Journal of caring sciences. 14(2):127-134.
doi: 10.34172/jcs.025.33659
Original Article
Development of the Spiritual Distress Scale for Patients with Chronic Non-communicable Diseases in Thailand
Yuttachai Chaiyasit Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing, 1, * 
Khwanprapat Chanbunlawat Conceptualization, Data curation, Investigation, Resources, Supervision, Validation, Visualization, Writing – original draft, 2
Author information:
1Department of Pediatric and Adolescent Nursing, Ubon Ratchathani University, Ubon Ratchathani, Thailand
2Department of Adult and Gerontological Nursing, Faculty of Nursing, Ubon Ratchathani Rajabhat University, Ubon Ratchathani, Thailand
Abstract
Introduction:
A spiritual distress scale for Thai patients with chronic non-communicable diseases (SDS-Thai-NCDs) has not yet been developed. This study aimed to develop and evaluate its psychometric properties.
Methods:
A methodological approach was applied to develop and verify the quality of the scale through seven steps: defining concepts, formatting the scale, creating items, expert review, item selection, field testing, and psychometric property testing. The sample included 400 Thai patients with chronic NCDs from eight provinces, representing all regions of Thailand. The scale’s quality was assessed through content validity, discrimination index, reliability, and exploratory factor analysis.
Results:
Initially, the scale contained 48 items, which were reduced to 46 items after expert review, with a content validity index of 0.97. Item analysis and selection revealed 43 items that met the criteria, with corrected item-total correlations greater than 0.30 and discrimination indices ranging from 0.336 to 0.906. The scale demonstrated excellent internal consistency, with a Cronbach’s alpha coefficient of 0.986. During the field test and psychometric property testing, the 43 items were grouped into five factors, with eigenvalues ranging from 3.494 to 8.385, explaining 70.80% of the variance. The five factors identified were: Loss of self-esteem, meaning, and purpose of life; Loss of relationships with oneself and others; Loss of hope and inner strength; Loss of relationship with nature and a higher power; and Physical expression.
Conclusion:
The SDS-Thai-NCDs is an effective tool for assessing spiritual distress and can be used in clinical practice or research to guide interventions aimed at alleviating spiritual distress among patients with chronic NCDs.
Keywords: Spiritual distress, Scale development, Psychometrics, Chronic non-communicable diseases, Thai patients
Copyright and License Information
© 2025 The Author(s).
This work is published by Journal of Caring Sciences as an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/). Non-commercial uses of the work are permitted, provided the original work is properly cited.
Funding Statement
This study was funded by Thailand Science, Research, and Innovation.
Introduction
Chronic non-communicable diseases (NCDs) have had a profound impact on healthcare systems worldwide, including in Thailand. Major behavioral risk factors contributing to NCDs include tobacco use, harmful alcohol consumption, physical inactivity, and chronic stress.1 Each year, 41 million people worldwide are affected by chronic NCDs. Among these, 15 million patients are between the ages of 30 to 69 years. The three leading causes of death from NCDs are cardiovascular disease, cancer, and diabetes, affecting 18, 9 and 4 million people annually, respectively.1,2In Thailand, the five most prevalent chronic NCDs that cause illness and premature death are hypertension, diabetes mellitus, cardiovascular diseases, cerebrovascular disease, and chronic obstructive pulmonary disease.3
Chronic NCDs affect various dimensions of health, including social, psychological, and particularly spiritual dimensions due to the complexity, prolongation, and incurability of these diseases. Patients with chronic NCDs often experience loss of self-esteem, loss of self-control, loss of meaning and purpose in life, hopelessness, uncertainty, loss of relationships, and fear of death, all of which contribute to spiritual distress.4,5 Research indicates that the rate of spiritual distress among patients with chronic illnesses, particularly those with severe illnesses, cancer patients undergoing chemotherapy or radiotherapy, patients with stigmatized diseases such as HIV/AIDS, and those nearing the end of their lives, has been reported to range from 17.4% to 73.1%.6-8
Spiritual distress occurs when a person’s value system and beliefs are disrupted or conflicted.5,8,9 This distress diminishes their capacity to handle problems and illness. It encompasses six dimensions: physical expression, psychological expression, lack of love and relationships with self, others, nature, and a higher power or God, lack of self-esteem, lack of meaning and purpose in life, and lack of inner strength.5,9
However, existing spiritual distress scales (SDSs) have several limitations. Most scales have been developed within Western sociocultural contexts, limiting their applicability to other regions, such as Thailand, where cultural and religious beliefs significantly influence the experience of spiritual distress. Furthermore, many of these tools fail to capture all six key dimensions of spiritual distress. For example, the SDS developed by Ku et al,10 for cancer patients in Taiwan includes only four domains: relationship with self, others, God, and attitude toward death. While it provides valuable insights, it does not address aspects like inner strength or relationships with nature, which may be particularly relevant in non-Western contexts. Similarly, a tool developed by Monod et al, for hospitalized elderly patients divides spiritual distress into four dimensions: meaning, transcendence, values, and psychosocial identity.11 While this tool is helpful, it does not fully reflect the complex and multi-dimensional nature of spiritual distress that can be experienced by chronic NCD patients.
Given these limitations, particularly the absence of a culturally relevant and comprehensive tool for Thai patients with chronic NCDs, there is a clear need for a new, standardized instrument. Such a tool would be tailored to the Thai sociocultural context, reflecting local beliefs and values, and would capture all six dimensions of spiritual distress. This tool could significantly benefit healthcare professionals, especially nurses, by helping them assess and address the spiritual distress of patients with chronic NCDs. Furthermore, it could serve as a foundation for future research on spiritual distress across diverse patient groups, enhancing our understanding of this important aspect of health and well-being. So, this study aimed to develop spiritual distress scale for Thai patients with chronic non-communicable diseases (SDS-Thai-NCDs) and evaluate its psychometric properties.
Materials and Methods
There are seven steps in the development and verification process of the SDS-Thai-NCDs12,13(Figure 1).
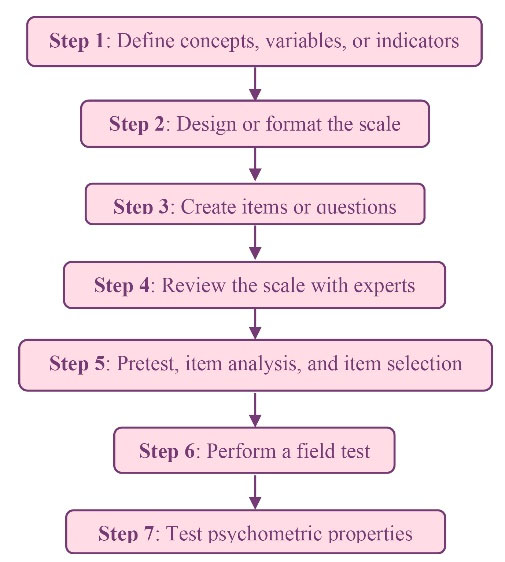
Figure 1.
The seven steps of the development and validation of the SDS-Thai-NCDs
.
The seven steps of the development and validation of the SDS-Thai-NCDs
Define concepts, variables, or indicators: In this step, the researcher conducted a literature review of both Thai and English articles using the keywords “spiritual distress,” “chronic illness and spiritual distress,” and “patients and spiritual distress” from PubMed, Science Direct, Elsevier, CINAHL, Google Scholar, ThaiLIS, and TCI. Thirteen articles related to the concepts and concept analysis were reviewed to identify the characteristics of spiritual distress, which would later be used to create questions in the next step. Six dimensions and forty-eight indicators of spiritual distress were identified: 1) physical expression; 2) psychological expression; 3) lack of love and relationships with self, others, nature, and a higher power or God; 4) lack of self-esteem; 5) lack of meaning and purpose in life; and 6) lack of inner strength.5,6,8,9,14-18
Design or format the scale: A five-point Likert scale was applied to the study, with the following response options: strongly agree (5 points), agree (4 points), neutral (3 points), disagree (2 points), and strongly disagree (1 point). A low score indicates a low level of spiritual distress, while a high score indicates a high level of spiritual distress.
Create items or questions: The researcher developed questions that align with the definition of spiritual distress, divided into six dimensions, for a total of 48 questions: 1) physical expression, 4 items (items 1-4) 2) psychological expression, 5 items (items 5–9) 3) loss of love and relationships, 15 items (items 10–24) 4) loss of self-esteem, 10 items (items 25–34) 5) loss of meaning and purpose in life, 9 items (items 35–43), and 6) loss of inner strength, 5 items (items 44–48).
Review the scale with experts: The scale was evaluated for content validity by five experts: a nursing lecturer specializing in adult nursing care, a nursing lecturer specializing in mental health and psychiatric nursing care, a nursing lecturer with expertise in research methodology and instrument development, a nurse expert in caring for patients with chronic NCDs, and a nurse expert in spiritual care. Content validity was assessed using the content validity index (CVI), where the CVI for each item was calculated by counting the number of experts who rated the item as 3 (minor revisions needed) or 4 (representative). An item was considered valid if its CVI value was greater than 0.70 or 0.80.12,13 For each item, items that received a rating of 1 or 2 points (from more than three experts) were discussed by the research team for potential selection or deletion. Items with a rating of 3 or 4 points (from at least three experts) were discussed for refinement or preservation.
Pretest, item analysis, and item selection: In this step, the scale was tested in a pilot study with thirty patients with NCDs to assess its discrimination power and internal consistency. Questions with a corrected item-total correlation value of 0.30 or higher were considered good questions and selected for inclusion in the scale.
Perform a field test: The researchers used the pre-tested SDS to collect data from a large sample of 400 patients with NCDs (see Table 1).
Test psychometric properties:In this step, the scale was evaluated using exploratory factor analysis to assess its psychometric properties.
The inclusion criteria for participants were as follows: 1) patients diagnosed with chronic NCDs, for example, hypertension, diabetes mellitus, cardiovascular disease, cerebrovascular disease, and chronic obstructive pulmonary disease; 2) Either male and female; 3) Aged over 20 years; 4) Residing in one of the eight selected provinces at eight Subdistrict Health Promoting Hospitals, covering all four regions of Thailand; 5) Consciousness and able to communicate effectively; and 6) willing to participate in the study. The sample size was calculated using the guideline of 5–10 participants per item for exploratory factor analysis.12,13 Given that the scale included 43 items, the required sample size ranged from 215 to 430 participants. Ultimately, 400 participants were included in the study.
A multi-stage random sampling method combined with stratified random sampling was employed, taking into account the distribution of chronic NCD cases across the study sites. The sampling procedure included the following steps:
The study area is divided into four regions according to the spatial division of Thailand, consisting of the northern region (17 provinces), northeastern region (20 provinces), central region (26 provinces), and southern region (14 provinces).
Two provinces were randomly selected from each region: Phayao, Phitsanulok, Lopburi, Chachoengsao, Nakhon Phanom, Ubon Ratchathani, Songkhla, and Narathiwat.
Two districts were randomly selected from each selected province: Pong, Wangthong, Pattananikom, Pranomsarakarm, That Phanom, Muang Ubon Ratchathani, Ranod, and Muang Narathiwat.
Two subdistrict health-promoting hospitals were selected from each district: Oi, Kangsopa, Deelung, Koh kanoon, Nathon, Nong Khon, Klongdan, and Kokkien.
A simple random sampling was used according to the proportion of the population of patients with chronic NCDs in each research area that met the inclusion criteria. (Table 1)
This research was approved by the Ethics Committee of Ubon Ratchathani Rajabhat University [EC number HE651011]. Registered nurses at a sub-district hospital for health promotion sent invitations to the participants based on the inclusion criteria. The participants were then given information regarding the goals and methods of the study, as well as its benefits and risks. They gave their consent and were given the option to participate in the study at any time after enrolling. Participants then completed the questionnaire within 15-30 minutes. A researcher was present to provide additional clarification for participants who had difficulty reading or understanding the items
Data were collected between May to August 2023.
Descriptive statistics, including frequency, percentage, mean, and standard deviation, were used to analyze participants’ socioeconomic and demographic characteristics. The scale’s quality was evaluated through content validity, item discrimination index, reliability testing, and exploratory factor analysis.
Results
Socio-economic and Demographic Profile of patients with NCDs
The majority of the sample were female, 73.25%, average age 61.09 years (SD = 10.24), Buddhist 71.50%, primary education 67.25%, married status 63.50%, not working 28.00%, average monthly income 4729.63 baht/month (SD = 4644.50), sufficient income, no savings 38%, hometown Narathiwat 28.50%, diagnosed with diabetes mellitus 50%, average duration of illness 8.43 years (SD = 5.98) as shown in Table 2.
Results of Verifying the Quality of the SDS-Thai-NCD
The original SDS-Thai-NCDs had 48 items rated on a five Likert scale (strongly agree = 5, agree = 4, neutral = 3, disagree = 2, strongly disagree = 1), where higher scores indicate greater spiritual distress. Based on expert recommendations, the number of items was reduced to 46. The overall content validity index (CVI) was 0.970.
Item analysis was used to determine internal consistency and select items with corrected item correlation values above 0.30 with 30 patients with NCDs. The results found that there were 43 out of 46 items with a corrected item correlation above 0.3, which was 0.336–0.906.
The Cronbach’s alpha coefficient for the initial version (n = 30) was 0.981, and for the final version with 400 participants, it was 0.986, indicating excellent internal consistency.
An exploratory factor analysis was conducted. Bartlett’s test of sphericity statistic was statistically significant (χ2 = 17356.399, df = 903, P = 0.000), and the Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy was 0.966. The 43 questions could be organized into 5 factors by using exploratory factor analysis with principal component analysis (PCA) and Varimax rotation, orthogonal component method with an Eigen value of 3.494–8.385, explaining 70.80% of the variance. The criterion for keeping an item on a scale after factor analysis involves assessing factor loadings. A common threshold is a factor loading greater than 0.30, as items with lower loadings may not contribute meaningfully to the factor and may be removed. All items had factor loadings greater than 0.30. Items with cross-loadings were addressed by assigning each item to the factor with the highest loading, ensuring that the content of the item aligned with the respective factor19 (For examples, items 19, 20, and 35).The five factors extracted were: 1) Loss of self-esteem, meaning, and purpose of life (Eigenvalue = 8.385; 19.50% of the variance); 2) Loss of relationships with oneself and others (Eigenvalue = 7.033; 16.36% of the variance); 3) Loss of hope and inner strength (Eigenvalue = 6.209; 14.44% of the variance; 4) Loss of relationship with nature and a higher power (Eigenvalue = 5.323; 12.38% of the variance); and 5) Physical expression (Eigenvalue = 3.494; 8.13% of the variance) (see Figure 2 andTable 3).
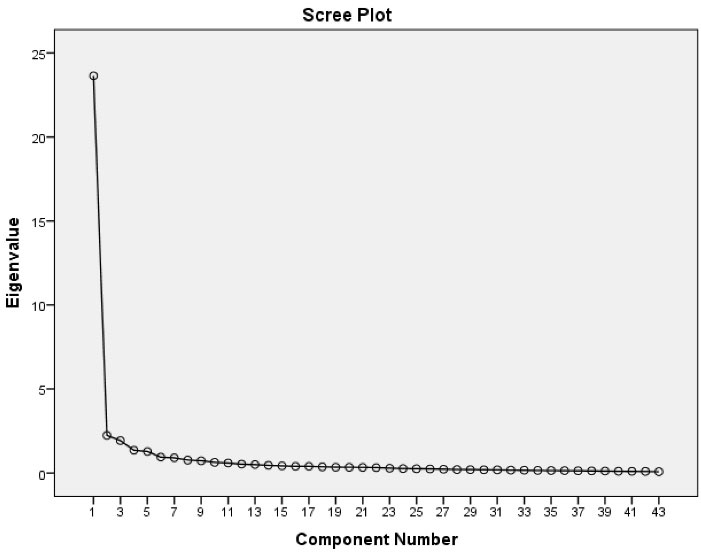
Figure 2.
A scree plot of the SDS-Thai-NCD; five factors, with eigenvalue greater than 1 and factor loading ≥ 0.30 were identified
.
A scree plot of the SDS-Thai-NCD; five factors, with eigenvalue greater than 1 and factor loading ≥ 0.30 were identified
Table 1.
Population and samples based on the regions
|
Region
|
Province
|
District
|
Sub-district
|
Population
|
Samples
|
| North |
Phayao |
Pong |
Oi |
556 |
31 |
| Phitsanulok |
Wangthong |
Kangsopa |
604 |
33 |
| Central |
Lopburi |
Pattananikom |
Deelung |
613 |
34 |
| Chachoengsao |
Pranomsarakarm |
Koh kanoon |
1.696 |
94 |
| Northeast |
Nakhon Phanom |
That Phanom |
Nathon |
601 |
33 |
| Ubon Ratchathani |
Muang |
Nong Khon |
827 |
45 |
| South |
Songkhla |
Ranod |
Klongdan |
294 |
16 |
| Narathiwat |
Muang |
Kokkien |
2.088 |
114 |
| Overall |
|
|
|
7.279 |
400 |
Table 2.
Socio-economic and demographic profile of patients with NCDs(n = 400)
|
Variables
|
N (%)
|
| Gender |
|
| Male |
107 (26.75) |
| Female |
293 (73.25) |
| Age (years), mean (SD) |
61.09 (10.24) |
| Religion |
|
| Buddhist |
286 (71.50) |
| Muslim |
111 (27.75) |
| Christian |
3 (0.75) |
| Educational level |
|
| None |
31 (7.75) |
| Primary |
269 (67.25) |
| Junior high school |
44 (11.00) |
| High school |
34 (8.50) |
| Diploma |
8 (2.00) |
| ≥ University |
14 (3.50) |
| Marital status |
|
| Single |
36 (9.00) |
| Married |
254 (63.50) |
| Divorced |
110 (27.50) |
| Occupation |
|
| None |
112 (28.00) |
| Agriculture |
101 (25.25) |
| Labor |
97 (24.25) |
| Merchant |
57 (14.25) |
| Retired |
6 (1.50) |
| Others |
27 (6.75) |
| Monthly income (Thai Baht), mean (SD) |
4729.63 (4644.50) |
| Sufficient payment |
|
| Sufficient/saving |
45 (11.25) |
| Sufficient/no saving |
152 (38.00) |
| Insufficient/no debt |
99 (24.75) |
| Insufficient/had debt |
104 (26.00) |
| Province |
|
| Phayao |
31 (7.75) |
| Phitsanulok |
33 (8.25) |
| Lopburi |
34 (8.50) |
| Chachoengsao |
94 (23.50) |
| Nakhon Phanom |
33 (8.25) |
| Ubon Ratchathani |
45 (11.25) |
| Songkhla |
16 (4.00) |
| Narathiwat |
114 (28.50) |
| Chronic NCDs (Be allowed to select more than one) |
| Hypertension |
87 (21.75) |
| Diabetes mellitus |
200 (50.00) |
| Cardiovascular disease |
6 (1.50) |
| Cerebrovascular disease |
17 (4.25) |
| Chronic obstructive pulmonary disease |
3 (0.75) |
| Others |
66 (16.50) |
| Duration of illness (years), mean (SD) |
8.43 (5.98) |
Table 3.
Results of exploratory factor analysis using the orthogonal component method by the Varimax method
|
|
Items
|
|
|
Component
|
|
|
1
|
2
|
3
|
4
|
5
|
| 1 |
I couldn't get to sleep or stay asleep because of my illness. |
0.057 |
0.186 |
0.017 |
0.130 |
0.740 |
| 2 |
My illness makes me physically tired. |
0.174 |
0.087 |
0.213 |
0.072 |
0.760 |
| 3 |
My illness makes me lose my appetite. |
0.233 |
0.295 |
0.180 |
0.089 |
0.695 |
| 4 |
My illness makes me feel uncomfortable and restless. |
0.202 |
0.358 |
0.243 |
0.100 |
0.663 |
| 5 |
I'm afraid because of my illness. |
0.273 |
0.545 |
0.220 |
0.106 |
0.432 |
| 6 |
I feel angry at myself for being sick. |
0.318 |
0.627 |
0.236 |
0.095 |
0.362 |
| 7 |
My illness makes me cry. |
0.358 |
0.698 |
0.192 |
0.084 |
0.268 |
| 8 |
I feel about my illness. |
0.248 |
0.684 |
0.224 |
0.098 |
0.222 |
| 9 |
My illness makes me feel alone. |
0.334 |
0.716 |
0.200 |
0.242 |
0.169 |
| 10 |
My illness reduces my relationship with others. |
0.381 |
0.651 |
0.241 |
0.238 |
0.143 |
| 11 |
I feel unsupported by others. |
0.285 |
0.628 |
0.195 |
0.380 |
0.153 |
| 12 |
My illness makes me feel abandoned. |
0.236 |
0.600 |
0.257 |
0.418 |
0.150 |
| 13 |
My illness makes me worry about my family. |
0.230 |
0.615 |
0.245 |
0.278 |
0.221 |
| 14 |
The illness has made me feel like I've lost my love. |
0.185 |
0.667 |
0.191 |
0.414 |
0.114 |
| 15 |
My illness makes me confused in my relationships with other people. |
0.171 |
0.593 |
0.260 |
0.471 |
0.128 |
| 16 |
My illness makes me feel abandoned by the Holy Spirit/higher power/God. |
0.118 |
0.471 |
0.265 |
0.664 |
0.157 |
| 17 |
My illness makes me feel angry toward the Holy Spirit/higher power/God. |
0.249 |
0.259 |
0.273 |
0.765 |
0.106 |
| 18 |
My illness makes me feel punished by the Holy Spirit/higher power/God. |
0.282 |
0.240 |
0.328 |
0.743 |
0.094 |
| 19 |
My illness reduces my interest in nature and my surroundings. |
0.453 |
0.225 |
0.141 |
0.465 |
0.187 |
| 20 |
My illness is caused by my karma/destiny. |
0.472 |
0.094 |
-0.087 |
0.411 |
0.346 |
| 21 |
My illness causes a loss of faith/higher power/God. |
0.316 |
0.202 |
0.324 |
0.710 |
0.116 |
| 22 |
My illness deprives me of my spiritual and religious practices. |
0.405 |
0.234 |
0.353 |
0.653 |
0.060 |
| 23 |
My illness makes me feel self-blamed and guilty. |
0.668 |
0.241 |
0.243 |
0.327 |
0.186 |
| 24 |
My illness causes me to lose my self-worth. |
0.662 |
0.225 |
0.197 |
0.329 |
0.247 |
| 25 |
My illness makes me lose my role. |
0.727 |
0.263 |
0.211 |
0.270 |
0.153 |
| 26 |
My illness makes me a burden to others. |
0.722 |
0.301 |
0.276 |
0.108 |
0.100 |
| 27 |
My illness makes me lose my confidence. |
0.722 |
0.294 |
0.360 |
0.123 |
0.175 |
| 28 |
My illness makes me lose self-control. |
0.598 |
0.312 |
0.427 |
0.154 |
0.200 |
| 29 |
My illness makes me lose my self-image. |
0.690 |
0.356 |
0.331 |
0.164 |
0.101 |
| 30 |
My illness makes me lose my dignity. |
0.631 |
0.340 |
0.311 |
0.337 |
0.033 |
| 31 |
My illness makes me lose my identity. |
0.676 |
0.360 |
0.322 |
0.254 |
0.075 |
| 32 |
My illness makes me question the meaning and purpose of life. |
0.642 |
0.168 |
0.298 |
0.183 |
0.223 |
| 33 |
My illness makes me lose the meaning and purpose of life. |
0.671 |
0.209 |
0.356 |
0.231 |
0.192 |
| 34 |
I have a question about my illness. |
0.548 |
0.241 |
0.441 |
0.224 |
0.221 |
| 35 |
I can't accept the illness or what happened. |
0.421 |
0.334 |
0.465 |
0.365 |
0.038 |
| 36 |
I feel uncertain about my future life, death, and the afterlife. |
0.300 |
0.133 |
0.669 |
0.255 |
0.189 |
| 37 |
My illness makes me feel like my life is empty and pointless. |
0.322 |
0.228 |
0.666 |
0.424 |
0.112 |
| 38 |
My illness makes me feel lacking in creativity. |
0.452 |
0.327 |
0.586 |
0.219 |
0.249 |
| 39 |
My illness makes me feel hopeless. |
0.340 |
0.319 |
0.717 |
0.217 |
0.181 |
| 40 |
My illness makes me suffer. |
0.449 |
0.387 |
0.630 |
0.199 |
0.116 |
| 41 |
My illness makes me not feel at peace. |
0.355 |
0.278 |
0.672 |
0.205 |
0.248 |
| 42 |
My illness makes me lose my courage. |
0.342 |
0.323 |
0.657 |
0.333 |
0.130 |
| 43 |
My illness makes me lose my inner strength. |
0.301 |
0.296 |
0.714 |
0.315 |
0.165 |
|
|
Eigen value |
8.385 |
7.033 |
6.209 |
5.323 |
3.494 |
|
|
Variance explained |
19.499 |
16.357 |
14.440 |
12.378 |
8.125 |
Discussion
Initially, the scale contained 48 items, which were reduced to 46 items after expert review, resulting in a content validity index of 0.97. This indicates that the scale has high content validity, suggesting that the items are relevant and representative of the construct being measured. Generally, a content validity index greater than 0.70-0.80 is considered acceptable.12,13,20 Additionally, item analysis and selection revealed 43 items that met the criteria, with corrected item-total correlations greater than 0.3012,13,21 and discrimination indices ranging from 0.336 to 0.906. The Cronbach’s alpha coefficient was 0.986, indicating excellent internal consistency, and the scale can be used as a reliable measure. A Cronbach’s alpha value greater than 0.70 is generally considered acceptable for reliability.12,13
An exploratory factor analysis found that Bartlett’s test of sphericity statistic was statistically significant (χ2 = 17356.399, df = 903, P = 0.000), and the KMO measure of sampling adequacy was 0.966, supporting the adequacy of the sample for factor analysis.12,13,22 PCA with varimax rotation revealed that the 43 items were grouped into five factors, with eigenvalues ranging from 3.494 to 8.385, explaining 70.80% of the variance. All items had factor loadings greater than 0.30. Cross-loadings were addressed by assigning each item to the factor with the highest loading, ensuring that the content of the item aligned with the respective factor19 (items 19, 20, and 35). This indicates that the scale is well-structured and effectively captures the underlying dimensions of spiritual distress. The exploratory factor analysis revealed five underlying dimensions of spiritual distress, each representing a distinct thematic cluster, as follows: 1) Loss of self-esteem, meaning, and purpose of life; 2) Loss of relationships with oneself and others; 3) Loss of hope and inner strength; 4) Loss of relationship with nature and a higher power; and 5) Physical expression.
Factor 1: Loss of self-esteem, meaning, and purpose of life; eigenvalue 8.385, explaining 19.499% of the variance. Questions within this component reflect the loss of self-esteem, meaning, and purpose of life. This aligns with the concept analysis of spiritual distress by Chaiyasit et al and Chaiyasit & Paiboonrungroj indicate that the loss of self-esteem, meaning, and purpose of life is one of the main attributes of spiritual distress.5,9The main characteristics consistent with the questions above include self-blame, guilt, loss of value, loss of role, feeling of being a burden to others, loss of confidence, loss of self-control, loss of image, loss of dignity, loss of identity, and loss of meaning and purpose in life.5,8,9,14,17,18
Factor 2: Loss of relationships with oneself and others; eigenvalue 7.033, explaining 16.357% of the variance. Questions within the component reflect the loss of relationships with oneself and others. This aligns with the concept analysis of spiritual distress by Chaiyasit et al and Chaiyasit & Paiboonrungroj indicate that loss of relationships with oneself and others is one of the main attributes of spiritual distress.5,9 The main characteristics consistent with the questions above include feeling afraid, angry at oneself, crying, sadness, loneliness, a lack of relationships with others, lack of support from others, feeling abandoned, worrying about family, lost love, and confusion in relationships with others.5,8,9,14,17,18
Factor 3: Loss of hope and inner strength; eigenvalue 6.209, explaining 14.440 % of the variance. Questions within the component reflect the loss of hope and inner strength. This aligns with the concept analysis of spiritual distress by Chaiyasit et al and Chaiyasit & Paiboonrungroj indicate that loss of hope and inner strength is one of the main attributes of spiritual distress.5,9 The main characteristics consistent with the questions above include inability to accept illness, worrying about the future, death, and the afterlife, feeling empty, lack of creativity, hopelessness, mental suffering, lack of mental peace, loss of courage, and loss of confidence strong mental resilience.5,8,9,14,17,18
Factor 4: Loss of relationship with nature and a higher power; eigenvalue 5.323, explaining 12.378% of the variance. Questions within the component reflect the loss of relationship with nature and a higher power. This aligns with the concept analysis of spiritual distress by Chaiyasit et al and Chaiyasit & Paiboonrungroj indicate that loss of relationship with nature and a higher power is one of the main attributes of spiritual distress.5,9 The main characteristics consistent with the questions above include feeling abandoned, feeling angry, feeling punished by a holy being, higher power, or God, decreased interest in nature and surroundings.5,8,9,14,17,18
Factor 5: Physical expression; eigenvalue 3.494, explaining 8.125% of the variance. Questions within the component reflect physical expression. This aligns with the concept analysis of spiritual distress by Chaiyasit et al and Chaiyasit & Paiboonrungroj indicate that physical expression is one of the main attributes of spiritual distress.5,9The main characteristics consistent with the questions above include insomnia, physical fatigue, loss of appetite, feeling unwell, and restlessness.5,8,9,14,17,18
However, some of the results are not consistent with the conceptual framework of the study. “Lack of self-esteem” and “lack of meaning and purpose in life” were integrated into Dimension 1: Loss of self-esteem, meaning, and purpose in life. This integration is based on the idea that having a sense of purpose and meaning in life enhances one’s self-esteem.23 Moreover, “lack of love and relationship with oneself, others, nature, and a higher power or God” was divided into two dimensions: Dimension 2: Loss of relationship with oneself and others, and Dimension 4: Loss of relationship with nature and a higher power. This division is based on the distinction between horizontal relationships (with oneself and others) and vertical relationships (with nature and a higher power).5,24
Additionally, psychological expression was integrated into Dimension 2: Loss of relationship with oneself and others. The items related to psychological expression could be appropriately included in this dimension. Meanwhile, “lack of inner strength” was modified to Dimension 3: Loss of hope and inner strength, as some items in this dimension reflect aspects of hope. On the other hand, physical expression remained unchanged and was allocated to Dimension 5.
This study, conducted among patients with NCDs at eight health promotion hospitals in Thailand, has limitations in generalizing the findings to broader populations. The scale used may reflect cultural norms and health perceptions specific to Thailand, limiting its applicability in other cultural or healthcare contexts. Additionally, biases in participant selection, such as the focus on individuals with lower health conditions, could affect the results, especially regarding spiritual distress. Therefore, future research should assess the scale’s psychometric properties across diverse populations and settings, accounting for cultural sensitivity, selection biases, and response tendencies, to ensure broader applicability and validity.
Conclusion
The SDS-Thai-NCDs demonstrated strong content validity and reliability. Five factors accounted for a significant portion of the total variance, including: 1) Loss of self-esteem, meaning, and purpose in life; 2) Loss of relationships with oneself and others; 3) Loss of hope and inner strength; 4) Loss of connection with nature and a higher power; and 5) Physical expression. This scale can be utilized to assess and address spiritual distress in patients with chronic NCDs, thus enhancing patient care through targeted interventions. It offers a valuable tool for research focused on the spiritual dimensions of chronic illness and can be applied in clinical and educational settings. However, the study, conducted among NCD patients in Thailand, has limitations in terms of generalizability due to cultural specificity and potential participant selection biases. Future research should assess the scale’s psychometric properties in diverse populations and settings, taking into account cultural differences, selection biases, and response tendencies, to strengthen its broader applicability and validity.
Acknowledgments
This study was funded by Thailand Science, Research, and Innovation. The authors would like to express their sincere gratitude to all the participants, as well as the staff at the research sites, for their kind cooperation and support.
Competing Interests
The authors declare no competing interests.
Data Availability Statement
The datasets are available from the corresponding author upon reasonable request.
Ethical Approval
The study was approved by the Ethics Committee of Ubon Ratchathani Rajabhat University (Ethical code: HE651011)
Research Highlights
What is the current knowledge?
What is new here?
References
- World Health Organization (WHO). Noncommunicable Diseases. WHO; 2018. Available from: https://www.who.int/news-room/factsheets/detail/Noncommunicable-diseases. Accessed July 28, 2024.
- World Health Organization (WHO). Noncommunicable Diseases Progress Monitor 2020. WHO; 2020. Available from: https://www.who.int/publications/i/item/ncd-progress-monitor-2020. Accessed July 28, 2024.
- Division of Non-Communicable Disease, Ministry of Public Health, Thailand. Number and Rates of NCDs in 2016-2018. 2019. Available from: http://www.thaincd.com/2016/mission/documentsdetail.php?id = 13684&tid = 32&gid = 1-020. Accessed July 28, 2024.
- Promkeawngam S, Namwong A. The spiritual well-being of community-dwelling Thai older people with chronic illness. J Nurs Health Care 2017; 35(3):204-13. [ Google Scholar]
- Chaiyasit Y, Piboonrungroj P. Nursing Cares for Patients with Spiritual Distress. Bangkok: Chaulalongkorn University; 2020.
- Pinho CM, Gomes ET, de Fátima Cordeiro Trajano M, de Almeida E Cavalcanti AT, Andrade MS, Valença MP. Impaired religiosity and spiritual distress in people living with HIV/AIDS. Rev Gaucha Enferm 2017; 38(2):e67712. doi: 10.1590/1983-1447.2017.02.67712 [Crossref] [ Google Scholar]
- Velosa T, Caldeira S, Capelas ML. Depression and spiritual distress in adult palliative patients: a cross-sectional study. Religions 2017; 8(8):156. doi: 10.3390/rel8080156 [Crossref] [ Google Scholar]
- Martins H, Caldeira S. Spiritual distress in cancer patients: a synthesis of qualitative studies. Religions 2018; 9(10):285. doi: 10.3390/rel9100285 [Crossref] [ Google Scholar]
- Chaiyasit Y, Chanbunlawat K, Thong-Orn R, Kaewkerd O. A conceptual analysis of spiritual distress. The Journal of Thailand Nursing and Midwifery Council 2021; 36(2):5-17. [ Google Scholar]
- Ku YL, Kuo SM, Yao CY. Establishing the validity of a spiritual distress scale for cancer patients hospitalized in southern Taiwan. Int J Palliat Nurs 2010; 16(3):134-8. doi: 10.12968/ijpn.2010.16.3.47325 [Crossref] [ Google Scholar]
- Monod SM, Rochat E, Büla CJ, Jobin G, Martin E, Spencer B. The spiritual distress assessment tool: an instrument to assess spiritual distress in hospitalised elderly persons. BMC Geriatr 2010; 10:88. doi: 10.1186/1471-2318-10-88 [Crossref] [ Google Scholar]
- Thato R. Nursing Research: Concepts to Application. 4th ed. Bangkok: Chaulalongkorn University; 2018.
- Tiansawad S. Instrument Development for Nursing Research. Chiang Mai: Siampimnana; 2019.
- Caldeira S, Carvalho EC, Vieira M. Spiritual distress-proposing a new definition and defining characteristics. Int J Nurs Knowl 2013; 24(2):77-84. doi: 10.1111/j.2047-3095.2013.01234.x [Crossref] [ Google Scholar]
- Bhatnagar S, Gielen J, Satija A, Singh SP, Noble S, Chaturvedi SK. Signs of spiritual distress and its implications for practice in Indian Palliative Care. Indian J Palliat Care 2017; 23(3):306-11. doi: 10.4103/ijpc.Ijpc_24_17 [Crossref] [ Google Scholar]
- Gielen J, Bhatnagar S, Chaturvedi SK. Prevalence and nature of spiritual distress among palliative care patients in India. J Relig Health 2017; 56(2):530-44. doi: 10.1007/s10943-016-0252-5 [Crossref] [ Google Scholar]
- Roze des Ordons AL, Sinuff T, Stelfox HT, Kondejewski J, Sinclair S. Spiritual distress within inpatient settings-a scoping review of patients’ and families’ experiences. J Pain Symptom Manage 2018; 56(1):122-45. doi: 10.1016/j.jpainsymman.2018.03.009 [Crossref] [ Google Scholar]
- Schultz M, Meged-Book T, Mashiach T, Bar-Sela G. The cultural expression of spiritual distress in Israel. Support Care Cancer 2018; 26(9):3187-93. doi: 10.1007/s00520-018-4177-2 [Crossref] [ Google Scholar]
- Jordan P, Spiess M. Rethinking the interpretation of item discrimination and factor loadings. Educ Psychol Meas 2019; 79(6):1103-32. doi: 10.1177/0013164419843164 [Crossref] [ Google Scholar]
- Gilbert GE, Prion S. Making sense of methods and measurement: Lawshe’s content validity index. Clin Simul Nurs 2016; 12(12):530-1. doi: 10.1016/j.ecns.2016.08.002 [Crossref] [ Google Scholar]
- Marianti S, Rufaida A, Hasanah N, Nuryanti S. Comparing item-total correlation and item-theta correlation in test item selection: a simulation and empirical study. J Penelit Eval Pendidik 2023; 27(2):133-45. doi: 10.21831/pep.v27i2.61477 [Crossref] [ Google Scholar]
- Hair JF, Black WC, Barbin BJ, Anderson RE. Multivariate Data Analysis. 8th ed. Hampshire, UK: Cengage Learning EMEA; 2019.
- Hosogi M, Okada A, Fujii C, Noguchi K, Watanabe K. Importance and usefulness of evaluating self-esteem in children. Biopsychosoc Med 2012; 6:9. doi: 10.1186/1751-0759-6-9 [Crossref] [ Google Scholar]
- Stoll RI. The essence of spirituality. In: Carson VB, ed. Spiritual Dimensions of Nursing Practice. Philadelphia: WB Saunders Company; 1989. p. 4-23.