Journal of caring sciences. 14(4):251-258.
doi: 10.34172/jcs.025.33581
Original Article
Prediction of Mortality in Iranian Elderly Using Frailty Index
Mehdi Norouzi Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Visualization, Writing – original draft, 1 
Zahra Amiri Data curation, Formal analysis, Investigation, Project administration, Writing – original draft, 1
Mohammad Hossein Madahali Data curation, Validation, 2
Ehsan Mosafarkhani Data curation, Funding acquisition, Methodology, Project administration, Resources, Supervision, Validation, Writing – review & editing, 3, *
Author information:
1Department of Epidemiology, School of Health, Mashhad University of Medical Sciences, Mashhad, Iran
2Department of Anatomical Sciences and Cell Biology, Mashhad University of Medical Sciences, Mashhad, Iran
3Department of Epidemiology, School of Health, Social Determinants of Health Research Center, Mashhad University of Medical Sciences, Mashhad, Iran
Abstract
Introduction:
Frailty in older adults can lead to severe outcomes such as early death, loss of function, and mental health issues. This study aims to predict mortality rates in elderly Iranians using the Frailty Index.
Methods:
This retrospective cohort study analyzed data from the Sina healthcare system, focusing on individuals aged 60 and above residing in nursing homes from 2020 to 2023. A total of 3554 elderly individuals were included, with frailty assessed using Fried’s scale. Data analysis was performed using Python 3.12, utilizing Kaplan-Meier survival analysis, log-rank tests, and Cox regression models to evaluate survival rates and the impact of frailty on mortality.
Results:
Of the 3,554 individuals assessed, 1,830 (51.50%) were identified as frail, and 36.50% of the total participants died during the follow-up period. The cumulative survival rates for frail individuals at 365,730, and 920 days were 0.62, 0.47, and 0.46, respectively, which were lower than those classified as healthy. Multivariable Cox regression analysis showed that frail individuals had a 2.04 times higher risk of mortality compared to healthy individuals, adjusting for confounding variables. Significant factors associated with increased mortality included being female, age over 70, and presence of co-morbidities, while literacy was identified as a protective factor.
Conclusion:
Frailty is strongly associated with increased mortality risk in the elderly. The frailty index is an effective predictor of mortality, highlighting the need for early identification and management of frailty to improve health outcomes in this population.
Keywords: Frailty index, Elderly, Mortality
Copyright and License Information
© 2025 The Author(s).
This work is published by Journal of Caring Sciences as an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/). Non-commercial uses of the work are permitted, provided the original work is properly cited.
Funding Statement
The financial support for this research endeavor was provided by Mashhad University of Medical Sciences (Grant No. 4021225).
Introduction
Old age is often considered the final phase of the human life cycle, but defining it precisely can be challenging due to the varying physical and psychological experiences individuals go through. The perception of old age differs across cultures, with some societies considering individuals as adults at a specific age while others do not. Additionally, the onset of old age is closely linked to a country’s life expectancy. For example, countries like Japan, where the life expectancy was 81 years, may have a different perspective on old age compared to countries like Iraq, where the life expectancy was 67 years.1,2 The concept of old age is subjective and changes over time and across different societies.3 In Iran, some demographic studies consider the age of 65 years and in others, 60 years as old age.4
The global population of elderly individuals is steadily increasing. Currently, 13% of the world’s population is over 65 years old, and this number is expected to rise to 20% by 2050.5,6 There are approximately 703 million individuals worldwide aged over 65, a figure projected to exceed two billion by 2050.7 Regions like North Africa and West Asia are anticipated to experience rapid growth in their elderly populations, with numbers expected to increase from 29 million in 2019 to 96 million in 2050.8
In Iran, the proportion of elderly population will increase significantly in the period from 2030 to 2050. Iran has witnessed a gradual rise in the number of people aged 60 and above, growing from 1.4 million in 1956 to almost 7 million in 2016. Population forecasts suggest that by 2035, Iran will have around 7.4 million individuals aged 60 and over, increasing to 33.4 million by 2056.9 Additionally, the number of individuals aged 65 and above is predicted to rise from 5 million to 23 million during this period. Over the course of a century from 1956 to 2056, the population of elderly individuals in the country is expected to increase significantly, from less than 10% of the population in 2016 to approximately 32% by 2056. Moreover, the percentage of individuals aged 65 and older is projected to rise from 6% in 2016 to 22% in 2056.9,10
Studies suggest that 80% of individuals aged 65 and older suffer from at least one chronic illness, with disorders in this age group contributing to 23% of the overall disease burden.11 Factors such as smoking, a sedentary lifestyle, a diet high in saturated fats, alcohol or drug use, lack of mental health prevention, poor oral hygiene, and high blood pressure are key contributors to these diseases,12,13 accounting for 86% of the disease burden risk and 11% of the total disease burden in Iran, corresponding to approximately 1.6 million years of disabled life.3,14
The aging process is associated with physiological changes such as alterations in body composition and loss of bone and muscle mass, which can lead to decreased mobility, falls, disability, frailty syndrome, hospitalizations, and an increased risk of mortality. Fatigue and tiredness have also emerged as significant concerns among the elderly. Frailty, characterized by symptoms like unexplained weight loss, weakness, fatigue, slow walking speed, and low body mass, is a common condition among the elderly population.15 Frailty has been linked to various factors including visual impairment, chronic heart failure, advanced age, female gender, poor nutrition, comorbid conditions, falls, kidney issues, weight fluctuations, physical inactivity, depression, living alone, and smoking. This complex interplay of factors may contribute to both the development of frailty and an increased risk of mortality.16-19Studies on frailty and mortality are well-documented globally; however, there is limited data specific to Iran and other Middle Eastern populations.20,21 Existing studies have reported frailty prevalence rates of 4.33% and 4.10%in some cities of Iran, such as Ardabil and Khuzestan provinces.22,23These findings highlight the need for region-specific research to explore frailty and its outcomes in diverse cultural and healthcare settings.
Aging in the Iranian population has progressed differently compared to Western countries, particularly prior to Iran’s socioeconomic development. This unique demographic transition necessitates country-specific approaches to understanding and managing the challenges of aging. Frailty, a condition extensively studied in relation to mortality, presents prevalence rates ranging from 30% to 70% in affected individuals globally.10However, there remains a significant gap in large-scale research on frailty in Iran. Addressing this gap, this study is the first to utilize the Frailty Index in a large cohort of Iranian elderly to predict mortality. By integrating data from a national registry and electronic health records, our research explores the interplay of frailty with cultural, dietary, and healthcare-specific factors unique to Iran. Furthermore, the findings provide critical insights into frailty and mortality during the COVID-19 pandemic, emphasizing the importance of early identification of frailty to delay or prevent adverse outcomes. This study aims to predict mortality rates in elderly Iranians using the Frailty Index.
Materials and Methods
This retrospective cohort study utilized data extracted from the Sina Electronic Health Record System (SinaEHR®, Iran)24and the national registry for registration and classification of causes of death in Iran.25 SinaEHR is an integrated health information system supervised by Mashhad University of Medical Sciences, which contains the health records of more than five million people in Khorasan Razavi province, Iran. The study population encompassed all nursing home facilities across the country under the jurisdiction of the Ministry of Health and Medical Education of Iran.
The study population comprised all 9,199 elderly adults aged ≥ 60 years who had a complete frailty assessment during the period between April 2021 and June 2022. All information, including frailty scores, demographic variables, and mortality outcomes, was extracted from these databases, and no direct contact or additional data collection from nursing home residents was performed.
Frailty assessments were conducted using the well-established 5-item Fried frailty phenotype,1 performed by trained personnel from the national social services agency between April 2021 and June 2022. This phenotype identifies frailty based on five criteria:
Unintentional weight loss: A loss of more than 4.50 kg or 5% of body weight in the past year.
Exhaustion: Assessed through responses to standardized questions regarding fatigue and energy levels.
Weakness: Measured using grip strength, adjusted for sex and body mass index.
Slowness: Evaluated based on walking speed over a standardized distance, adjusted for sex and height.
Low physical activity: Determined through self-reported levels of physical activity compared to normative data.
Each criterion was scored as 1 (present) or 0 (absent), resulting in an overall score ranging from 0 to 5. Scores were classified as follows: 0: Robust (healthy status), 1–2: Pre-frail and 3–5: Frail. This frailty assessment tool has been extensively validated and demonstrated good reliability across diverse populations.1
Frailty data up until August 2022 were extracted from the centralized databases. Mortality data, including time of death, were obtained from the national death registry. Other variables like demographics and comorbidities were also obtained from the Sina Electronic Health Record System. The subjects were categorized into frail (scores > 3, n = 3,556) and non-frail (scores ≤ 3, n = 5,643) groups based on the frailty assessment scores.
The Kaplan-Meier method was used to estimate survival rates, and the log-rank test was employed to compare survival distributions between the frail and non-frail groups. Cox proportional hazards regression analysis was conducted to determine the adjusted hazard ratios (HRs) and 95% confidence intervals (CIs) for factors associated with mortality, including frailty status, age, sex, and comorbidities. In this study, an “event” refers to death, while “censorship” applies to participants who were alive at the study’s end or lost to follow-up. Right-censoring was used to account for incomplete survival data. The proportional hazards assumption was tested using Schoenfeld residuals, visual inspection of log-minus-log survival plots, and time-dependent covariates analysis. The results confirmed the validity of the Cox proportional hazards regression model for our data. Data analysis was conducted using Python (version 3.12) with the following packages: pandas for data manipulation, NumPy for numerical computations, SciPy for statistical testing, lifelines for survival analysis (e.g., Kaplan-Meier and Cox regression), and matplotlib and seaborn for data visualization. Statistical significance was set at P < 0.05.
Results
Table 1 presents the demographic characteristics and frailty index of the participants stratified by mortality status. Out of the total 9,199 participants, 3,354 (36.50%) individuals experienced death during the follow-up period. The analysis revealed that 1,830 (51.50%) of the 3,556 frail individuals passed away, while the mortality rate was lower among non-frail individuals. Differences in mortality rates were observed across various subgroups. The mortality rate was higher among women (37.30%) compared to men (35.30%), although this difference was not statistically significant. Older age was associated with increased mortality, with the highest rate observed in individuals aged 90 years and above (55.50%); however, the difference across age groups was not statistically significant. Unmarried individuals had a higher mortality rate compared to married individuals. The presence of chronic comorbidities was also significantly associated with increased mortality, while literacy was identified as protective factor, all observed differences were statistically significant.
Survival Analysis
The cumulative survival probability declined over time, as shown in Table 2. At 200 days, the survival probability was 0.83 (95% CI: 0.82–0.83), decreasing to 0.62 (95% CI: 0.61–0.62) by 800 days. Censorship also increased with time, reflecting participants lost to follow-up or still alive. As presented in Table 3, frail individuals had markedly lower cumulative survival rates at 365, 730, and 920 days compared to non-frail participants. Figures 1 and 2 illustrate the survival probability by frailty status, showing that frail individuals had a significantly lower survival rate than non-frail participants, highlighting the strong impact of frailty on mortality risk.
The impact of frailty on survival was further examined using Cox proportional hazards regression analysis. Table 4 shows the results of both univariate and multivariate Cox regression analyses. In the univariate analysis, frailty was associated with a HR of 2.31 (95% CI: 2.15-2.47) for mortality. After adjusting for potential confounders in the multivariate model, frailty remained a significant predictor of mortality, with an HR of 2.04 (95% CI: 1.90-2.19).
Other significant predictors of mortality identified in the multivariate analysis included advanced age, female gender, and the presence of chronic comorbidities. Compared to the reference group (age 60-69 years), the HRs for mortality were 1.76 (95% CI: 1.55-2.04) for age 70-79 years, 2.48 (95% CI: 2.19-2.48) for age 80-89 years, and 3.56 (95% CI: 3.14-4.04) for age 90 years and above. Females had a higher risk of mortality (HR: 1.30, 95% CI: 1.02-1.40) compared to males. The presence of one chronic disease (HR: 1.30, 95% CI: 1.15-1.47) and two or more chronic diseases (HR: 1.47, 95% CI: 1.16-1.87) were also associated with increased mortality risk compared to individuals without chronic diseases. Notably, being literate was identified as a protective factor, with a lower risk of mortality (HR: 0.86, 95% CI: 0.77-0.95) compared to illiterate individuals.
Table 1.
Demographic characteristics and fertility index in deceased and living people
|
Variable
|
Occurrence of death
|
No death
|
Total
|
P
value
|
| Death |
3354 (36.50) |
5845 (63.50) |
9199 |
|
| Frailty |
|
|
|
|
| Frailty |
1830 (51.50) |
1726 (48.50) |
3556 |
< 0.001 |
| Healthy |
1524 (27) |
4119 (73) |
5643 |
| Sex |
|
|
|
|
| Man |
1297 (35.30) |
2380 (64.70) |
3677 |
0.054 |
| Woman |
2057 (37.30) |
3465 (62.70) |
5522 |
| Age |
|
|
|
|
| 60-69 |
336 (17.90) |
1542 (82.10) |
1878 |
< 0.001 |
| 70-79 |
765 (30) |
1783 (70) |
2548 |
| 80-89 |
1187 (41.60) |
1665 (58.40) |
2852 |
| 90 and more |
1066 (55.50) |
855 (45.50) |
1921 |
| Education |
|
|
|
|
| Literate |
2972 (36.06) |
5270 (63.94) |
8242 |
< 0.01 |
| Illiterate |
382 (39.92) |
575 (60.08) |
957 |
| Marital status |
|
|
|
|
| Married (with wife) |
53 (38.41) |
85 (61.59) |
138 |
0.63 |
| Single |
3301 (36.43) |
5760 (63.57) |
9061 |
| Chronic comorbidity |
| Not have |
2995 (35.50) |
5444 (64.50) |
8439 |
0.001 |
| 1 disease |
290 (46.20) |
338 (53.80) |
628 |
| 2 diseases |
69 (52.30) |
63 (47.70) |
132 |
Discussion
Based on the results of multivariable regression analysis and after adjusting the effect of other variables under study (by removing the effect of possible confounding variables), the effect of the Frailty variable remains significant. Also, other variables such as age, gender, co-morbidities and qualifications were also significant after adjustment of other variables. In the present study, frailty significantly predicted mortality, with frail individuals showing a twofold higher risk compared to non-frail individuals (HR: 2.04, 95% CI: 1.90–2.19, P < 0.001). Gender differences were observed, as females had a higher mortality risk compared to males (HR: 1.04, 95% CI: 0.69–1.80, P = 0.001). Additionally, the presence of multimorbidity significantly increased mortality risk. Participants with two or more chronic diseases had a 47% higher risk of mortality than those without comorbidities (HR: 1.47, 95% CI: 1.16–1.87, P < 0.001). Various studies have reported that frailty is associated with various factors such as visual impairment, chronic heart failure, age, female gender, nutrition, co-morbidities, falls, kidney problems, weight, inactivity, depression, living alone, smoking, BMI. It is related that all these factors can be a reason for the relationship between frailty and mortality.19,26-28 The survival rates of 365 days, 730 days and 920 days were 0.74, 0.62 and 0.61, respectively. In the first 365 days, survival has decreased significantly. The reason for this could be the decreasing slope of survival in frailty people, as seen in the survival curve 2-4, survival in frailty people decreases sharply and reaches 0.66 at the end of 365 days. Also, this data Studies have been collected during the corona pandemic, which studies have reported that mortality due to corona is related to frailty.29Data collection during the COVID-19 pandemic likely amplified frailty-related mortality due to heightened vulnerability among elderly individuals. Frailty has been shown to exacerbate outcomes of respiratory infections, further supporting the observed trends.30
Aging is associated with the continuous accumulation of damage and deterioration at the level of cells, tissues, organs or organisms, which ultimately leads to death. In the present study, with the increase in survival age, the survival rate decreases and the risk of death increases, so that the risk in the age group of 90 years and older is 4.02 in the univariate model and 3.56 in the multivariate model. The results of various studies show that there is a statistically significant relationship between age and frailty, and older age is associated with more frailty. With increasing age, changes in various systems occur due to the interaction of physiological mechanisms and pathological conditions caused by aging is associated with conditions such as increased incidence of chronic diseases, depression symptoms, decreased cognitive and functional capacity, which leads to the acceleration of the frailty process. Frailty can be one of the causes of death at older ages.31-33 The present study showed that the number of frail individuals increased with advancing age, and this relationship was statistically significant. Overall, age was identified as a strong predictor of mortality.
In the present study, the survival rate among women was slightly lower than that of men, and the risk of death in women was significantly higher. This contrasts with some studies from Western populations, where women typically have lower mortality rates despite higher frailty prevalence.34,35 However, women in this study showed greater risk, possibly due to physiological and cultural factors. Post-menopausal hormonal changes, such as reduced estrogen levels, may accelerate muscle mass loss and increase susceptibility to chronic diseases, contributing to higher frailty and mortality. Additionally, the prevalence of obesity, which was higher in women than men in this study, is known to exacerbate frailty-related outcomes.36,37 The participants in this study were in the older age group, where the cumulative effects of aging and chronic disease burden are more pronounced. In Iran, cultural and healthcare differences may also play a role. Limited access to gender-specific healthcare resources, combined with societal factors such as caregiving responsibilities and reduced physical activity in elderly women, could further elevate mortality risks. These findings highlight the need for targeted interventions to address gender disparities in frailty and mortality in elderly populations.38
Although life expectancy has increased due to advancements in modern medicine, chronic diseases have become more prevalent, leading to a rise in multimorbidity among the elderly.39 Studies report that 55%–98% of individuals over 65 have multiple chronic conditions.40 The present study found a significant relationship between frailty and multimorbidity, with individuals having two or more chronic diseases experiencing a 1.78-fold higher risk of mortality compared to those without chronic conditions.
Frailty and multimorbidity interact synergistically, further accelerating mortality risk. Chronic diseases impair physiological reserves, while frailty exacerbates these effects, leading to worse outcomes. This dose-response relationship has been observed in elderly nursing home patients, where the combination of disability and comorbidity significantly increased mortality, independent of age and gender.41-43 The prevalence of cardiovascular, pulmonary, and inflammatory diseases increases with age and represents the leading causes of death in individuals over 65.44For instance, Arshadipour and colleagues’ study reported that having both cancer and another chronic disease increased mortality risk by 66%.45 These findings emphasize the importance of addressing multimorbidity and frailty together to reduce mortality in elderly populations.
Evidence shows that the level of education is a protective factor against adverse effects on the health of elderly people. Lower education levels are associated with mental health issues, chronic conditions, and limited access to healthcare, while higher education improves health knowledge, disease management, and access to resources.46,47 In our study, individuals without formal education had higher mortality risks. Education likely mitigates frailty’s impact by fostering health literacy and preventive behaviors, highlighting its importance as a strategy to reduce mortality and improve health outcomes in aging populations.48
This study has several limitations. First, the COVID-19 pandemic may have influenced mortality rates and frailty assessments. Second, frailty assessments relied on self-reported data, which could introduce bias. Finally, potential confounders such as socioeconomic status and diet were not included in the analysis.
This study has important implications for clinical practice, education, and public health. Clinically, early frailty identification can guide interventions to reduce mortality. Training healthcare professionals to recognize frailty and incorporating frailty awareness into public health campaigns can further improve elderly care.
Table 2.
Cumulative survival rates over time
|
Survival time
|
Death (Cumulative)
|
Censorship
*
|
Probability of survival
|
95% confidence interval for survival
|
| 200 days |
1502 |
8 |
0.83 |
0.82 - 0.83 |
| 400 days |
2448 |
38 |
0.73 |
0.72 - 0.73 |
| 600 days |
3114 |
310 |
0.65 |
0.64 - 0.66 |
| 800 days |
3354 |
1746 |
0.62 |
0.61- 0.62 |
*Censorship refers to participants who were alive at the end of the study period or lost to follow-up before experiencing the event (death).
Table 3.
Cumulative survival rate in risk groups
|
Group/Time
|
365 days
|
730 days
|
920 days
|
|
Cumulative Survival
|
95% CI
|
Cumulative Survival
|
95% CI
|
Cumulative Survival
|
95% CI
|
| Health |
0.82 |
0.81-0.83 |
0.72 |
0.70-0.72 |
0.71 |
0.70-0.72 |
| Frailty |
0.62 |
0.61-0.64 |
0.47 |
0.45-0.48 |
0.46 |
0.44-0.48 |
Table 4.
Fit of univariate Cox and Multiple cox models
|
Variable
|
Univariate analysis
|
Multivariate analysis
|
|
HR
|
Significance level
|
95% CI for HR
|
HR
|
Significance level
|
95% CI for HR
|
| Frailty |
2.31 |
0.0005 |
2.15-2.47 |
2.04 |
0.001 |
1.90 - 2.199 |
| Sex |
1.05 |
0.13 |
0.98-1.13 |
1.30 |
0.001 |
1.20-1.04 |
| Education |
0.88 |
0.02 |
0.75-0.98 |
0.86 |
0.007 |
0.77-0.95 |
| Age 70-79 |
1.8 |
0.001 |
1.59-2.05 |
1.76 |
0.001 |
1.55-2.04 |
| Age 80-89 |
2.73 |
0.001 |
2.41-3.08 |
2.48 |
0.001 |
2.19-2.48 |
| Age 90 and more |
4.02 |
0.001 |
3.55-4.54 |
3.56 |
0.001 |
3.14-4.04 |
| Comorbidity |
1.44 |
0.001 |
1.28-1.62 |
1.30 |
0.001 |
1.15-1.47 |
| Two diseases etc. |
1.78 |
0.001 |
1.40-2.24 |
1.47 |
0.001 |
1.16-1.87 |
CI: Confidence interval; HR: hazard ratio.
*Reference levels: Frailty (robust/healthy status), Sex (male), Education (illiterate), Age (60-69 years), Comorbidity (no disease).
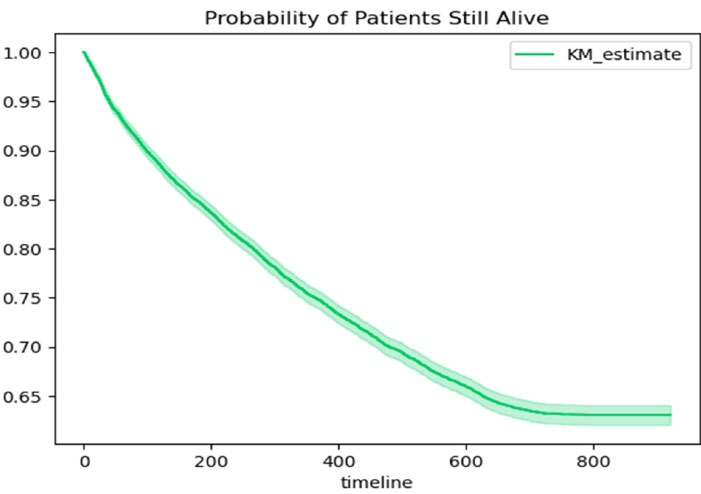
Figure 1.
Cumulative survival and censoring in elderly participants over time
.
Cumulative survival and censoring in elderly participants over time
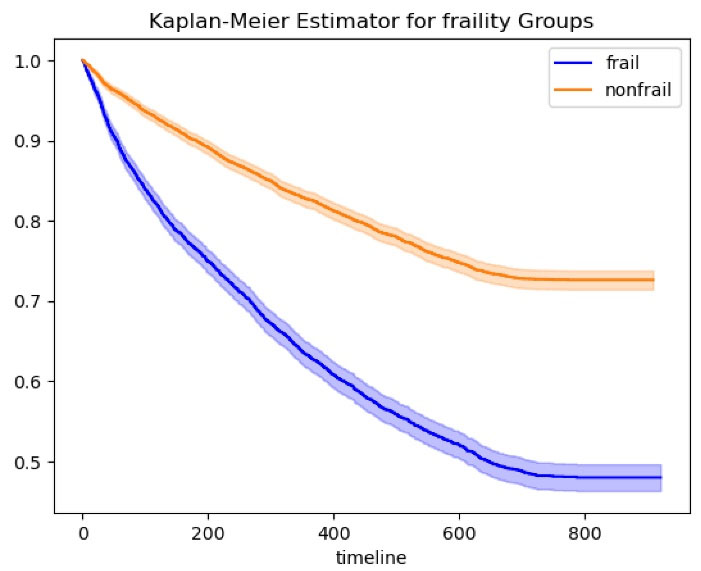
Figure 2.
Cumulative survival rates in frail vs. non-frail groups
.
Cumulative survival rates in frail vs. non-frail groups
Conclusion
Frailty remained a significant predictor of mortality even after adjustment for confounding variables, underscoring its strong association with adverse outcomes in older adults. The frailty index proved to be an effective predictor of mortality, emphasizing the importance of its early identification and management in clinical and community settings. Integrating frailty screening into geriatric care can guide preventive interventions, optimize resource allocation, and improve survival outcomes among the elderly.
Although life expectancy has increased due to medical advancements, the growing burden of chronic diseases and multimorbidity highlights the need for comprehensive approaches addressing frailty. Promoting health literacy, physical activity, and balanced nutrition may mitigate frailty-related risks. These findings emphasize the importance of incorporating frailty assessment into elderly care programs and developing targeted interventions to improve quality of life and reduce mortality in Iran’s aging population.
Future research should focus on designing and evaluating interventions that target frailty in different elderly subgroups. Studies exploring the influence of lifestyle, comorbidity management, and psychosocial factors on frailty progression and mortality would further enhance understanding of this critical health determinant.
Competing Interests
The authors declared no conflict of interest.
Data Availability Statement
The datasets are available from the corresponding author on reasonable request.
Ethical Approval
The present study received ethical approval from the Ethics Committee of Mashhad University of Medical Sciences (Code: IR.MUMS.FHMPM.REC.1402.195).
Research Highlights
What is the current knowledge?
-
Frailty in older adults is associated with adverse outcomes such as early death, loss of function, and mental health issues.
-
Frailty prevalence in older adults worldwide is estimated between 10% and 20%, but precise data for Iranian older adults is limited.
-
Frailty has been extensively studied in relation to mortality, with prevalence rates varying from 30% to 70% in affected individuals.
What is new here?
-
This study predicts mortality in Iranian elderly using the Frailty Index, demonstrating that frailty is a significant predictor with a 2.04 times higher risk of mortality compared to non-frail individuals.
-
The study identifies key risk factors for mortality in this population, including advanced age (especially 90 and above), presence of chronic comorbidities, and illiteracy, while literacy is identified as a protective factor.
Acknowledgements
We express our gratitude to the Iran Ministry of Health and Medical Education and the national social services agency for granting us access to the frailty assessment data from the Sina Electronic Health Record System and mortality data from the national death registry, which were instrumental in conducting this research.
References
- Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci 2001; 56(3):M146-56. doi: 10.1093/gerona/56.3.m146 [Crossref] [ Google Scholar]
- Chode S, Malmstrom TK, Miller DK, Morley JE. Frailty, diabetes, and mortality in middle-aged African Americans. J Nutr Health Aging 2016; 20(8):854-9. doi: 10.1007/s12603-016-0801-3 [Crossref] [ Google Scholar]
- Khosravi A, Alizadeh M, Torkashvand M, Aghaei N. Population Ageing in IR Iran. Tehran: United Nations Population Fund in Iran; 2014.
- Mohammadi S, Yazdani Charati J, Mousavinasab N. Factors affecting Iran’s population aging, 2016. J Mazandaran Univ Med Sci 2017; 27(155):71-8. [ Google Scholar]
- Bloom DE, Canning D, Fink G. Population aging and economic growth. In: Globalization and Growth. World Bank; 2010. p. 297-328.
- Thanh Trong N, Thi Dong N, Thi Ly P. Population aging and economic growth: evidence from ASEAN countries. Cogent Bus Manag 2024; 11(1):2298055. doi: 10.1080/23311975.2023.2298055 [Crossref] [ Google Scholar]
- Beard JR, Officer AM, Cassels AK. The world report on ageing and health. Gerontologist 2016; 56 Suppl 2:S163-6. doi: 10.1093/geront/gnw037 [Crossref] [ Google Scholar]
- Department of Economic. World Population Prospects 2024: Summary of Results. Stylus Publishing LLC; 2024.
- Mehri N, Messkoub M, Kunkel S. Trends, determinants and the implications of population aging in Iran. Ageing Int 2020; 45(4):327-43. doi: 10.1007/s12126-020-09364-z [Crossref] [ Google Scholar]
- Fathi E. The phenomenon of population aging in Iran. Iranian Journal of Official Statistics Studies 2020; 30(2):387-413. [ Google Scholar]
- Prince MJ, Wu F, Guo Y, Gutierrez Robledo LM, O’Donnell M, Sullivan R. The burden of disease in older people and implications for health policy and practice. Lancet 2015; 385(9967):549-62. doi: 10.1016/s0140-6736(14)61347-7 [Crossref] [ Google Scholar]
- Khodabakhshi H, Tiyuri A, Yari E, Beheshti D, Sharifzadeh G. Prevalence of non-communicable disease risk factors among the elderly of Birjand in 2014. Iran J Ageing 2019; 14(1):52-63. doi: 10.32598/sija.13.10.370 [Crossref] [ Google Scholar]
- Aminorroaya A, Fattahi N, Azadnajafabad S, Mohammadi E, Jamshidi K, Rouhifard Khalilabad M. Burden of non-communicable diseases in Iran: past, present, and future. J Diabetes Metab Disord 2024; 23(2):1793-9. doi: 10.1007/s40200-020-00669-z [Crossref] [ Google Scholar]
- Djalalinia S, Saeedi Moghaddam S, Moradi-Lakeh M, Shahraz S, Naghavi M, Murray CJL. Prevalence and years lived with disability of 310 diseases and injuries in Iran and its neighboring countries, 1990-2015: findings from Global Burden of Disease Study 2015. Arch Iran Med 2017; 20(7):392-402. [ Google Scholar]
- St John PD, Tyas SL, Menec V, Tate R. Multimorbidity, disability, and mortality in community-dwelling older adults. Can Fam Physician 2014; 60(5):e272-80. [ Google Scholar]
- Marengoni A, Angleman S, Melis R, Mangialasche F, Karp A, Garmen A. Aging with multimorbidity: a systematic review of the literature. Ageing Res Rev 2011; 10(4):430-9. doi: 10.1016/j.arr.2011.03.003 [Crossref] [ Google Scholar]
- Hahn RA, Truman BI. Education improves public health and promotes health equity. Int J Health Serv 2015; 45(4):657-78. doi: 10.1177/0020731415585986 [Crossref] [ Google Scholar]
- Li L, Duan L, Wang B, Wang K, Niu G, He S. Association of changes in frailty with mortality in the aged with hypertension. Sci Rep 2025; 15(1):12422. doi: 10.1038/s41598-025-95904-z [Crossref] [ Google Scholar]
- Wang X, Hu J, Wu D. Risk factors for frailty in older adults. Medicine (Baltimore) 2022; 101(34):e30169. doi: 10.1097/md.0000000000030169 [Crossref] [ Google Scholar]
- Fan J, Yu C, Guo Y, Bian Z, Sun Z, Yang L. Frailty index and all-cause and cause-specific mortality in Chinese adults: a prospective cohort study. Lancet Public Health 2020; 5(12):e650-60. doi: 10.1016/s2468-2667(20)30113-4 [Crossref] [ Google Scholar]
- Kojima G, Iliffe S, Walters K. Frailty index as a predictor of mortality: a systematic review and meta-analysis. Age Ageing 2018; 47(2):193-200. doi: 10.1093/ageing/afx162 [Crossref] [ Google Scholar]
- Talaee Boura F, Hosseini SR, Mouodi S, Ghadimi R, Bijani A. Frailty syndrome in older adults and related sociodemographic factors in the north of Iran: a population-based study. Iran Red Crescent Med J 2021; 23(1):e249. doi: 10.32592/ircmj.2021.23.1.249 [Crossref] [ Google Scholar]
- Saeidimehr S, Delbari A, Zanjari N, Fadaye Vatan R. Factors related to frailty among older adults in Khuzestan, Iran. Iran J Ageing 2021; 16(2):202-17. doi: 10.32598/sija.16.2.1600.1 [Crossref] [ Google Scholar]
- Norouzi M, Amiri Z, Farkhani EM, Hoseini SJ, Khosravi Asl T. Advancing healthcare infrastructure: the features of Iran’s Sina electronic health record system. Epidemiol Health System J 2024; 11(2):48-54. doi: 10.34172/ehsj.26105 [Crossref] [ Google Scholar]
- Jafari N, Kabir MJ, Motlagh ME. Death registration system in IR Iran. Iran J Public Health 1970; 38(Suppl 1):127-9. [ Google Scholar]
- Arts MH, van den Berg KS, Marijnissen RM, de Jonge L, Hegeman AJ, Collard RM. Frailty as a predictor of mortality in late-life depression: a prospective clinical cohort study. J Clin Psychiatry 2021; 82(3):20m13277. doi: 10.4088/JCP.20m13277 [Crossref] [ Google Scholar]
- Ruiz-Grao MC, Sánchez-Jurado PM, Molina-Alarcón M, Hernández-Martínez A, Avendaño Céspedes A, Abizanda P. Frailty, depression risk, and 10-year mortality in older adults: the FRADEA study. Int Psychogeriatr 2021; 33(8):803-12. doi: 10.1017/s1041610220003506 [Crossref] [ Google Scholar]
- Kremer KM, Braisch U, Rothenbacher D, Denkinger M, Dallmeier D. Systolic blood pressure and mortality in community-dwelling older adults: frailty as an effect modifier. Hypertension 2022; 79(1):24-32. doi: 10.1161/hypertensionaha.121.17530 [Crossref] [ Google Scholar]
- Mak JKL, Kuja-Halkola R, Wang Y, Hägg S, Jylhävä J. Frailty and comorbidity in predicting community COVID-19 mortality in the UK Biobank: the effect of sampling. J Am Geriatr Soc 2021; 69(5):1128-39. doi: 10.1111/jgs.17089 [Crossref] [ Google Scholar]
- Heyl J, Hardy F, Tucker K, Hopper A, Marchã MJ, Navaratnam AV. Frailty, comorbidity, and associations with in-hospital mortality in older COVID-19 patients: exploratory study of administrative data. Interact J Med Res 2022; 11(2):e41520. doi: 10.2196/41520 [Crossref] [ Google Scholar]
- Makizako H, Shimada H, Tsutsumimoto K, Lee S, Doi T, Nakakubo S, et al. Social frailty in community-dwelling older adults as a risk factor for disability. J Am Med Dir Assoc 2015; 16(11): 1003.e7-11. 10.1016/j.jamda.2015.08.023
- Nitta K, Hanafusa N, Tsuchiya K. Frailty and mortality among dialysis patients. Ren Replace Ther 2017; 3(1):41. doi: 10.1186/s41100-017-0122-y [Crossref] [ Google Scholar]
- Herr M, Robine JM, Pinot J, Arvieu JJ, Ankri J. Polypharmacy and frailty: prevalence, relationship, and impact on mortality in a French sample of 2350 old people. Pharmacoepidemiol Drug Saf 2015; 24(6):637-46. doi: 10.1002/pds.3772 [Crossref] [ Google Scholar]
- Garcia-Canton C, Rodenas A, Lopez-Aperador C, Rivero Y, Anton G, Monzon T. Frailty in hemodialysis and prediction of poor short-term outcome: mortality, hospitalization and visits to hospital emergency services. Ren Fail 2019; 41(1):567-75. doi: 10.1080/0886022x.2019.1628061 [Crossref] [ Google Scholar]
- López-Montes A, Martínez-Villaescusa M, Pérez-Rodríguez A, Andrés-Monpeán E, Martínez-Díaz M, Masiá J. Frailty, physical function and affective status in elderly patients on hemodialysis. Arch Gerontol Geriatr 2020; 87:103976. doi: 10.1016/j.archger.2019.103976 [Crossref] [ Google Scholar]
- Gordon EH, Peel NM, Samanta M, Theou O, Howlett SE, Hubbard RE. Sex differences in frailty: a systematic review and meta-analysis. Exp Gerontol 2017; 89:30-40. doi: 10.1016/j.exger.2016.12.021 [Crossref] [ Google Scholar]
- Kane AE, Howlett SE. Sex differences in frailty: Comparisons between humans and preclinical models. Mech Ageing Dev 2021; 198:111546. doi: 10.1016/j.mad.2021.111546 [Crossref] [ Google Scholar]
- Esbrí-Víctor M, Huedo-Rodenas I, López-Utiel M, Navarro-López JL, Martínez-Reig M, Serra-Rexach JA. Frailty and fear of falling: the FISTAC study. J Frailty Aging 2017; 6(3):136-40. doi: 10.14283/jfa.2017.19 [Crossref] [ Google Scholar]
- Uijen AA, van de Lisdonk EH. Multimorbidity in primary care: prevalence and trend over the last 20 years. Eur J Gen Pract 2008; 14 Suppl 1:28-32. doi: 10.1080/13814780802436093 [Crossref] [ Google Scholar]
- Arshadipour A, Thorand B, Linkohr B, Rospleszcz S, Ladwig KH, Heier M. Impact of prenatal and childhood adversity effects around World War II on multimorbidity: results from the KORA-Age study. BMC Geriatr 2022; 22(1):115. doi: 10.1186/s12877-022-02793-2 [Crossref] [ Google Scholar]
- Hanlon P, Nicholl BI, Jani BD, Lee D, McQueenie R, Mair FS. Frailty and pre-frailty in middle-aged and older adults and its association with multimorbidity and mortality: a prospective analysis of 493 737 UK Biobank participants. Lancet Public Health 2018; 3(7):e323-32. doi: 10.1016/s2468-2667(18)30091-4 [Crossref] [ Google Scholar]
- Pilotto A, Rengo F, Marchionni N, Sancarlo D, Fontana A, Panza F. Comparing the prognostic accuracy for all-cause mortality of frailty instruments: a multicentre 1-year follow-up in hospitalized older patients. PLoS One 2012; 7(1):e29090. doi: 10.1371/journal.pone.0029090 [Crossref] [ Google Scholar]
- Vetrano DL, Palmer K, Marengoni A, Marzetti E, Lattanzio F, Roller-Wirnsberger R. Frailty and multimorbidity: a systematic review and meta-analysis. J Gerontol A Biol Sci Med Sci 2019; 74(5):659-66. doi: 10.1093/gerona/gly110 [Crossref] [ Google Scholar]
- Rosamond W, Flegal K, Furie K, Go A, Greenlund K, Haase N. Heart disease and stroke statistics--2008 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation 2008; 117(4):e25-146. doi: 10.1161/circulationaha.107.187998 [Crossref] [ Google Scholar]
- Arshadipour A, Thorand B, Linkohr B, Ladwig KH, Heier M, Peters A. Multimorbidity patterns and mortality in older adults: results from the KORA-Age study. Front Nutr 2023; 10:1146442. doi: 10.3389/fnut.2023.1146442 [Crossref] [ Google Scholar]
- Pinheiro HA, de Almeida Mucio A, de Freitas Oliveira L. Prevalence and factors associated with the frailty syndrome in older adults in the Brazilian Federal District. Geriatr Gerontol Aging 2020; 14(1):8-14. doi: 10.5327/z2447-212320201900072 [Crossref] [ Google Scholar]
- Baker DP, Smith WC, Muñoz IG, Jeon H, Fu T, Leon J. The population education transition curve: education gradients across population exposure to new health risks. Demography 2017; 54(5):1873-95. doi: 10.1007/s13524-017-0608-9 [Crossref] [ Google Scholar]
- IHME-CHAIN Collaborators. Effects of education on adult mortality: a global systematic review and meta-analysis. Lancet Public Health 2024; 9(3):e155-65. doi: 10.1016/s2468-2667(23)00306-7 [Crossref] [ Google Scholar]