Scholar]
- Rodgers BL. Concepts, analysis and the development of nursing knowledge: the evolutionary cycle. J Adv Nurs 1989; 14(4):330-5. doi: 10.1111/j.1365-2648.1989.tb03420.x [Crossref] [ Google Scholar]
- Rogers BL. Concept analysis an evolutionary view. 2nd ed. In: Concept Development in Nursing Foundations, Techniques and Applications. Philadelphia: WB Saunders Company; 2000.
- Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med 2018; 169(7):467-73. doi: 10.7326/m18-0850 [Crossref] [ Google Scholar]
- Grover S, Singh P, Sahoo S, Mehra A. Stigma related to COVID-19 infection: are the health care workers stigmatizing their own colleagues?. Asian J Psychiatr 2020; 53:102381. doi: 10.1016/j.ajp.2020.102381 [Crossref] [ Google Scholar]
- Adiukwu F, Bytyçi DG, El Hayek S, Gonzalez-Diaz JM, Larnaout A, Grandinetti P. Global perspective and ways to combat stigma associated with COVID-19. Indian J Psychol Med 2020; 42(6):569-74. doi: 10.1177/0253717620964932 [Crossref] [ Google Scholar]
- Kalateh Sadati A, Zarei L, Shahabi S, Heydari ST, Taheri V, Jiriaei R. Nursing experiences of COVID-19 outbreak in Iran: a qualitative study. Nurs Open 2021; 8(1):72-9. doi: 10.1002/nop2.604 [Crossref] [ Google Scholar]
- Ransing R, Ramalho R, de Filippis R, Ojeahere MI, Karaliuniene R, Orsolini L. Infectious disease outbreak related stigma and discrimination during the COVID-19 pandemic: drivers, facilitators, manifestations, and outcomes across the world. Brain Behav Immun 2020; 89:555-8. doi: 10.1016/j.bbi.2020.07.033 [Crossref] [ Google Scholar]
- Roelen K, Ackley C, Boyce P, Farina N, Ripoll S. COVID-19 in LMICs: the need to place stigma front and centre to its response. Eur J Dev Res 2020; 32(5):1592-612. doi: 10.1057/s41287-020-00316-6 [Crossref] [ Google Scholar]
- Chew QH, Chia FL, Ng WK, Lee WC, Tan PL, Wong CS. Perceived stress, stigma, traumatic stress levels and coping responses amongst residents in training across multiple specialties during COVID-19 pandemic-a longitudinal study. Int J Environ Res Public Health 2020; 17(18):6572. doi: 10.3390/ijerph17186572 [Crossref] [ Google Scholar]
- Shiu C, Chen WT, Hung CC, Huang EP, Lee TS. COVID-19 stigma associates with burnout among healthcare providers: evidence from Taiwanese physicians and nurses. J Formos Med Assoc 2022; 121(8):1384-91. doi: 10.1016/j.jfma.2021.09.022 [Crossref] [ Google Scholar]
- Mostafa A, Sabry W, Mostafa NS. COVID-19-related stigmatization among a sample of Egyptian healthcare workers. PLoS One 2020; 15(12):e0244172. doi: 10.1371/journal.pone.0244172 [Crossref] [ Google Scholar]
- Taylor S, Landry CA, Rachor GS, Paluszek MM, Asmundson GJG. Fear and avoidance of healthcare workers: an important, under-recognized form of stigmatization during the COVID-19 pandemic. J Anxiety Disord 2020; 75:102289. doi: 10.1016/j.janxdis.2020.102289 [Crossref] [ Google Scholar]
- Singh R, Subedi M. COVID-19 and stigma: social discrimination towards frontline healthcare providers and COVID-19 recovered patients in Nepal. Asian J Psychiatr 2020; 53:102222. doi: 10.1016/j.ajp.2020.102222 [Crossref] [ Google Scholar]
- Do Duy C, Nong VM, Ngo Van A, Doan Thu T, Do Thu N, Nguyen Quang T. COVID-19-related stigma and its association with mental health of health-care workers after quarantine in Vietnam. Psychiatry Clin Neurosci 2020; 74(10):566-8. doi: 10.1111/pcn.13120 [Crossref] [ Google Scholar]
- Asadi-Aliabadi M, Tehrani-Banihashemi A, Moradi-Lakeh M. Stigma in COVID-19: a barrier to seek medical care and family support. Med J Islam Repub Iran 2020; 34:98. doi: 10.34171/mjiri.34.98 [Crossref] [ Google Scholar]
- Adatara P, Kuug AK, Nyande FK, Klutsey EE, Johnson BB, Nyefene MK. A qualitative study on frontline nurses’ experiences and challenges in providing care for COVID-19 patients in the Volta region of Ghana: implications for nursing management and nursing workforce retention. Healthcare (Basel) 2023; 11(7):1028. doi: 10.3390/healthcare11071028 [Crossref] [ Google Scholar]
- Taremwa IM, Ashaba S, Naggayi BRK, Kayongo B, Nimwesiga C, Ayebazibwe C. Psychosocial challenges of the coronavirus disease-2019 pandemic among frontline health care providers and their coping mechanisms at Mbarara Regional Referral Hospital, southwestern Uganda. Psychol Res Behav Manag 2023; 16:549-60. doi: 10.2147/prbm.S399687 [Crossref] [ Google Scholar]
- Memis A, Karapelit Z. The relation between nurses’ perception of social stigmatization and professional commitment during the COVID 19 pandemic. Int J Caring Sci 2023; 16(2):850-8. [ Google Scholar]
- Spruijt I, Cronin A, Udeorji F, Nazir M, Shehu S, Poix S. Respected but stigmatized: healthcare workers caring for COVID-19 patients. PLoS One 2023; 18(7):e0288609. doi: 10.1371/journal.pone.0288609 [Crossref] [ Google Scholar]
- Lim CS, See B, Teo DC, Tan MS, Hassan N, Tee A. Risk perception and psychosocial impact during the early period of the COVID-19 pandemic on healthcare workers. BJPsych Open 2023; 9(S1):S57-8. doi: 10.1192/bjo.2023.205 [Crossref] [ Google Scholar]
- Tekin C, Karakaş N, Akbulut S, Kurt H, Bentli R. Stigmatization of healthcare professionals during the COVID-19 pandemic: their psychosocial states and the factors affecting them. J Psychiatr Nurs 2023; 14(2):120-9. doi: 10.14744/phd.2022.83436 [Crossref] [ Google Scholar]
- Bisenius S, Treml J, Hanschmidt F, Kersting A. Stigmatization profiles and psychological distress in people at high risk of infection with COVID-19 - a study conducted in Germany from March to August 2021. PLoS One 2023; 18(5):e0285788. doi: 10.1371/journal.pone.0285788 [Crossref] [ Google Scholar]
- Osman DM, Khalaf FR, Ahmed GK, Abdelbadee AY, Abbas AM, Mohammed HM. Worry from contracting COVID-19 infection and its stigma among Egyptian health care providers. J Egypt Public Health Assoc 2022; 97(1):2. doi: 10.1186/s42506-021-00099-6 [Crossref] [ Google Scholar]
- Aghaei A, Zhang R, Taylor S, Tam CC, Yang CH, Li X, et al. Impact of COVID-19 symptoms on social aspects of life among female long haulers: a qualitative study. Res Sq [Preprint]. February 10, 2022. Available from: https://pubmed.ncbi.nlm.nih.gov/35169790/.
- Cruz-Torres CE, Martín Del Campo-Ríos J. Stigmatization towards healthcare personnel during the first COVID-19 wave in Central and Northern Mexico. PeerJ 2022; 10:e14503. doi: 10.7717/peerj.14503 [Crossref] [ Google Scholar]
- Abuhammad S, Alzoubi KH, Al-Azzam S, Alshogran OY, Ikhrewish RE, Amer ZW. Stigma toward healthcare providers from patients during COVID-19 era in Jordan. Public Health Nurs 2022; 39(5):926-32. doi: 10.1111/phn.13071 [Crossref] [ Google Scholar]
- Huarcaya-Victoria J, Podestá A, Rojas W. Factors associated with distress among medical staff during the initial phase of the COVID-19 pandemic in Peru. Int J Ment Health Addict 2023; 21(5):3473-82. doi: 10.1007/s11469-022-00804-2 [Crossref] [ Google Scholar]
- Khoo EM, Abdullah A, Liew SM, Hussein N, Hanafi NS, Lee PY. Psychological health and wellbeing of primary healthcare workers during COVID-19 pandemic in Malaysia: a longitudinal qualitative study. BMC Prim Care 2022; 23(1):261. doi: 10.1186/s12875-022-01870-0 [Crossref] [ Google Scholar]
- Alfaifi A, Darraj A, El-Setouhy M. The psychological impact of quarantine during the COVID-19 pandemic on quarantined non-healthcare workers, quarantined healthcare workers, and medical staff at the quarantine facility in Saudi Arabia. Psychol Res Behav Manag 2022; 15:1259-70. doi: 10.2147/prbm.S362712 [Crossref] [ Google Scholar]
- Alnahdi OS, Albuqaytah FA, Alotaibi N, Afeef MA, Natto ZS, Subahi RH. COVID-19 stigma correlates with burnout among healthcare workers: evidence from healthcare workers practicing in Saudi Arabia. Saudi J Health Syst Res 2023; 3(1-4):85-92. doi: 10.1159/000528564 [Crossref] [ Google Scholar]
- Soubra K, Tamworth C, Kamal Z, Brook C, Langdon D, Billings J. Health and social care workers experiences of coping while working in the frontline during the COVID-19 pandemic: one year on. PLoS One 2023; 18(4):e0284306. doi: 10.1371/journal.pone.0284306 [Crossref] [ Google Scholar]
- Al Mutair A, Woodman A, Al Hassawi AI, Ambani Z, Al Bazroun MI, Alahmed FS. Healthcare providers as patients: COVID-19 experience. PLoS One 2023; 18(8):e0289131. doi: 10.1371/journal.pone.0289131 [Crossref] [ Google Scholar]
- Hossain I, Mehedi N, Ali I, Azman A. Occupational health of frontline workers during the COVID-19 pandemic: is health and well-being an issue in Bangladesh?. Rev Cercet Interv Soc 2023; 80(1):18-39. doi: 10.33788/rcis.80.2 [Crossref] [ Google Scholar]
- Kealeboga KM, Ntsayagae EI, Tsima O. Psychological impact of COVID-19 on nurses caring for patients during COVID-19 pandemic in Gaborone. Nurs Open 2023; 10(5):3084-93. doi: 10.1002/nop2.1557 [Crossref] [ Google Scholar]
- Turki M, Ouali R, Ellouze S, Ben Ayed H, Charfi R, Feki H. Perceived stigma among Tunisian healthcare workers during the COVID-19 pandemic. Encephale 2023; 49(6):582-8. doi: 10.1016/j.encep.2022.08.014 [Crossref] [ Google Scholar]
- Mediavilla R, Fernández-Jiménez E, Andreo J, Morán-Sánchez I, Muñoz-Sanjosé A, Moreno-Küstner B. Association between perceived discrimination and mental health outcomes among health workers during the initial COVID-19 outbreak. Span J Psychiatry Ment Health 2023; 16(4):221-4. doi: 10.1016/j.rpsm.2021.06.001 [Crossref] [ Google Scholar]
- Alajmi AF, Al-Olimat HS, Abu Ghaboush R, Al Buniaian NA. Social avoidance and stigma among healthcare workers serving COVID-19 patients in Saudi Arabia. Sage Open 2022; 12(2):21582440221095845. doi: 10.1177/21582440221095845 [Crossref] [ Google Scholar]
- Almomani MH, Khater WA, Akhu-Zaheya LM, Alloubani A, AlAshram SA, Azab M. Nurses’ experiences of caring for patients with COVID-19: a qualitative study. Sage Open 2022; 12(4):21582440221144982. doi: 10.1177/21582440221144982 [Crossref] [ Google Scholar]
- Yufika A, Pratama R, Anwar S, Winardi W, Librianty N, Prashanti NAP. Stigma associated with COVID-19 among health care workers in Indonesia. Disaster Med Public Health Prep 2022; 16(5):1942-6. doi: 10.1017/dmp.2021.93 [Crossref] [ Google Scholar]
- Jeleff M, Traugott M, Jirovsky-Platter E, Jordakieva G, Kutalek R. Occupational challenges of healthcare workers during the COVID-19 pandemic: a qualitative study. BMJ Open 2022; 12(3):e054516. doi: 10.1136/bmjopen-2021-054516 [Crossref] [ Google Scholar]
- Tsukuda M, Kayano T, Ito Y. Experiences of COVID-19-related stigma: a qualitative study on nurses caring for patients with COVID-19. J Nurs Res 2022; 30(6):e241. doi: 10.1097/jnr.0000000000000528 [Crossref] [ Google Scholar]
- Sachdeva A, Nandini H, Kumar V, Chawla RK, Chopra K. From stress to stigma - mental health considerations of health care workers involved in COVID19 management. Indian J Tuberc 2022; 69(4):590-5. doi: 10.1016/j.ijtb.2021.09.007 [Crossref] [ Google Scholar]
- O’Regan-Hyde M, Dalton-O Connor C, Flynn A, Murphy A, McCarthy VJ. Nurses’ experiences of the caring role during the COVID-19 pandemic: a scoping review of qualitative research. J Nurs Manag 2024; 2024:7147203. doi: 10.1155/2024/7147203 [Crossref] [ Google Scholar]
- Shetty AP, Mishra S, Radhakrishnan RV, Venkatesan M, Renjith V. Experience of nurses in caring for patients with COVID-19: a descriptive qualitative study. Clin Epidemiol Glob Health 2024; 28:101696. doi: 10.1016/j.cegh.2024.101696 [Crossref] [ Google Scholar]
- Marpaung YM. Stigma in the prolonged pandemic: insights from nurses in two Indonesian provinces. Open Public Health J 2024; 17(1):e18749445292650. doi: 10.2174/0118749445292650240312041029 [Crossref] [ Google Scholar]
- Ali HA, Gaber MA, Attia NM. COVID-19 social stigma and nurse’s role efficacy. Zagazig Nurs J 2024; 20(1):391-405. doi: 10.21608/znj.2024.353286 [Crossref] [ Google Scholar]
- Negarandeh R, Shahmari M, Zare L. Stigmatization experiences of healthcare workers in the context of the COVID-19 pandemic: a scoping review. BMC Health Serv Res 2024; 24(1):823. doi: 10.1186/s12913-024-11300-9 [Crossref] [ Google Scholar]
- Stevenson A. Oxford Dictionary of English. Oxford: Oxford University Press; 2010.
- Ayuthaya AI. The implications of stigma to heath communication. J Commun Arts 2019; 9(2):1-16. [ Google Scholar]
- Link BG, Phelan JC. Conceptualizing stigma. Annu Rev Sociol 2001; 27(1):363-85. doi: 10.1146/annurev.soc.27.1.363 [Crossref] [ Google Scholar]
- Corrigan PW. Mental health stigma as social attribution: implications for research methods and attitude change. Clin Psychol (New York) 2000; 7(1):48-67. [ Google Scholar]
- Seo K, Song Y. Self-stigma among Korean patients with diabetes: a concept analysis. J Clin Nurs 2019; 28(9-10):1794-807. doi: 10.1111/jocn.14789 [Crossref] [ Google Scholar]
- Fowler HW, Fowler FG. The Concise Oxford Dictionary of Current English. Clarendon Press; 1926.
- de Hooge IE, Breugelmans SM, Wagemans FM, Zeelenberg M. The social side of shame: approach versus withdrawal. Cogn Emot 2018; 32(8):1671-7. doi: 10.1080/02699931.2017.1422696 [Crossref] [ Google Scholar]
- Jones AC. Stigma and shame: conceptualisations and views concerning service use and health care provision: a literature review and commentary. J Clin Med Res 2019; 2019(1):1-16. [ Google Scholar]
- Corrigan PW, Rafacz J, Rüsch N. Examining a progressive model of self-stigma and its impact on people with serious mental illness. Psychiatry Res 2011; 189(3):339-43. doi: 10.1016/j.psychres.2011.05.024 [Crossref] [ Google Scholar]
- Parker R. Stigma, prejudice and discrimination in global public health. Cad Saude Publica 2012; 28(1):164-9. doi: 10.1590/s0102-311x2012000100017 [Crossref] [ Google Scholar]
- Fibbi R, Midtbøen AH, Simon P. Concepts of discrimination. In: Migration and Discrimination: IMISCOE Short Reader. Cham: Springer International Publishing; 2021. p. 13-20. 10.1007/978-3-030-67281-2_2
- Ackerman JM, Hill SE, Murray DR. The behavioral immune system: current concerns and future directions. Soc Personal Psychol Compass 2018; 12(2):e12371. doi: 10.1111/spc3.12371 [Crossref] [ Google Scholar]
- Jecker NS, Takahashi S. Shaming and stigmatizing healthcare workers in Japan during the COVID-19 pandemic. Public Health Ethics 2021; 14(1):72-8. doi: 10.1093/phe/phab003 [Crossref] [ Google Scholar]
- Spring H. Health literacy and COVID‐19. Health Info Libr J 2020; 37(3):171-2. doi: 10.1111/hir.12322 [Crossref] [ Google Scholar]
- Paakkari L, Okan O. COVID-19: health literacy is an underestimated problem. Lancet Public Health 2020; 5(5):e249-50. doi: 10.1016/s2468-2667(20)30086-4 [Crossref] [ Google Scholar]
- Hurst SK, Dotson JA, Butterfield P, Corbett CF, Oneal G. Stigma resulting from head lice infestation: a concept analysis and implications for public health. Nurs Forum 2020; 55(2):252-8. doi: 10.1111/nuf.12423 [Crossref] [ Google Scholar]
- Martínez-Lorca M, Martínez-Lorca A, Criado-Álvarez JJ, Armesilla MDC, Latorre JM. The fear of COVID-19 scale: validation in Spanish university students. Psychiatry Res 2020; 293:113350. doi: 10.1016/j.psychres.2020.113350 [Crossref] [ Google Scholar]
- Fitzpatrick KM, Harris C, Drawve G. Fear of COVID-19 and the mental health consequences in America. Psychol Trauma 2020; 12(S1):S17-21. doi: 10.1037/tra0000924 [Crossref] [ Google Scholar]
- Schimmenti A, Billieux J, Starcevic V. The four horsemen of fear: an integrated model of understanding fear experiences during the COVID-19 pandemic. Clin Neuropsychiatry 2020; 17(2):41-5. doi: 10.36131/cn20200202 [Crossref] [ Google Scholar]
- Solomon DH, Bucala R, Kaplan MJ, Nigrovic PA. The “infodemic” of COVID-19. Arthritis Rheumatol 2020; 72(11):1806-8. doi: 10.1002/art.41468 [Crossref] [ Google Scholar]
- Abuhammad S, AlAzzam M, Mukattash T. The perception of nurses towards their roles during the COVID-19 pandemic. Int J Clin Pract 2021; 75(4):e13919. doi: 10.1111/ijcp.13919 [Crossref] [ Google Scholar]
- Nursalam N, Sukartini T, Priyantini D, Mafula D, Efendi F. Risk factors for psychological impact and social stigma among people facing COVID 19: a systematic review. Syst Rev Pharm 2020; 11(6):1022-8. [ Google Scholar]
- Yakeley J. Shame, culture and mental health. Nord J Psychiatry 2018; 72(sup1):S20-s2. doi: 10.1080/08039488.2018.1525641 [Crossref] [ Google Scholar]
- Kollareth D, Fernandez-Dols JM, Russell JA. Shame as a culture-specific emotion concept. J Cogn Cult 2018; 18(3-4):274-92. doi: 10.1163/15685373-12340031 [Crossref] [ Google Scholar]
- Piers EV. Piers-Harris Children’s Self-Concept Scale. Los Angeles, CA: Western Psychological Services; 2002.
- González-Valero G, Zurita-Ortega F, Lindell-Postigo D, Conde-Pipó J, Grosz WR, Badicu G. Analysis of self-concept in adolescents before and during COVID-19 lockdown: differences by gender and sports activity. Sustainability 2020; 12(18):7792. doi: 10.3390/SU12187792 [Crossref] [ Google Scholar]
- Catalano LT, Brown CH, Lucksted A, Hack SM, Drapalski AL. Support for the social-cognitive model of internalized stigma in serious mental illness. J Psychiatr Res 2021; 137:41-7. doi: 10.1016/j.jpsychires.2021.02.014 [Crossref] [ Google Scholar]
- Janoušková M, Pekara J, Kučera M, Kearns PB, Šeblová J, Wolfová K. Experiences of stigma, discrimination and violence and their impact on the mental health of health care workers during the COVID-19 pandemic. Sci Rep 2024; 14(1):10534. doi: 10.1038/s41598-024-59700-5 [Crossref] [ Google Scholar]
- Badrfam R, Zandifar A. Stigma over COVID- 19; new conception beyond individual sense. Arch Med Res 2020; 51(6):593-4. doi: 10.1016/j.arcmed.2020.05.006 [Crossref] [ Google Scholar]
- Villa S, Jaramillo E, Mangioni D, Bandera A, Gori A, Raviglione MC. Stigma at the time of the COVID-19 pandemic. Clin Microbiol Infect 2020; 26(11):1450-2. doi: 10.1016/j.cmi.2020.08.001 [Crossref] [ Google Scholar]
- Khatooni M. Stigma in the context of COVID-19 crisis: an evolutionary concept analysis. Prof Case Manag 2022; 28(1):20-32. doi: 10.1097/ncm.0000000000000573 [Crossref] [ Google Scholar]
- Sun Y, Bao Y, Ravindran A, Sun Y, Shi J, Lu L. Mental health challenges raised by rapid socioeconomic transformations in China: lessons learned and prevention strategies. Heart Mind 2020; 4(3):59-66. doi: 10.4103/hm.hm_22_20 [Crossref] [ Google Scholar]
- Li JQ, Wang YH, Lu QD, Xu YY, Shi J, Lu L. Prevalence of psychological distress in type ii diabetes in China: a systematic review and meta-analysis. Heart Mind 2019; 3(4):147-52. doi: 10.4103/hm.hm_67_19 [Crossref] [ Google Scholar]
- Abiri S, Oakley LD, Hitchcock ME, Hall A. Stigma related avoidance in people living with severe mental illness (SMI): findings of an integrative review. Community Ment Health J 2016; 52(3):251-61. doi: 10.1007/s10597-015-9957-2 [Crossref] [ Google Scholar]
- Carrara BS, Fernandes RH, Bobbili SJ, Ventura CA. Health care providers and people with mental illness: an integrative review on anti-stigma interventions. Int J Soc Psychiatry 2021; 67(7):840-53. doi: 10.1177/0020764020985891 [Crossref] [ Google Scholar]
- Knaak S, Mantler E, Szeto A. Mental illness-related stigma in healthcare: barriers to access and care and evidence-based solutions. Healthc Manage Forum 2017; 30(2):111-6. doi: 10.1177/0840470416679413 [Crossref] [ Google Scholar]
- Lawson TG. Betty Neuman: systems model. In: Alligood MR, ed. Nursing Theorists and Their Work. Mosby; 2021. p. 231-46.