Journal of caring sciences. 14(3):173-181.
doi: 10.34172/jcs.025.33640
Original Article
Health-Related Quality of Life in Patients with Colorectal Cancer: A Comparison Between Those With and Without Colostomy
Amirmohammad Dahouri Conceptualization, Data curation, Investigation, Project administration, Visualization, Writing – original draft, 1, 2 
Mohammad Hassan Sahebihagh Conceptualization, Funding acquisition, Methodology, Resources, Project administration, Supervision, Validation, 1, 3, *
Neda Gilani Formal analysis, Methodology, Project administration, Supervision, Validation, 4
Leila Sheikhnezhad Writing – review & editing, 1
Author information:
1Department of Community Health Nursing, Faculty of Nursing and Midwifery, Tabriz University of Medical Sciences, Tabriz, Iran
2Student Research Committee, Tabriz University of Medical Sciences, Tabriz, Iran
3Tabriz Health Services Management Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
4Department of Statistics and Epidemiology, Faculty of Health, Tabriz University of Medical Sciences, Tabriz, Iran
Abstract
Introduction:
Colorectal cancer (CRC), as a leading cause of cancer-related morbidity and mortality worldwide, often requires surgical interventions such as colostomy, which can substantially affect patients’ health-related quality of life. The presence of a colostomy adversely affects deferent aspects of patient’s life. The aim of this study is to compare the health-related quality of life in patients with and without a colostomy.
Methods:
In this comparative cross-sectional study, 256 patients with CRC were included through convenience sampling, comprising 127 patients with a colostomy (49.6%) and 129 without a colostomy (50.4%). The data collection tools included the demographic information form and the shortened form of the health-related quality of life questionnaire (SF-36). Statistical analyses were performed using IBM SPSS Statistics version 13, including descriptive statistics, independent samples t-tests, general linear modeling, and multiple regression analyses. Results: In this study, the health-related quality of life score (range: 0–100) was 43.03±17.08 in patients with a colostomy and 51.38±15.57 in those without a colostomy. Also, there was a statistically significant difference in physical functioning, role limitation due to physical health, role limitation due to emotional problems and health-related quality of life in people with and without colostomies (P<0.05). Finally, in sex stratified exploratory analyses, differences were evident among women but not among men.
Conclusion:
This study demonstrates that patients with CRC, particularly those with a colostomy, experience significantly lower health-related quality of life. The findings emphasize the importance of early and targeted interventions to improve physical and psychosocial well-being in this population. Greater attention should be given to the needs of patients with colostomy in both hospital and community care settings to enhance their overall quality of life.
Keywords: Health-related quality of life, Quality of life, Colorectal neoplasms, Colostomy
Copyright and License Information
© 2025 The Author(s).
This work is published by Journal of Caring Sciences as an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/). Non-commercial uses of the work are permitted, provided the original work is properly cited.
Funding Statement
This study was supported by Tabriz University of Medical Sciences (grant number: 69407).
Introduction
Colorectal cancer (CRC) presents a significant global health challenge, ranking as the second leading cause of cancer-related deaths in the United States.1 In Iran, CRC accounts for a substantial proportion of cancer cases, constituting 38% of all diagnosed cancers and contributing to 44.4% of cancer-related fatalities, making it one of the most prevalent cancers in the country.2,3 Over the past 25 years, the incidence of CRC in Iran has risen notably, positioning it as the fourth most common cancer overall, the third most common among Iranian women, and the fifth most common among Iranian men.4,5
Beyond its impact on individual health, CRC imposes significant economic and psychosocial burdens.6 Advances in cancer treatment have led to a growing population of cancer survivors, including those living with an ostomy or permanent stoma.7,8 Annually, approximately 100,000 patients worldwide undergo intestinal ostomy surgery, with significant numbers in England and the United States.9-11 The presence of a stoma introduces various psychosocial challenges for cancer survivors, who must manage their ostomy and adapt to considerable lifestyle changes.7,8 A critical aspect of survivorship in cancer care is health-related quality of life (HRQoL).12 While quality of life encompasses broader factors such as access to nutritious food and clean water, HRQoL specifically refers to an individual’s perception of their psychological, physical, and social well-being. In CRC patients, HRQoL is influenced by diagnosis, treatment, post-treatment recovery, and long-term survivorship and is commonly assessed using validated tools.13
HRQoL assessment tools measure multiple dimensions of well-being, including: Physical functioning (evaluates limitations in physical), social functioning (assesses the ability to engage in social activities and maintain relationships), role Functioning (looks at how health issues impact daily roles, such as work and family responsibilities), general health perceptions (captures an individual’s overall view of their health status and life satisfaction), fatigue/ energy levels (measures fatigue, energy levels, and overall feelings of vigor), pain (evaluates the presence and impact of pain on daily activities and quality of life), emotional well-being (assesses psychological aspects such as anxiety, depression, and emotional stability, reflecting how health affects mental resilience and overall mood).14 A scoping review by Corrigan et al highlighted the challenges faced by cancer patients undergoing radiotherapy, including disturbances in body image, sexual health, fertility, and financial hardship, all of which significantly affect HRQoL.15 Similarly, Mokhtari-Hessari and Montazeri found that while HRQoL in breast cancer patients has improved in recent years, symptoms such as pain and sexual dysfunction—particularly among younger patients—remain inadequately addressed.13
Previous studies have consistently reported that individuals diagnosed with CRC experience lower HRQoL compared to the general population.16-20 While Omani CRC survivors generally report satisfactory HRQoL, many face persistent psychological, emotional, and physical challenges.21Patients with a permanent colostomy, in particular, undergo major life changes often perceived as traumatic, which can further compromise HRQoL.20,22
Despite this understanding, there remains a notable lack of studies investigating the specific impact of colostomy on HRQoL in CRC patients. Comparative analyses between patients with and without a colostomy are also limited. This study therefore aimed to compare HRQoL between CRC patients with a colostomy and those without a colostomy. In addition, exploratory subgroup analyses were conducted to examine whether the observed associations differed between women and men. By addressing these gaps, the aim of this study is to compare the HRQoL in patients with and without a colostomy.
Materials and Methods
This comparative cross-sectional study was conducted in Tabriz, Iran, between April 1 and May 1, 2022. The study was carried out in several outpatient chemotherapy centers, including both public and private hospitals. The setting ensured access to a diverse patient population while minimizing disruption to routine clinical care.
The study population consisted of patients with a confirmed diagnosis of CRC who was receiving care at the selected hospitals. Inclusion criteria required participants to be over 30 years of age, able to communicate effectively, and to have sufficient knowledge of their disease and treatment. Patients with either a temporary or permanent colostomy were eligible for inclusion, as were those without a colostomy. Additional inclusion requirements were prior sexual activity and continued sexual function before the onset of disease, to allow for comparability of HRQoL assessments. Exclusion criteria included the presence of chronic comorbidities such as diabetes, cardiovascular disease, or kidney disease that could influence HRQoL, as well as any self-reported cognitive disorders such as Alzheimer’s disease or documented psychiatric disorders. Patients unwilling to participate were also excluded. Figure 1 illustrates the participant selection process through a detailed sampling flowchart, offering a clear overview of how the study population was recruited.
Based on the study by Näsvall and colleagues,23 which assessed quality of life in CRC patients using the SF-36, the required sample size was determined with an alpha of 0.05, a power of 0.90, and adjustment for a design effect and expected dropout. This yielded a final sample size of 252 participants, with 126 in the colostomy group and 126 in the non-colostomy group. In total, 256 patients were ultimately recruited through cluster random sampling, in which hospitals were treated as clusters and patients were selected according to their treatment schedules. It should be noted that G-power software was utilized to ensure accurate sample size estimation.24
Data collection involved two instruments. A researcher-designed questionnaire was used to obtain demographic and clinical information, including age, sex, education level, marital status, medical history, and treatment details. To evaluate HRQoL, the validated Persian version of the 36-Item Short Form Health Survey (SF-36) was administered.25 The SF-36 measures eight dimensions of well-being: physical functioning, role limitations due to physical health, role limitations due to emotional problems, vitality, emotional well-being, social functioning, pain, and general health perceptions. Items are rated using a Likert-type scale, where respondents indicate the frequency of each health aspect: 1 = All the time, 2 = Most of the time, 3 = Sometimes, 4 = Rarely, and 5 = Never. Responses are then transformed to a 0–100 scale for each domain, with higher scores reflecting better HRQoL. The instrument has shown strong psychometric properties internationally and in Iran,26-28 including a Cronbach’s alpha of 0.92, confirming its internal consistency.27-29
Data collection was facilitated by trained researchers who assisted patients in completing the questionnaires to ensure accuracy. Recruitment and data gathering were coordinated with hospital chemotherapy departments to minimize interference with patient care.
Data analysis was performed using IBM SPSS Statistics version 13. Descriptive statistics, including frequencies, percentages, means, and standard deviations, were used to summarize demographic and HRQoL data. The Kolmogorov–Smirnov test, as well as skewness and kurtosis indices, were applied to assess normality. Independent samples t-tests were conducted to compare mean HRQoL scores between groups. In addition, general linear modeling and multiple regression analyses were applied to control for potential confounders. The primary analysis focused on comparing HRQoL between patients with and without a colostomy. Sex-stratified analyses were conducted as exploratory and were not included in the original sample size calculation. In addition to mean score comparisons, radar charts were generated to provide a visual representation of HRQoL profiles across different domains. For this purpose, mean rank values were obtained from Friedman test. The mean rank values for each HRQoL domain were exported from SPSS to Microsoft Excel, where radar diagrams were created separately for patients with and without a colostomy. This approach allowed for a comparative visualization of multidimensional HRQoL patterns between groups.
Results
Table 1.
Distribution of frequency and percentage of individual characteristics of samples (N = 256)
|
Variable
|
Categories
|
N (%)
|
| Age |
30 to 40 |
67 (26.2) |
| 40 to 50 |
46 (18.0) |
| 50 to 60 |
95 (37.1) |
| More than 60 |
48 (18.8) |
| Mean (SD) |
47.74 (11.77) |
| Gender |
Male |
129 (50.4) |
| Female |
127 (49.6) |
| Marital status |
Single |
22 (8.6) |
| Married |
206 (80.5) |
| Divorced and widowed |
28 (10.9) |
| Education |
Under diploma |
50 (19.5) |
| Diploma |
73 (28.5) |
| Bachelor |
81 (31.6) |
| post graduate |
52 (20.3) |
| Job |
Employed |
Negative |
| Unemployed |
90 (35.2) |
| Income adequacy |
Income equals expenditure |
138 (53.9) |
| Income more than expenditure |
42 (16.4) |
| Income less than expenditure |
76 (29.7) |
| Weight (kg) |
45-65 |
63 (24.6) |
| ≥ 65-85 |
126 (49.2) |
| ≥ 85-105 |
67 (26.2) |
| Mean (SD) |
74.71 (14.42) |
| Height (cm) |
70-130 |
3 (1.2) |
| ≥ 130-192 |
253 (98.8) |
| Mean (SD) |
169.34 (13.48) |
| Body mass index (kg/m2) |
< 18.5 |
12 (4.7) |
| ≥ 18.5-25 |
123 (48) |
| ≥ 25-30 |
67 (26.2) |
| ≥ 30 |
54 (21.1) |
| Mean (SD) |
25.88 (4.74) |
| Time of last surgery (month) |
1-10 |
223 (87.1) |
| ≥ 10-20 And more |
33 (12.9) |
| Mean (SD) |
6.11 (5.52) |
| Having insurance |
Yes |
228 (89.1) |
| No |
28 (10.9) |
| Location |
City |
240 (93.8) |
| Village |
16 (6.3) |
| Housing type |
Personal |
228 (89.1) |
| Rent |
28 (10.9) |
| Type of treatment |
Only chemotherapy |
81 (31.6) |
| Chemotherapy-radiotherapy-surgery |
98 (38.3) |
| Chemotherapy-surgery |
77 (30.1) |
| Time of last chemotherapy (wk) |
< 5 |
232 (90.6) |
| ≥ 5-10 |
24 (9.4) |
| Mean (SD) |
3.10 (4.04) |
| Family history |
Positive |
121 (47.3) |
| Negative |
135 (52.7) |
| Exercise (h/wk) |
10 |
229 (89.5) |
| ≥ 10-20 And more |
27 (10.5) |
| Mean (SD) |
3.42 (3.84) |
| Metastasis |
Yes |
149 (58.2) |
| No |
107 (41.8) |
| Another disease besides cancer |
Yes |
106 (41.4) |
| No |
150 (58.6) |
| Having colostomy |
Yes |
127 (49.6) |
| No |
129 (51.4) |
| No. of chemotherapy courses (Number) |
< 10 |
137 (53.5) |
| ≥ 10-20 |
84 (32.8) |
| ≥ 20-30 |
35 (13.7) |
| Mean (SD) |
9.34 (6.98) |
| Sexually active before the disease |
Active |
251 (98) |
| Not active |
5 (2) |
Table 2.
Total HRQoL scores and comparisons between patients with and without colostomy (N = 256)
|
Dimensions
|
Mean (SD)
|
95 % Cl Max-Min
|
Comparison between groups
|
|
With colostomy
|
Without colostomy
|
With colostomy
|
Without colostomy
|
P
value
*
|
df
|
t
|
| Physical Functioning |
39.88 (30.41) |
50.04 (30.81) |
0 – 100 |
0 – 100 |
0.009 |
252 |
-2.64 |
| Role limitations due to Physical health |
54.92 (41.79) |
69.77 (38.23) |
0 – 100 |
0 – 100 |
0.003 |
254 |
-2.96 |
| Role limitations due to emotional problems |
52.69 (41.88) |
71.06 (38.27) |
0 – 100 |
0 – 100 |
< 0.001 |
251 |
-3.64 |
| Energy/Fatigue |
52.64 (15.62) |
51.94 (16.36) |
5 – 100 |
10 – 100 |
0.727 |
252 |
0.35 |
| Emotional well-being |
57.92 (14.68) |
57.22 (16.51) |
32 – 100 |
20 – 100 |
0.720 |
250 |
0.35 |
| Social functioning |
47.93 (23.13) |
48.16 (24.90) |
0 – 100 |
0 – 100 |
0.940 |
254 |
-0.07 |
| Pain |
41.99 (25.01) |
45.18 (26.94) |
0 – 100 |
0 – 100 |
0.329 |
252 |
-0.97 |
| General health |
32.48 (8.26) |
34.33 (8.51) |
6 – 46 |
10 – 56 |
0.163 |
161 |
-1.40 |
| Total score of HRQoL |
43.03 (17.08) |
51.38 (15.57) |
6 – 74 |
15 – 75 |
0.002 |
148 |
-3.13 |
Table 3.
Comparison of HRQoL scores between patients with and without colostomy by sex (N = 256)
|
Dimensions
|
Mean (SD) female (N = 127)
|
Comparison between groups
|
Mean (SD) for male (N = 129)
|
Comparison between groups
|
|
With colostomy
|
Without colostomy
|
P
-value
*
|
df
|
t
|
With colostomy
|
Without colostomy
|
P
value
*
|
df
|
t
|
| Physical functioning |
24.53 (25.73) |
49.75 (28.54) |
< 0.001 |
123 |
-5.19 |
55.48 (26.75) |
50.30 (32.99) |
0.331 |
127 |
0.97 |
| Role limitations due to physical health |
35.94 (37.76) |
69.84 (38.14) |
< 0.001 |
125 |
-5.03 |
74.21 (36.74) |
69.70 (38.60) |
0.498 |
127 |
0.67 |
| Role limitations due to emotional problems |
30.21 (37.89) |
69.31 (38.93) |
< 0.001 |
125 |
-5.73 |
76.67 (31.47) |
72.73 (37.85) |
0.529 |
124 |
0.63 |
| Energy/fatigue |
47.26 (12.46) |
47.54 (10.92) |
0.893 |
123 |
-0.13 |
57.94 (16.67) |
56.14 (19.41) |
0.574 |
127 |
0.56 |
| Emotional well-being |
54.00 (7.26) |
53.05 (10.47) |
0.555 |
123 |
0.59 |
61.90 (18.77) |
61.19 (19.97) |
0.835 |
125 |
0.20 |
| Social functioning |
40.63 (18.36) |
40.92 (20.30) |
0.118 |
125 |
-1.57 |
55.36 (25.17) |
50.19 (28.63) |
0.279 |
127 |
1.08 |
| Pain |
30.94 (19.12) |
43.73 (23.58) |
0.001 |
123 |
-3.33 |
53.21 (25.41) |
46.52 (29.83) |
0.173 |
127 |
1.37 |
| General health |
32.74 (9.20) |
36.44 (8.15) |
0.041 |
93 |
-2.06 |
32.18 (7.20) |
30.69 (7.96) |
0.419 |
66 |
0.81 |
| Total score of HRQoL |
34.09 (10.47) |
52.15 (15.41) |
< 0.001 |
85 |
-6.19 |
53.31 (17.54) |
50.12 (16.02) |
0.454 |
61 |
0.75 |
Table 4.
Univariate and multiple linear regression model of HRQoL to compare two groups with and without
|
Variant
|
Class
|
Univariate linear regression
|
Multiple linear regression
|
|
P
value
|
β (95% CI)
|
P
value
|
β (95% CI)
|
| Group |
With colostomy |
0.002 |
-8.35 (-13.62, -3.08) |
< 0.001 |
-10.14 (-15.54, -4.73) |
| Without colostomy |
Reference string |
Reference string |
R squared = 0.554 (Adjusted R squared = 0.427).
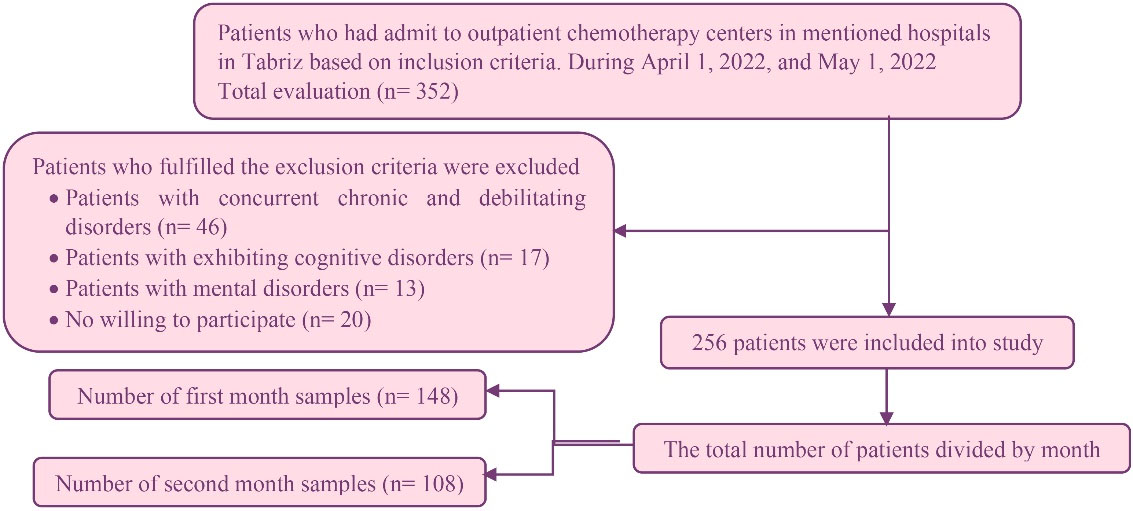
Figure 1.
Consort flow diagram (inclusion-exclusion criteria)
.
Consort flow diagram (inclusion-exclusion criteria)
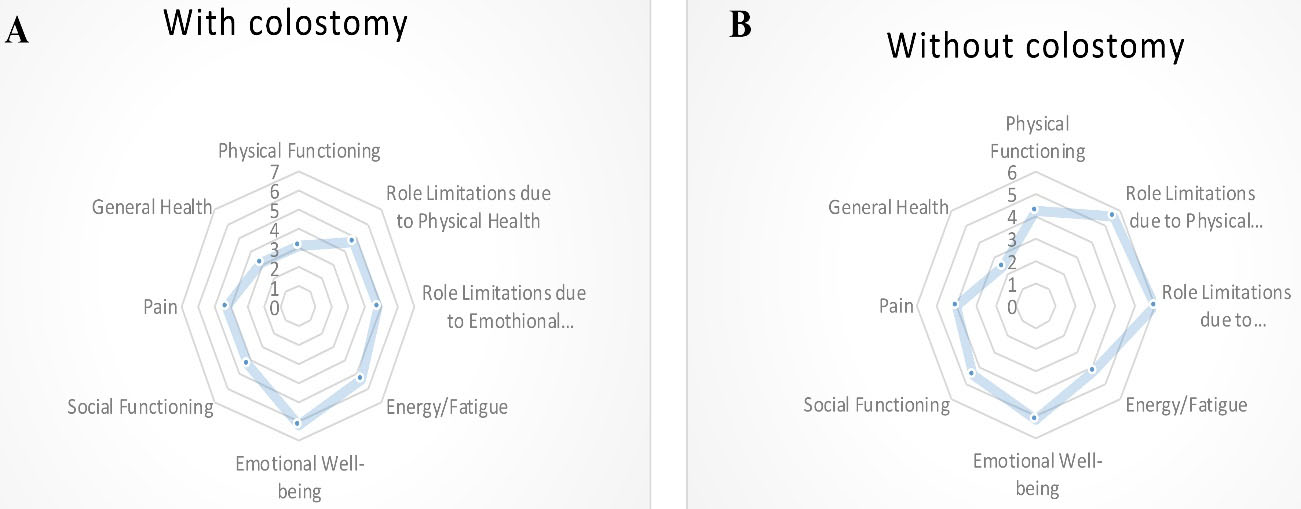
Figure 2.
Radar diagram of HRQoL scores in different domains
.
Radar diagram of HRQoL scores in different domains
Discussion
This study investigated the impact of having a colostomy on HRQoL among CRC patients, with particular attention to sex-specific differences across HRQoL domains. Understanding these patterns is essential for identifying vulnerable patient groups and informing targeted interventions aimed at improving long-term well-being.
One significant finding of this study is the relatively low scores observed across multiple dimensions of HRQoL in both patients with and without a colostomy. This demonstrates the significant impact of CRC and its management on multiple aspects of patients’ daily functioning and well-being. HRQoL is a critical factor not only in shaping the patient’s subjective experience but also in influencing their treatment response and long-term survival outcomes.30 Previous studies have thoroughly investigated various factors affecting HRQoL in CRC patients, identifying symptoms, surgical interventions, and comorbidities as major contributors to diminished quality of life.31 In a study by Färkkilä et al32 patients with CRC undergoing palliative treatment exhibited lower HRQoL, findings that align with the results of our study. Additionally, a review of breast cancer research indicated that while HRQoL in breast cancer patients has improved over recent decades, it still remains a significant concern.13 This suggests that interventions successful in improving HRQoL in breast cancer patients could potentially be applied to CRC patients to enhance their quality of life. Therefore, a comprehensive approach to understanding HRQoL in CRC patients must consider a range of factors beyond just the presence of a colostomy.
Another important finding of this study is the statistically significant lower total HRQoL scores among individuals with a colostomy compared to those without. This finding supports previous research that has consistently shown how patients with ostomies encounter numerous challenges that impact their quality of life.33-35 The presence of a colostomy contributes to a decrease in HRQoL during treatment. It is important to recognize that the reduction in HRQoL is not solely attributed to the colostomy but is influenced by other factors as well.
The study also examined specific dimensions of HRQoL, including physical functioning, role limitations due to physical health, role limitations due to emotional problems, and the overall score. A statistically significant difference was observed between individuals with and without a colostomy. Previous studies have indicated that a decline in physical functioning can lead to a loss of independence,31 while the presence of a stoma in cancer patients contributes to various psychosocial problems.7 To enhance the HRQoL of CRC patients, interventions should focus on improving physical functioning and addressing psychosocial well-being. Social challenges faced by these patients include reduced interest and participation in social activities, avoidance of travel, decreased work engagement, deteriorating sexual relations, and decreased communication with friends and relatives.36-38Psychological issues encompass depression, anxiety, body image changes, and low self-esteem.7
Furthermore, the study revealed that Women with a colostomy had lower scores than women without a colostomy in several domains in exploratory analyses, while findings in men were not significant. These subgroup results should be viewed as hypothesis generating. This gender disparity was observed in dimensions such as physical functioning, role limitations due to physical health, role limitations due to emotional problems, pain, and the overall HRQoL score. These findings emphasize the vulnerability of women with colostomy pouches and underscore the importance of providing targeted attention and support to address their unique challenges. Research has indicated that the HRQoL for women with colostomies is particularly compromised, aligning with findings from previous studies that highlight the disparities in health outcomes based on gender.39,40 Healthcare providers, especially those in women’s health, should be mindful of this vulnerable group and deliver appropriate care to improve their quality of life.41
Previous research has highlighted the positive correlation between higher levels of adaptation in chronic conditions such as living with a stoma and the adoption of health-promoting behaviors, leading to a reduced risk of relapse.42 Additionally, comprehensive knowledge about the impact of ostomies on HRQoL has proven beneficial in preparing and informing patients before surgery.43 These findings emphasize the need for oncologists, psychiatrists, oncology nurses, and health planners to prioritize the dimensions of quality of life among ostomy patients to facilitate their adaptation and improve their overall well-being. This, in turn, will contribute to enhance HRQoL, particularly in the dimensions mentioned. Preoperative discussions and informative sessions with physician and nurses can help patients make informed decisions regarding treatment choices and set realistic expectations.44 The duration since surgery also plays a significant role in successfully adapting to life with an ostomy. Many challenges, such as changes in body appearance, anxiety about ostomy leakage, unpleasant odor, bowel sounds, and loss of sexual desire, tend to diminish over time.45 In some studies on supportive interventions, immediate post-surgery ostomy care and support are emphasized.46 The present study’s findings reinforce the importance of timely interventions and the provision of attentive care as soon as possible after surgery.
It is crucial to recognize that quality of life is a comprehensive concept encompassing all factors affecting an individual’s life, whereas HRQoL specifically focuses on aspects related to health.47 In social settings, care is centered around maximizing an individual’s self-care potential, regardless of injury or illness, with the responsibility for health care resting with the patient.48 Changes in healthcare services have necessitated shifts in nursing care, with an emphasis on community-based and home care. The purpose of such care is not merely treatment but rather the improvement of quality of life and the implementation of supportive measures to enhance patient comfort. Health professionals, especially nurses, play a crucial role in improving the quality of life of ostomy patients. Their knowledge and skills are instrumental in providing comprehensive care before and after ostomy surgery, ultimately contributing to enhanced patient outcomes and well-being.49
This study has some limitations that should be acknowledged. The sample size was relatively limited and may not fully capture the diversity of experiences among CRC patients, which restricts the generalizability of the findings. In addition, subgroup analyses by sex were exploratory and the study was not sufficiently powered to detect such differences; therefore, these results should be interpreted with caution. Future research with larger and more diverse samples is needed to confirm these findings and provide more robust evidence, particularly regarding gender-specific outcomes. Expanding the scope of investigation to include clinical and psychosocial factors would also allow for a more comprehensive understanding of HRQoL in this patient population.
Conclusion
In conclusion, this study examined HRQoL in CRC patients with and without a colostomy, with attention to sex-specific differences. The findings highlight the relatively low HRQoL scores in this population and the significant impact of a colostomy, particularly in domains related to physical functioning and psychosocial well-being. Gender differences were also observed, with women with colostomies reporting lower HRQoL compared to their counterparts without ostomy. These results underscore the importance of comprehensive support, timely postoperative interventions, and patient education to facilitate adaptation and improve quality of life. By recognizing the multidimensional nature of HRQoL, healthcare professionals, especially nurses, can play a key role in delivering patient-centered care and enhancing outcomes for ostomy patients.
Acknowledgements
This study was conducted as part of the Master Thesis of the first author (Amirmohammad Dahouri) at the Tabriz University of Medical Sciences. In addition, we would like to appreciate of the cooperation of Clinical Research Development Unit, Imam Reza General Hospital, Tabriz, Iran in conducting of this research.
Competing Interests
The authors reported no actual or potential conflict of interest.
Data Availability Statement
Data of this manuscript has been gathered through questionnaires by patients themselves the questioner was actively present when the questionnaires were filled and provided the necessary guidance in filling the questionnaires by the patients. The data sets used and analyzed for the current study are available upon reasonable request of the corresponding author Dr. Mohammad Hassan Sahebihagh.
Ethical Approval
This study prioritized ethical principles and obtained necessary approvals and permissions from relevant authorities. The research plan received approval from the Research Council and the Research Vice-Chancellor of the Faculty of Nursing and Midwifery at Tabriz University. Permission to conduct the study was granted by the Research Vice-Chancellor of Tabriz University of Medical Sciences, with approval from the regional ethics committee (reference number IR.TBZMED.REC.1401.046). Participants were fully informed about the research objectives, and their voluntary participation was sought. Confidentiality and anonymity were ensured through the use of a coding system instead of actual names. Ethical guidelines were followed for the use of other research and sources, with proper citation and referencing. The research findings were made available to participants upon request, promoting transparency and accountability.
Research Highlights
What is the current knowledge?
-
CRC significantly reduces HRQoL in patients.
-
Colostomies impose physical, psychosocial, and sexual challenges on patients.
-
Women with CRC may experience worse HRQoL outcomes than men.
-
HRQoL can improve with adaptation, supportive care, and patient education.
-
Previous studies have primarily focused on general HRQoL in CRC or other cancers, with limited comparative data between patients with and without colostomy.
What is new here?
-
Confirms that HRQoL is lower in Iranian CRC patients with a colostomy compared to those without, highlighting the impact of stoma on multiple HRQoL domains.
-
Quantifies these challenges and identifies specific HRQoL dimensions most affected, including physical functioning, role limitations (physical and emotional), pain, and social well-being.
-
Demonstrates that women with a colostomy report significantly lower HRQoL in multiple domains compared to women without a colostomy, emphasizing sex-specific vulnerabilities.
-
Reinforces the importance of timely interventions, pre- and post-operative patient education, and nursing care to improve adaptation and HRQoL among ostomy patients.
-
Provides a direct comparison of HRQoL between CRC patients with and without colostomy, filling a gap in the literature and offering evidence for targeted clinical interventions.
References
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2021. CA Cancer J Clin 2021; 71(1):7-33. doi: 10.3322/caac.21654 [Crossref] [ Google Scholar]
- Asgarian FS, Mahdian M, Amori N. Epidemiology and trends of gastrointestinal cancer in Iran (2004-2008). J Cancer Res Ther 2021; 17(4):963-8. doi: 10.4103/jcrt.JCRT_509_19 [Crossref] [ Google Scholar]
- Mousavi SM, Gouya MM, Ramazani R, Davanlou M, Hajsadeghi N, Seddighi Z. Cancer incidence and mortality in Iran. Ann Oncol 2009; 20(3):556-63. doi: 10.1093/annonc/mdn642 [Crossref] [ Google Scholar]
- Ostadghaderi M, Hanafi Bojd A, Nematollahi SH, Holakoui-Naeini K. Spatial analysis of factors affecting colorectal cancer using the model of geographical weight regression in Iran. Iran J Epidemiol 2021; 17(1):1-12. [ Google Scholar]
- Abbastabar H, Roustazadeh A, Alizadeh A, Hamidifard P, Valipour M, Valipour AA. Relationships of colorectal cancer with dietary factors and public health indicators: an ecological study. Asian Pac J Cancer Prev 2015; 16(9):3991-5. doi: 10.7314/apjcp.2015.16.9.3991 [Crossref] [ Google Scholar]
- Bray F, Sankila R, Ferlay J, Parkin DM. Estimates of cancer incidence and mortality in Europe in 1995. Eur J Cancer 2002; 38(1):99-166. doi: 10.1016/s0959-8049(01)00350-1 [Crossref] [ Google Scholar]
- Ayaz-Alkaya S. Overview of psychosocial problems in individuals with stoma: a review of literature. Int Wound J 2019; 16(1):243-9. doi: 10.1111/iwj.13018 [Crossref] [ Google Scholar]
- Villa G, Manara DF, Brancato T, Rocco G, Stievano A, Vellone E. Life with a urostomy: a phenomenological study. Appl Nurs Res 2018; 39:46-52. doi: 10.1016/j.apnr.2017.10.005 [Crossref] [ Google Scholar]
- Ozturk O, Yalcin BM, Unal M, Yildirim K, Ozlem N. Sexual dysfunction among patients having undergone colostomy and its relationship with self-esteem. J Fam Med Community Health 2015; 2(1):1028. doi: 10.47739/2379-0547/1028 [Crossref] [ Google Scholar]
- Davis BR, Valente MA, Goldberg JE, Lightner AL, Feingold DL, Paquette IM. The American Society of Colon and Rectal Surgeons clinical practice guidelines for ostomy surgery. Dis Colon Rectum 2022; 65(10):1173-90. doi: 10.1097/dcr.0000000000002498 [Crossref] [ Google Scholar]
- International Association for Stoma Care. Ostomy Facts and Figures [Internet]. IASupport.org. Available from: https://iasupport.org. Accessed August 27, 2025.
- Bunkong S, Arpanantikul M, Sirapo-Ngam Y, Monkong S, Viwatwongkasem C, Olson K. A model of factors influencing health-related quality of life among Thais with colorectal cancer and a permanent colostomy. Pac Rim Int J Nurs Res 2023; 27(1):185-99. doi: 10.60099/prijnr.2023.260341 [Crossref] [ Google Scholar]
- Mokhtari-Hessari P, Montazeri A. Health-related quality of life in breast cancer patients: review of reviews from 2008 to 2018. Health Qual Life Outcomes 2020; 18(1):338. doi: 10.1186/s12955-020-01591-x [Crossref] [ Google Scholar]
- Guyatt GH, Feeny DH, Patrick DL. Measuring health-related quality of life. Ann Intern Med 1993; 118(8):622-9. doi: 10.7326/0003-4819-118-8-199304150-00009 [Crossref] [ Google Scholar]
- Corrigan KL, Reeve BB, Salsman JM, Siembida EJ, Andring LM, Geng Y. Health-related quality of life in adolescents and young adults with cancer who received radiation therapy: a scoping review. Support Care Cancer 2023; 31(4):230. doi: 10.1007/s00520-023-07682-x [Crossref] [ Google Scholar]
- Northouse LL, Caffey M, Deichelbohrer L, Schmidt L, Guziatek-Trojniak L, West S. The quality of life of African American women with breast cancer. Res Nurs Health 1999; 22(6):449-60. [ Google Scholar]
- Chopra I, Kamal KM. A systematic review of quality of life instruments in long-term breast cancer survivors. Health Qual Life Outcomes 2012; 10:14. doi: 10.1186/1477-7525-10-14 [Crossref] [ Google Scholar]
- Thors CL, Broeckel JA, Jacobsen PB. Sexual functioning in breast cancer survivors. Cancer Control 2001; 8(5):442-8. doi: 10.1177/107327480100800508 [Crossref] [ Google Scholar]
- Bouleuc C, Anota A, Cornet C, Grodard G, Thiery-Vuillemin A, Dubroeucq O. Impact on health-related quality of life of parenteral nutrition for patients with advanced cancer cachexia: results from a randomized controlled trial. Oncologist 2020; 25(5):e843-51. doi: 10.1634/theoncologist.2019-0856 [Crossref] [ Google Scholar]
- Laghousi D, Jafari E, Nikbakht H, Nasiri B, Shamshirgaran M, Aminisani N. Gender differences in health-related quality of life among patients with colorectal cancer. J Gastrointest Oncol 2019; 10(3):453-61. doi: 10.21037/jgo.2019.02.04 [Crossref] [ Google Scholar]
- Al-Shandudi M, Al-Mandhari M, Chan MF, Al-Hajri T, Al-Balushi M, Al-Azri M. Health-related quality of life of Omani colorectal cancer survivors. Cancer Control 2022; 29:10732748221084198. doi: 10.1177/10732748221084198 [Crossref] [ Google Scholar]
- Zhang Y, Xian H, Yang Y, Zhang X, Wang X. Relationship between psychosocial adaptation and health-related quality of life of patients with stoma: a descriptive, cross-sectional study. J Clin Nurs 2019; 28(15-16):2880-8. doi: 10.1111/jocn.14876 [Crossref] [ Google Scholar]
- Näsvall P, Dahlstrand U, Löwenmark T, Rutegård J, Gunnarsson U, Strigård K. Quality of life in patients with a permanent stoma after rectal cancer surgery. Qual Life Res 2017; 26(1):55-64. doi: 10.1007/s11136-016-1367-6 [Crossref] [ Google Scholar]
- Campbell MJ, Machin D, Walters SJ. Medical Statistics: A Textbook for the Health Sciences. 4th ed. Chichester: John Wiley & Sons; 2010.
- Ware JE Jr, Sherbourne CD. Ware JE Jr, Sherbourne CDThe MOS 36-item short-form health survey (SF-36)IConceptual framework and item selection. Med Care 1992; 30(6):473-83. [ Google Scholar]
- Montazeri A, Goshtasebi A, Vahdaninia MS. The Short Form Health Survey (SF-36): translation and validation study of the Iranian version. Payesh 2006; 5(1):49-56. [Persian].
- Rafaati S, Bagheri Z, Jafari P, Soltani N. Using confirmatory factor analysis (CFA) to assess structure of SF-36 (Persian version) questions for normal people and patients with chronic diseases. Hormozgan Med J 2015; 19(2): 121-8. [Persian].
- Motamed N, Ayatollahi AR, Zare N, Sadeghi-Hassanabadi A. Validity and reliability of the Persian translation of the SF-36 version 2 questionnaire. East Mediterr Health J 2005; 11(3):349-57. [ Google Scholar]
- Asadollahi A, Ismaeli A, Fani-Saberi L. Validity and reliability of quality of life test among Ahwaz older adults in 2016. J Sociol Stud 2016; 9(32): 7-15. [Persian].
- Quinten C, Coens C, Mauer M, Comte S, Sprangers MA, Cleeland C. Baseline quality of life as a prognostic indicator of survival: a meta-analysis of individual patient data from EORTC clinical trials. Lancet Oncol 2009; 10(9):865-71. doi: 10.1016/s1470-2045(09)70200-1 [Crossref] [ Google Scholar]
- Marventano S, Forjaz M, Grosso G, Mistretta A, Giorgianni G, Platania A. Health related quality of life in colorectal cancer patients: state of the art. BMC Surg 2013; 13(Suppl 2):S15. doi: 10.1186/1471-2482-13-s2-s15 [Crossref] [ Google Scholar]
- Färkkilä N, Sintonen H, Saarto T, Järvinen H, Hänninen J, Taari K. Health-related quality of life in colorectal cancer. Colorectal Dis 2013; 15(5):e215-22. doi: 10.1111/codi.12143 [Crossref] [ Google Scholar]
- Coons SJ, Chongpison Y, Wendel CS, Grant M, Krouse RS. Overall quality of life and difficulty paying for ostomy supplies in the Veterans Affairs ostomy health-related quality of life study: an exploratory analysis. Med Care 2007; 45(9):891-5. doi: 10.1097/MLR.0b013e318074ce9b [Crossref] [ Google Scholar]
- Adel Mehraban M, Ashoori E, Moladoost A, Aghaei S. Psychological experiences of patients with surgical stoma (colostomy): a phenomenological study. J Res Behav Sci 2008; 6(2): 119-27. [Persian].
- Borwell B. Continuity of care for the stoma patient: psychological considerations. Br J Community Nurs 2009; 14(8):326, 8, 30-1. doi: 10.12968/bjcn.2009.14.8.43511 [Crossref] [ Google Scholar]
- Ayaz S. Approach to sexual problems of patients with stoma by PLISSIT model: an alternative. Sex Disabil 2009; 27(2):71-81. doi: 10.1007/s11195-009-9113-4 [Crossref] [ Google Scholar]
- Grant M, McMullen CK, Altschuler A, Mohler MJ, Hornbrook MC, Herrinton LJ. Gender differences in quality of life among long-term colorectal cancer survivors with ostomies. Oncol Nurs Forum 2011; 38(5):587-96. doi: 10.1188/11.Onf.587-596 [Crossref] [ Google Scholar]
- Gautam S, Poudel A. Effect of gender on psychosocial adjustment of colorectal cancer survivors with ostomy. J Gastrointest Oncol 2016; 7(6):938-45. doi: 10.21037/jgo.2016.09.02 [Crossref] [ Google Scholar]
- Roth ME, Parsons SK, Ganz PA, Wagner LI, Hinds PS, Alexander S. Inclusion of a core patient-reported outcomes battery in adolescent and young adult cancer clinical trials. J Natl Cancer Inst 2023; 115(1):21-8. doi: 10.1093/jnci/djac166 [Crossref] [ Google Scholar]
- Özden ZM, Kılıç M. The effect of self-efficacy levels of patients with intestinal stoma on stoma adaptation. Support Care Cancer 2023; 31(5):252. doi: 10.1007/s00520-023-07702-w [Crossref] [ Google Scholar]
- Ambe PC, Kugler CM, Breuing J, Grohmann E, Friedel J, Hess S. The effect of preoperative stoma site marking on risk of stoma-related complications in patients with intestinal ostomy - a systematic review and meta-analysis. Colorectal Dis 2022; 24(8):904-17. doi: 10.1111/codi.16118 [Crossref] [ Google Scholar]
- Roat-Shumway S, Tonelli C, Singer M, Cohn T, Luchette FA, Abdelsattar Z. Is local excision an appropriate treatment modality in patients presenting with early-stage (cT1 N0 M0) rectal adenocarcinoma? Surgery 2023; 173(3): 665-73. Is local excision an appropriate treatment modality in patients presenting with early-stage (cT1 N0 M0) rectal adenocarcinoma? Surgery 2023; 173(3):665-73. doi: 10.1016/j.surg.2022.08.040 [Crossref] [ Google Scholar]
- Xu S, Tan X, Ma C, McElyea RS, Shieh K, Stover AM. An eHealth symptom and complication management program for cancer patients with newly created ostomies and their caregivers (Alliance): a pilot feasibility randomized trial. BMC Cancer 2023; 23(1):532. doi: 10.1186/s12885-023-10919-x [Crossref] [ Google Scholar]
- Trinder MW, Clifford M, Jones AL, Shepherd T, Jacob AO. The impact of sarcopenia on outcomes in patients with inflammatory bowel disease undergoing colorectal surgery. ANZ J Surg 2022; 92(3):397-402. doi: 10.1111/ans.17439 [Crossref] [ Google Scholar]
- Haraldstad K, Wahl A, Andenæs R, Andersen JR, Andersen MH, Beisland E. A systematic review of quality of life research in medicine and health sciences. Qual Life Res 2019; 28(10):2641-50. doi: 10.1007/s11136-019-02214-9 [Crossref] [ Google Scholar]
- Coulter A, Oldham J. Person-centred care: what is it and how do we get there? Future Hosp J 2016; 3(2): 114-6. what is it and how do we get there? Future Hosp J 2016; 3(2):what is it and how do we get there? Future Hosp J 2016; 3(2). doi: 10.7861/futurehosp.3-2-114 [Crossref] [ Google Scholar]
- Zeydani A, Atashzadeh-Shoorideh F, Hosseini M, Zohari-Anboohi S. Community-based nursing: a concept analysis with Walker and Avant’s approach. BMC Med Educ 2023; 23(1):762. doi: 10.1186/s12909-023-04749-5 [Crossref] [ Google Scholar]
- Zewude WC, Derese T, Suga Y, Teklewold B. Quality of life in patients living with stoma. Ethiop J Health Sci 2021; 31(5):993-1000. doi: 10.4314/ejhs.v31i5.11 [Crossref] [ Google Scholar]
- Dabirian A, Yaghmaei F, Rassouli M, Zagheri Tafreshi M. Quality of life in ostomy patients: a qualitative study. Patient Prefer Adherence 2010; 5:1-5. doi: 10.2147/ppa.S14508 [Crossref] [ Google Scholar]