Journal of caring sciences. 14(3):151-164.
doi: 10.34172/jcs.025.33683
Original Article
Multi Components in the Implementation of Advanced Care Planning for Patients with Cancer: A Scoping Review
Yodang Yodang Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing, 1, 2 
Erna Rochmawati Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Resources, Project administration, Validation, Visualization, Writing – original draft, Writing – review & editing, 2, 3
Sarah Amalia Data curation, Formal analysis, Investigation, Project administration, Resources, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing, 3
Christantie Effendy Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Resources, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing, 2, 4, *
Author information:
1School of Nursing, Faculty of Science and Technology, Universitas Sembilanbelas November Kolaka, Kolaka Indonesia
2Indonesia Palliative Nurses Association, Sleman, Indonesia
3School of Nursing, Universitas Muhammadiyah Yogyakarta, Bantul, Indonesia
4Department of Medical-Surgical Nursing, Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia
Abstract
Introduction:
Advance care planning (ACP) facilitates patients’ preferences for future treatment. It has been associated with improved quality of end-of-life care. While several factors contribute to ACP implementation, little is known about the specific components involved. This scoping review aimed to identify and explore components of ACP, including knowledge, attitudes, values and beliefs, cultural and ethnic factors in patients with cancer and their families.
Methods:
The scoping review followed the updated Preferred Reporting Items for Systematic Reviews and Meta-Analysis Scoping Review (PRISMA-ScR) 2020 checklist. A search was conducted in the PubMed, Scopus, and Science Direct databases until December 2023, and the selected articles were assessed using the Joanna Briggs Critical Appraisal Tool (MMAT).
Results:
This scoping review included 42 studies. The included studies were grouped by design: quantitative (n=12), qualitative (n=15), and mixed methods (n=15). Key ACP components identified included knowledge and perceptions (n=28), attitudes and behaviours (n=33), values and beliefs (n=26), and cultural and ethnic aspects (n=13).
Conclusion:
This review provides a summary of the crucial components including knowledge and perception, attitudes and behaviors, values and beliefs, and cultural and ethnic perspectives to consider when implementing ACP for patients with cancer.
Keywords: Advance care planning, Advance directive, Cancer, Oncology, Scoping review
Copyright and License Information
© 2025 The Author(s).
This work is published by Journal of Caring Sciences as an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/). Non-commercial uses of the work are permitted, provided the original work is properly cited.
Funding Statement
Not applicable.
Introduction
Advance care planning (ACP) is defined as a formal decision-making process aimed at helping patients make informed decisions about their future care.1 ACP incorporates sharing values and preferences for medical care between the patient and health care professionals (HCPs), also often supplemented with input from and involvement of family or informal carers.2 In recent decades, patient autonomy has become increasingly essential in ACP. Many patients desire to engage in making decisions and extend their autonomy to future care decisions that take effect when they lose capacity or become incapacitated.3 Over time, a more patient-centred approach evolved in medicine, leading to an enhanced involvement of patients in clinical decision-making.4
ACP plays a significant role in addressing palliative care needs and recognizing the end-of-life stage in a timely way,5 particularly for meeting patients’ end-of-life wishes, as an element of comprehensive care including cancer care.6 ACP includes items such as preferred place of care and death, resuscitation policy, treatment limitations and euthanasia directives.5 Furthermore, ACP facilitates patients’ preferences for future treatments, including care intensification and invasive interventions. Considering their beliefs, goals, and perceived quality of life, ACP helps HCPs balance medical decisions with patient-centered care,7 and help prevent family members from the difficult situation of having to guess what kind of care their loved ones would choose.8
In caring for patients with cancer, the ACP has been associated with reduced use of life-sustaining treatments and cancer-directed therapy; fewer hospitalizations and healthcare costs; greater use of hospice services in the last weeks of life; and can lead to more patient-centred care.9 Although the ACP being an important in palliative care for those with cancer, the communication around it can be challenging.10 Further, it was reported that the patient’s and family’s desire and readiness to hear and accept information about prognosis, meanwhile readiness to discuss such things is variable, and was suggested to be reliant upon the values and characteristics of the individual person and family.11 Additionally, including information on patients’ values, beliefs and more general wishes in the advance directives (ADs) as a part of ACP process may be helpful. When the patients are not able to communicate, their families could provide detail information about the patients preferences and make decisions on behalf of the patients.12Thus, it could be challenging for HCPs in providing ACP in regard to various patients and families concerns such as knowledge, attitudes, value and beliefs, culture and ethnic.13 So that the implementation of ACP could differ in each different country all over the world, especially the country which consist multi-ethnics and cultures.14
The growing interest in ACP has resulted in a variety of ACP interventions and programmes,2 and usually used in the context of progressive illness and anticipated deterioration.1 Otherwise, a large variation also still exists in the extent to which ACP documentation takes place,5 and affects the ACP and ADs often are not completed, including those in minorities and with lower education and literacy skills.15 Thus, the HCPs should document care plans and all patient’s wishes in a written advance directive form, and share them with patients, family and team members.15,16
As such of ACP implementation, ADS has been reported that it’s associated with a reduction in aggressive treatments, fewer in-hospital deaths, increased use of hospices, and lower hospital charges. Absence of ADs may lead to unwanted aggressive treatments, which correlates to poor quality of life.8
Despite growing global interest, the implementation of ACP varies significantly across regions and cultural contexts.17 Therefore, this scoping review aims to identify and explore components of ACP, including knowledge, attitudes, values and beliefs, cultural and ethnic factors in patients with cancer and their families. The guiding question is “What are the components of ACP in palliative care intervention among patients with cancer or neoplasms and their families?” This review also aims to provide culturally informed guidance for implementing ACP globally.
Material and Methods
This scoping review was conducted in accordance with the updated PRISMA-ScR 2020 checklist.18
Search Strategy
A comprehensive search was performed in PubMed, Scopus and ScienceDirect databases up to December 2023. Key search terms included “advanced care planning” OR “advance statement” OR “advanced directive planning” OR “end-of-life care planning” AND “cancer” OR “neoplasm” OR “oncology” AND “patient” OR “family”.
English-language articles reporting on the implementation of a multicomponent of advance care planning in palliative care intervention targeting individuals aged 18 years and older with cancer or their family were eligible for this review. Quantitative and qualitative or mixed-method studies that have clear findings from patients or family caregivers were included. We selected studies that discussed aspects of the multicomponent in ACP. We defined a priori a multicomponent aspect that included one or more of the following domains: (1) knowledge, (2) values, (3) attitude and belief (4) culture or ethnicity. Review or protocol were excluded.
Study Selection and Data Abstraction
All abstracts from the initial search were reviewed by 2 reviewers (ER, SA) for possible inclusion in the study. Any uncertainty regarding whether an abstract should be included was brought to the entire group and resolved by discussion. All reviewers (CE, YY, ER, SA) judge the included full-text articles if they meet the study’s eligibility criteria. The reference lists of all retained articles were also reviewed to identify additional potentially eligible articles. For the final set of articles reviewed, data were abstracted independently by two reviewers and then discussed by all reviewers. Disagreements were resolved through discussion. Data from articles that detailed the same intervention were incorporated into 1 unit of analysis rather than separating them.
Study quality was assessed independently by all reviewers using the Joanna Briggs Critical Appraisal Tool for cross-sectional and cohort studies and Mixed Methods Appraisal Tool (MMAT) for mixed-method studies. Any discrepancies were resolved by discussion. The tool assesses the overall study quality in 5 areas: Reporting, external validity, internal validity—control of bias, internal validity— confounding, and power. Studies were extracted based on the following categories: Author and year of publication, study location and setting, study design, population demographic data, and ACP components being discussed.
Results
Data Synthesis and Analysis
The current systematic review included qualitative, quantitative and mixed-method studies, therefore a narrative synthesis was conducted. We conducted thematic analysis to categorise knowledge, attitudes, values and beliefs, cultural and ethnic of the patients with cancer and their families into domains from included studies.
Study Selection
Figure 1 shows the PRISMA flowchart diagram. We identified 12,591 studies for title and abstract screening. After removing 699 duplicates, 11,888 records remained. A total of 11,842 records were excluded because they did not meet the inclusion criteria. Forty-six articles were screened by reading the full-text articles.
Four articles were excluded due to irrelevant populations (e.g., studies including children or a mixed cancer and non-cancer population). In the end, 42 studies were included in the review.
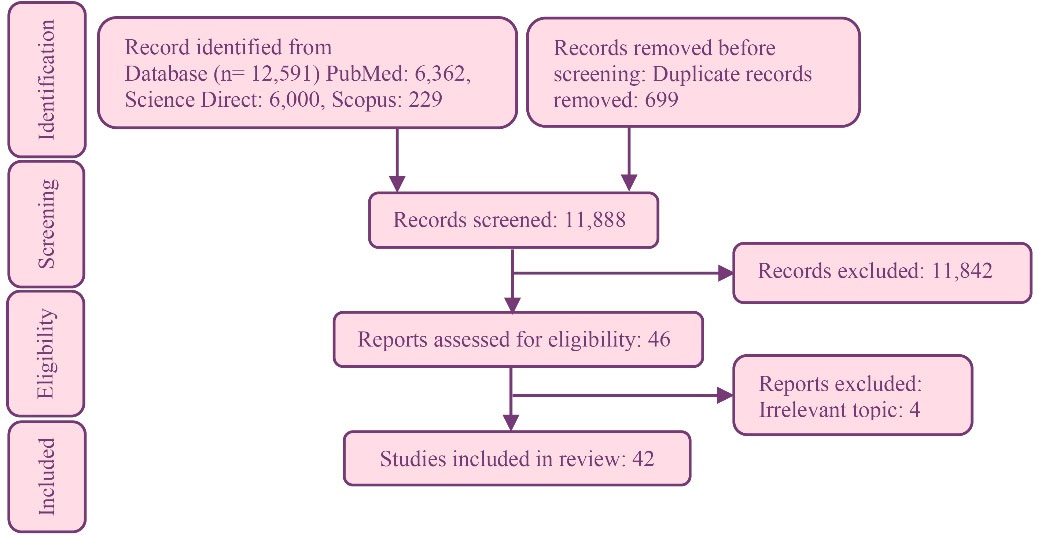
Figure 1.
PRISMA flow chart for study selection
.
PRISMA flow chart for study selection
Characteristics of Included Study
Table 1 shows the characteristics of included studies. The studies included were quantitative (n = 12), qualitative (n = 15) and mixed methods (n = 15). The quality of included studies was high (n = 41) and medium (n = 1). All studies were conducted in high-income countries including the United States of America (n = 14), Canada (n = 2), the United Kingdom (n = 1), Europe (n = 6), China (n = 6), Taiwan (n = 3), South Korea (n = 1), Australia (n = 3), multiple countries (n = 3), Indonesia (n = 1) and Singapore (n = 1). Most studies were conducted in hospital settings and involving patients with cancer. A total of 19,573 patients with life-limiting illness and 4,670 family caregivers were involved in the included studies. All included 42 studies reported perspectives from patients and family caregivers, of which 28 studies reported on knowledge and perceptions; 33 studies on attitudes and behaviours, 26 studies on values and beliefs, and 13 studies on culture and ethnics.
Table 2 Shows synthesis of multiple components of ACP from included study. We group the components into: (1) knowledge and perception; (2) attitude and behaviour; (3) values and belief and (4) cultural aspects and ethnic.
Patients and Family Caregivers’ Knowledge and Perception on ACP
Twenty-eight studies reported patients’ and family caregivers’ knowledge and perceptions on ACP. We synthesised findings into three subcomponents: (1) lack of knowledge and information on ACP; (2) varied perceptions of ACP; and (3) education on ACP and its impacts. The majority of included studies found the knowledge and information of ACP was still considered low both among patients and family members, and which caused reluctance in initiating ACP discussion.37,30 In addition, the lack of knowledge is considered the strongest barrier in initiating ACP discussion,22 although there is an openness and willingness to engage in such discussions.
Findings of a cross-sectional study in the US show that there is an effort to improve knowledge on ACP by providing education via videos, pamphlets.50 In addition, a study from South Korea utilised public promotion and education to facilitate ACP.19 Such efforts have positive impacts, e.g. the change of treatment preference particularly in life-prolonging treatment measures.20 In addition, the provision of ACP resources patients’ discussions on ACP with the physician. Two studies revealed that patients and caregivers prefer to have ACP discussions after being diagnosed.35 However, another study identified that caregivers prefer to have ACP discussions when there is no more treatment or disease recurrence. Participants in the included studies reported that following ACP discussion they prefer comfort care and sought to avoid aggressive treatments.
Patients and Family Caregivers’ Attitudes and Behaviour on ACP
Thirty-three studies discussed patients and family caregivers attitude and behaviour. There are three subcomponents: (1) Openness and acceptance to ACP; (2) factors influencing the decision to engage in ACP discussions; and (3) delayed decisions.55 Abu al Hamayel et al’s study discovered that generally, patients contemplate the importance of considering their end-of-life wishes.39 Moreover, several studies found that the majority of patients can make their own decision regarding end-of-life, although in other studies some patients are influenced by family caregivers in the decision-making. For example, family caregivers from China tend to dominant role in the process of decision-making.
Several factors influence patients and family caregivers in having ACP including the timing of these sensitive discussions, their feelings, and emotions. One study found that more than two-thirds patients think the optimal time to have ACP discussions is after being diagnosed with life-limiting illness.56 Earlier ACP discussion leads to lower rates of aggressive care.31 Three studies discussed the delayed decisions made by patients and family caregivers5,31,43 and summarized that conflicting opinions were one of the main contributing factors.
Table 1.
Characteristics of included studies
|
Author, Year/ Country
|
Setting
|
Method
|
Population
|
Results
|
Park et al19
(2019)/Seoul, Korea |
General hospitals and National cancer centre |
Cross-sectional study |
1001 Cancer patients and 1006 family caregivers |
Public promotion efforts and education regarding ACP were the most important means for facilitating ACP.
One-third of cancer patients and family caregivers were aware AD. |
Berkowitz et al6
(2021)/USA |
Community-based and academic PC practices |
Retrospective cross- sectional study |
1,604 Patients with cancer and 1,094 patients without cancer |
Patients with cancer still had not identified a healthcare proxy. to assist with conversations and documentation, using decision aids and education tools with patients (eg, videos or pamphlets), and implementing electronic reminders to address ACP |
Ermers et al5
(2019)/Nijmegen, The Netherlands |
General practices |
Retrospective cohort study |
163 Deceased patients with colorectal or lung cancer |
Lack of documentation disadvantages continuity of care and could be improved by using predictable, homogeneous and exchangeable formats to document ACP.
ACP is mainly discussed in the last 3 months of life, showing that the conversation on ACP is initiated late. |
Garrido et al20
(2014)/USA |
Out-patient clinic |
Quantitative study |
606 Patients (437 non-Latino White, 93 Black, 76 Latino) with advanced cancer |
The development of interventions that educate patients about the benefits and risks of specific life-prolonging treatments so that patients with advanced cancer are equipped to clarify when they would and would not want a given treatment.
Treatment preferences often change after education on the risks and benefits involved in life-prolonging treatment measures |
Hu et al21
(2021)/Wuhan, China |
Hospital |
Cross-sectional study |
258 Lung cancer patients |
There were 77.5% of patients who regarded hospice care important. One hundred and sixty (60%) patients wanted to make EOL decisions on their own. However, only 10.1% of patients were familiar with AD. |
McDonald et al22
(2017)/Ontario, Canada |
The Cancer Centre’s Chemotherapy Day Unit |
Quantitative survey |
193 Cancer patients |
Lack of knowledge as the strongest barrier to completing an AD (identified as a strong barrier by 50 % of those surveyed). Procrastination was also identified by many as a strong barrier (46 % of those surveyed). many patients hold misperceptions about medical interventions and care at the end of life |
Xing et al23
(2017)/China |
The Oncology Department |
Quantitative study |
412 Adult cancer patients |
Nearly all the patients deciding on their own AD knew their entire situation, including diagnosis and prognosis. Patients with less knowledge of the modern world (i.e., those not living in cities or with lower educational level) tended to end anti-cancer therapy against the recommendation of the oncologist. |
Falzarano et al24
(2021)/USA |
Medical and cancer center |
Longitudinal cohort study |
98 Dyads patient and caregivers |
Advance directive completion may help facilitate terminal illness acknowledgment, making patients more cognizant of planning and coming to terms with their own death. In fact, cognitive acceptance has been associated with DNR order completion and plays a fundamental role in end-of-life decision-making and care. |
McMahan et al25
(2013)/California, US |
General hospital and Veteran Affairs Medical center |
Qualitative study |
38 Patients and 31 surrogates |
The inadequacies of ADs saying that the ‘‘hypothetical situations’’ often used in ADs did not prepare them to face the uncertainty of ‘‘real’’ complex medical decision making. Most participants also stated that focusing on specific treatment preferences, such as ‘‘the DNR’’ (Do Not Resuscitate), was not enough to help make the ‘‘many decisions’’ with which they were faced, stating, |
van Eechoud et al26
(2014)/Flanders, Belgium |
The acute geriatric
ward, the medical oncology ward, and the palliative care unit |
Qualitative methodology, with constructivist grounded theory |
21 Family members |
Several family members, mainly spouses, lacked accurate knowledge about ACP. They either had never heard of or thought about it, or those who said they had considered ACP interpreted advance directives sometimes differently from the meaning they have in Belgian law |
Carrion et al27
(2013a)/Florida, USA |
Community health clinics, churches, cultural centers, and support groups |
Qualitative study |
15 Cancer patients |
Only two of the Latino men had completed a living will and two men were knowledgeable about a living will and a health surrogate. Some of the men in the study reported not feeling ready to discuss any ACP, yet others had informally discussed ACP plans with their wives and family members. Those who had limited knowledge and understanding of a cancer diagnosis were particularly worried. |
Carrion et al28
(2013)/ Florida, USA |
Community health clinics, churches, cultural centres, and cancer support groups |
Qualitative study |
45 Cancer patients |
The participants’ responses highlight the misunderstanding of ACP, as they related it to insurance and financial factors. Of the 13 participants who had heard of ACP but had not completed them, none were able to satisfactorily articulate the definition of ACP. |
Voltz et al29
(1998)/
USA, Germany, Japan |
PC and hospice care units |
Quantitative study |
159 Patients |
The answers were classified as positive feelings (for example, relief, happiness) or negative feelings (for example, sadness, loneliness, fear, loss of control, frustration, concern, anger). In the United States and Germany, more than 80% of the patients mentioned negative feelings. In Japan, 17% of patients said they felt no emotions facing their future decision (different from the United States). Only 45% of Japanese patients had negative emotions toward their future decision, this percentage being lower than in the United States or Germany. |
Tsai et al30
(2022)/Taiwan |
Family medicine clinic |
cross-sectional study |
198 Adults who were outpatients of a family medicine clinic |
Most (138/198) respondents indicated that ACP is important to very important, of which 60% (85/138) showed a high willingness to participate in AC. |
Enguidanos & Ailshire31
(2017)/
USA |
Data from the Health and Retirement Study |
Survey Study |
2904 Proxy of deceased cancer patients |
The higher prevalence of preference for aggressive care associated with ADs completed in the last three months of life. As the result of hurried discussions around urgent treatment procedures rather than in-depth goals of care discussion. Early completion of an AD is not associated with a preference for more aggressive. Additionally, even ADs completed 10 years or more before death were associated with lower rates of preferences for aggressive care. |
Feng et al8
(2020)/Sichuan, China |
Oncology outpatient clinic |
Cross-sectional study |
148 LUNG cancer patients and 149 caregivers |
Lung cancer patients, there were significant differences in attitude toward having ADs among patients choosing different time to have ADs and those relying on different people’s advice to make medical choices. For caregivers, there were differences in attitude toward having ADs among groups with different attitudes toward the management of patients, including whether patients should know the diagnosis and prognosis of the disease, willingness to advocate surgery and radiotherapy for patients, and caregivers own willingness to receive radiotherapy and chemotherapy if they were diagnosed with cancer. |
Kish et al32
(2000)/Texas, USA |
Medical ICU |
Prospective quantitative |
872 Critically ill cancer patients, Solid and nonsolid cancer |
African American generally had a positive attitude about AD, although many did not trust formal documents. Completion of AD will compromise their care; they agree living will help them keep control over their terminal care. African American wanted more life sustaining treatment and less likely to complete a living will |
Pautex et al33
(2010)/Geneva, Switzerland |
Hospital |
Retrospective chart review |
50 Patients with an advanced oncological disease |
Motivations of patients to complete their ADs were: to enhance autonomy, to enhance communication with caregivers, fear of over treatment, not to be a burden, to enhance communication with their surrogates and to be sure their preferences will be respected. Wish to have everything attempted to prolong his life, to have everything done to keep or improve their cognitive function even if symptoms like pain would be experienced, wish not to die alone, and nominated proxies they wanted to stay along during the dying process. |
Sahm et al34
(2005)/Hesse, Germany |
The Oncology Clinic and in the Breast Cancer Centre |
Survey cohort study |
100 Cancer patients |
Only a minority of the participants had written an advance directive and knew about the possibility of authorising a health care proxy. Deteriorating health was associated with increasing willingness to make a directive. Despite a majority belief that ADs may influence treatment at the end of life, other factors limit their employment, such as fear of abuse. |
Zhang et al35
(2016)/Guangzhou, China |
Seven organ-specific departments in the Sun Yat-sen University Cancer Center |
Quantitative study |
209 Cancer patients and 215 family caregivers |
Most participants (74%) agreed with ADs. More than 80% answered that “when they were diagnosed with a life-threatening disease” was the optimal time for completing ADs. |
Driller et al36
(2022)/Norway |
Home care |
Retrospective observational cohort study |
250 Cancer patients |
The patients with ACP conversations also more frequently died at home (impact of ACP) |
Hou et al37
(2021)/Beijing, China |
Tumour hospital |
Cross-sectional study |
264 Advanced cancer patients |
The main reasons for refusing to talk about ACP included “trust relatives to make appropriate decisions for them”, “trust doctors to make appropriate decisions for them” and “fear of making their relatives sad”. Most (67.8%) chose to refuse resuscitation attempts or life-sustaining medical interventions. they considered to accept resuscitation attempts or life-sustaining medical interventions were “could comfort their relatives” and “may prolong their own life”, and the main reasons why they refused were “let nature take its course”, “were unwilling to drag their family down”, “hope to die with dignity” and “were unwilling to have low quality of life”. most (70.8%) hoped to have a surrogate decision maker, and their wife or husbands were the most important proxy decision maker. |
Michael et al38
(2014)/Melbourne, Australia |
A large tertiary cancer centre |
A qualitative descriptive design with grounded theory |
>18 Caregivers and 17 patients |
Caregivers can acknowledge patients’ future care wishes while developing subsidiary plans. According to the caregivers, there is often a mismatch between primary and secondary caregivers’ and patients’ desires to discuss various ACP components. Although agreeing with ACP themselves, some believed that patients would not discuss the concept. |
Abu Al Hamayel et al39
(2019)/Maryland, US |
An academic suburban primary care clinic |
Qualitative study |
20 Older patients |
Generally, patients thought it was important to think about their end- of-life wishes and start planning sooner rather than later, when they are not able to make decisions for themselves. This thought process entailed having discussions about wishes and future illness with family members and primary care clinicians in advance of preparing these documents. Patients were aware of the relevance/ importance of ACP as a whole process that includes both discussions with family members and/or primary care clinicians, and completion of ADs or similar forms. Aging and the consequences of aging (e.g., being forgetful) motivated patients to begin exploring their wishes and preferences, and patients’ career field, specifically those in medicine or law, which made them more aware of issues that could surface if preferences were not considered early. |
Andreassen et al40
(2017)/Aarhus C, Denmark |
The departments of cardiology, pulmonology and oncology. |
Qualitative study |
10 Patients with seriously ill from lung disease, heart disease or cancer |
One patient and three relatives described different positive effects the ACP discussion had had on their lives or on the patient’s EOL. Three factors in particular were emphasised as having been affected in a positive way by ACP: communication, awareness of dying and a sense of empowerment. Distrust that the preferences described in the advance directive would be met. Another reason for perceiving ACP as insignificant was the view that no one can foresee or control events in connection with EOL care and death which makes it difficult or even impossible to plan for in advance. Patient–relative conflict reveals how an ACP discussion has the potential to obstruct communication about EOL care and death, if one or more of the involved parties are offended or overwhelmed by the subject matter. |
Johnson et al41
(2017)/
New South Wales, Australia |
Metropolitan hospitals |
Qualitative study |
5 Metastatic cancer patients and 6 family members |
Cancer and death was framed in terms of a threat to self, and to others, with an accompanying loss of control. Participants described trust as a central element of the experience of having cancer, as patients and family are dependent on other people’s expertise and care. Trust extended not only to individuals such as spouses, but doctors and the healthcare system as a whole. |
Barnes et al42
(2012)/London, UK |
Out-patient clinic |
Qualitative study |
22 Palliative care and oncology patients |
The majority of participants felt the most appropriate time to discuss advance care planning would be after a recurrence of disease, or when treatment has failed and the prognosis is poor. Advance care planning discussions may enhance a sense of control by providing the opportunity to make choices regarding the end-of-life. A number of participants said that having cancer had changed the way they viewed life, so that they wanted to live more in the present and not dwell too much on the future. Some said there were things they would appreciate discussing, but they also wanted to be able to close the topic down again. |
Chiang et al43
(2021)/Hualien, Taiwan |
Transnational (Taiwan, Hongkong, Singapore, Australia) |
Qualitative study |
111 Participants were conducted in Taiwan, Singapore, Hong Kong, and Australia |
They were not receptive to life-sustaining treatments that prolonged the near-death process, including intubation, defibrillation, and cardiac massage, as they felt that such treatments not only increase the pain of the patient but also cause distress for their relatives. Participants from Singapore and Australia exhibited significantly more open attitudes. They were willing to engage in end-of-life discussions on any occasion, e.g., during hospitalisation or everyday life at home. |
Lipnick et al44
(2020)/Philadelphia and Massachusetts, US |
Tertiary care centers |
Mixed Method |
285 Adult patients with advanced illness alone or with spokespersons (285), 198 spokespersons for interview |
Spokespersons indicated that their attitudes toward ACP conversations influenced their stress. For example, those who stated that ACP conversations were stressful focused on the inherent difficulty in having the end-of-life conversations, whereas those who did not experience stress focused on the importance of ACP conversations for gathering information about their loved one’s wishes. Many spokespersons focused on their self-described personality, identity, and belief system as impacting whether or not subsequent ACP conversations were stressful. Those who reported ACP conversations as being stressful often said that they were emotional people, and stress often resulted from trying to hide their emotions from their loved ones during conversations. Many spokespersons noted that their stress during ACP conversations was related to their existing interpersonal relationship with their loved one |
Karches et al45
(2012)/
Chicago, USA |
The general internal medicine |
Quantitative study |
8308 Patients |
Religious characteristics, in multivariate analysis, were not significantly associated with having a DNR order, ADs were slightly more common among patients with moderate spirituality than among those with low spirituality |
Kubi et al46
(2020)/Maryland, USA |
The surgical oncology and medical oncology units |
A cross-sectional 19-question survey |
200 Cancer patients |
Four participants reported that their “religion has direct consequences for [their] medical decisions.” This subset of patients felt that ACP was the most powerful way to prevent others from infringing upon their values. |
Zheng et al47
(2016)/Chengdu, China |
Hospital inpatient services |
Quantitative study |
526 Cancer patients |
Patients in the approved ADs group were more willing to discuss about ADs in the place of cancer centre, were more likely to choose comfort care near the EOL compared with those in the disapproved ADs group. Most of respondents would like to pass away at home. Religious beliefs were more likely to have willingness to designate ADs. |
Menon et al48
(2018)/Singapore |
Health care institutions |
An explorative qualitative study |
61 Participants (15 doctors, 13 nurses, 5 MSWs, 15 patients, and 13 caregivers). |
All participants expected that ACP had limited value because the relatives were often the key decision-makers. This was especially so for elderly patients as well as patients and caregivers. |
Abu Al Hamayel et al39
(2019)/Maryland, USA |
An academic suburban primary care clinic |
Qualitative study |
20 Older patients |
Personal values helped shape patients’ preferences. Patients expressed not wanting extreme measures or interventions if they were not getting better, but still wanted to be kept comfortable. Patients highlighted quality of life as a central concept for their preference for refraining from extreme measures. Patients also valued being at home and surrounded with loved ones rather than being in a hospital or a nursing home. |
Shen et al49
(2020)/New York, USA |
Outpatient cancer clinics |
Qualitative study |
20 Patients and 9 caregivers |
Participants’ discussions of the intersection of care with religious faith indicated a powerful belief in the ability of a higher power to restore the patient to health. The consequence of this firm belief or all patients and caregivers who reported that they subscribed to it was that hope was never lost, provided that faith remained strong. |
Carrion et al28
(2013)/
Florida, USA |
Community health clinics, churches, cultural centers, and support groups |
Qualitative study |
15 Cancer patients |
The participants reported that family members were supportive yet were not always aware of the role changes that occurred as a result of their diagnosis. His religious beliefs enabled him to openly discuss with his physician his inability to accept a blood transfusion during brain surgery. |
Epstein et al50
(2015)/New York, USA |
Outpatient medical oncologist |
Qualitative study |
54 Patients with advanced hepato-pancreatic-biliary cancers |
Participants were apprehensive about ACP but wanted to discuss it. Information about the process of cardiopulmonary resuscitation (CPR) affirmed existing personal beliefs/ knowledge/ values: ‘The video reinforced what we felt inside,’ ‘I am guided by my [religious] laws,’ and ‘I don’t want my family to suffer’ were examples of the various ways in which the themes of affirmation emerged. |
Michael et al38
(2014)/Victoria, Australia |
A large tertiary cancer center |
Qualitative study |
18 Caregivers of the lung and gastrointestinal cancer patients |
The caregivers’ lack of experience, caring-related fatigue, belief that others will make ACP decisions, or concern that their views will affect patients’ plans. ACP, many caregivers said, was confronting in cancer care because of cancer’s association with death. Conversations may not occur because imagining the patient’s deterioration is ‘‘scary’’ or ‘‘things are good now so you tend to forget about it.” although agreeing with ACP themselves, some believed that patients would not discuss the concept. ‘‘There is no way on this earth that ACP would have suited my parents because that would be like encouraging (other group participants: ‘fate?’ and ‘bad aura?’) something.” |
Agarwal et al9
(2020)/New York, USA |
GI medical oncology clinics |
Mixed method |
151 Patients with advanced gastrointestinal (GI) cancers |
The participants with increased distress, thematic analysis demonstrated that nearly all preferred limited or comfort care at the end of life had a negative emotional response and expressed fear of life-prolonging measures (CPR and mechanical ventilation) as depicted in the video and identified their familial relationships and religious faith as sources of support. We believe that distress may therefore be a by-product of engaging in a value-based interview while coping with disease-related emotions and processing information from the video about end-of-life care options. |
Zwakman et al12
(2020)/six European countries Belgium, Denmark, Italy, the Netherlands, Slovenia and the United Kingdom |
Hospital |
Mixed method |
125 Patients with advanced cancer |
Religion was described by most patients. Fifteen patients specified their religion (e.g. Church of England, Catholic or Christian). The same number of patients elaborated on the role their religion played in their lives regarding their disease or described preferences based on their religion. Regarding personal beliefs, a few patients described living day-by-day, not giving up and being positive. One patient described: “I believe in faith, that the course of life and experiences are predestined”. |
Tsai et al30
(2022)/Taiwan |
Family medicine clinic |
Cross-sectional study |
198 Adults who were outpatients of a family medicine clinic |
Confucianism has deeply influenced the Chinese culture, and thus, consideration of the family is a significant ethical consideration in medical decision making |
Garrido et al20
(2014)/USA |
Out-patient clinic |
Quantitative study |
606 Patients (437 Non-Latino White, 93 Black, 76 Latino) with advanced cancer |
The relationship between preferences against life-prolonging care and increased likelihood of advance care planning is consistent across racial/ethnic groups. |
Xing et al23
(2017)/China |
The Oncology Department |
Quantitative study |
412 Adult cancer patients |
Chinese family members always protected the patients from hearing their end-of-life message. Modern Chinese people, mainly living in cities, who have received better education from Western culture tended to participate more in the AD discussion. Moreover, patients with a superordinate family position presented an increased tendency to be involved in their AD discussion. When an AD had to be discussed, patients living in villages tended to follow the traditional Chinese culture and preferred to die in their family temples. Thus, they more actively accepted the concept of ADs and spent the last days of their lives at home. |
Chu et al51
(2018)/Taipei, Taiwan |
Hospital inpatient services |
Retrospective study |
1411 CHRONIC life-limiting illness patients |
All Taiwanese adults who have full capacity to make juridical decisions can establish AD regarding the EOL care and family members can become surrogate decision-makers if patients lose their decisional capacity. The findings of this study suggest that ACP and AD are feasible in the East Asia. |
Van Eechoud et al26
(2014) /Flanders, Belgium |
The acute geriatric
ward, the medical oncology ward, and the palliative care unit |
Qualitative methodology, with constructivist grounded theory |
21 Family members |
Family members took different positions in the end-of-life care planning for the older patient with a limited prognosis. Family members in this position did not want to be responsible for decision making but strongly felt the expectation of the patient for them to make decisions. This responsibility caused them to feel burdened, and consequently they experienced considerable tension. All family members in this position were non spouses, namely daughters |
Carrion et al28
(2013)/Florida, USA |
Community health clinics, churches, cultural centers, and cancer support groups |
Qualitative study |
45 Cancer patients |
Female patients plan ahead with the assistance of their spouse and physician; consequently, they successfully documented their advance care plans. Despite the lack of formal information and the limited provision of knowledge from health professionals, the Mexican women acknowledged the precarious nature of their cancer diagnosis and informally discussed after death plans with family members, trusting that their desires would be fulfilled. |
Chiang et al43
(2021)/Hualien, Taiwan |
Transnational (Taiwan, Hongkong, Singapore, Australia) |
Qualitative study |
111 Participants were conducted in Taiwan, Singapore, Hong Kong, and Australia |
Participants from Singapore had divided opinions, with some showing a preference for end-of-life care at home due to the visitor restrictions at hospitals and the inconvenience of travelling back and forth from the hospital for their family members. Other participants preferred to pass away in a hospital or hospice care unit in view of the lack of healthcare professionals and medical equipment at home, the complicated process of filing out a death certificate for a home death, and negative emotions such as fear and a sense of loss that may arise in young children. |
Martina et al52
(2022)/Indonesia |
In patient ward at a national cancer centre in Jakarta and a tertiary academic general hospital in Yogyakarta |
Qualitative study |
16 Patients with cancer and 15 family caregivers |
Four major themes emerged as important in advance care planning: (1) participants' perceptions on the importance or harmfulness of cancer-related information, (2) the importance of communicating bad news sensitively (through empathetic, implicit, and mediated communication),54 participants' motives for participating in medical decision-making (decision-making seen as patients' right or responsibility, or patients' state of dependency on others), and (4) the complexities of future planning (e.g., due to its irrelevance to participants' religious beliefs and/or their difficulties in seeing the relevance of future planning). |
Anaka et al53
(2022)/Canada |
Two tertiary, four regional, and 11 community cancer centers in Alberta province. |
Retrospective study |
471 Patients newly diagnosed with advanced pancreatic cancer |
There is an increased participation of goal of care in the outpatient records of patients with advanced pancreatic cancer during the multifactorial ACP initiative. The goals of care include medical care resuscitation, full resuscitation and comfort care. Multifactorials include participants and translation multilanguage of written materials. |
Huepenbecker et al54
(2022)/USA |
Single institution but clearly explained |
Need assessment |
106 Patients |
33% of patients had ACP documents, 26 % had discussed ACP with a physician, and the majority (82%) thought discussing ACP was important. The majority preferred these conversations in the outpatient setting (52%) with their gynecologic oncologist (80%) instead of nurses or trainees. ACP discussions with an oncologist during outpatient visits are important to patients and improve their knowledge regarding completing ACP documents. |
Table 2.
Synthesis of components of ACP
|
Author (year)
|
Knowledge and perception
|
Attitude and behavior
|
Values and beliefs
|
Cultural aspects and ethnic factors
|
| Karches et al45 (2012) |
|
✓ |
✓ |
✓ |
| Park et al19 (2019) |
✓ |
✓ |
|
|
| Voltz et al29 (1998) |
|
✓ |
|
|
| McMahan et al25 (2013) |
✓ |
|
|
|
| Tsai et al30 (2022) |
✓ |
✓ |
✓ |
|
| Enguidanos & Ailshire31 (2017) |
✓ |
✓ |
|
|
| Berkowitz et al6 (2021) |
✓ |
|
|
✓ |
| Ermers et al5 (2019) |
|
✓ |
✓ |
|
| Feng et al8 (2020) |
✓ |
✓ |
|
|
| Garrido et al20 (2014) |
✓ |
✓ |
|
✓ |
| Hu et al21 (2021) |
|
✓ |
✓ |
✓ |
| Kish et al32 (2000) |
|
✓ |
✓ |
✓ |
| Kubi et al46 (2020) |
✓ |
✓ |
✓ |
✓ |
| McDonald et al22 (2017) |
✓ |
✓ |
✓ |
✓ |
| Pautex et al33 (2010) |
|
✓ |
✓ |
|
| Sahm et al34(2005) |
✓ |
✓ |
✓ |
|
| Xing et al23(2017) |
✓ |
✓ |
✓ |
✓ |
| Zhang et al35 (2016) |
|
✓ |
|
|
| Zheng et al47 (2016) |
|
✓ |
✓ |
|
| Chu et al51 (2018) |
✓ |
✓ |
|
|
| Driller et al36 (2022) |
|
✓ |
|
|
| Falzarano et al24 (2021) |
✓ |
✓ |
✓ |
|
| Hou et al37 (2021) |
✓ |
✓ |
✓ |
|
| Menon et al48 (2018) |
✓ |
✓ |
✓ |
|
| Michael et al38 (2014) |
✓ |
✓ |
✓ |
|
| van Eechoud et al26 (2014) |
✓ |
✓ |
|
|
| Abu Al Hamayel et al39 (2019) |
✓ |
✓ |
✓ |
|
| Shen et al49 (2020) |
|
|
✓ |
✓ |
| Andreassen et al40 (2017) |
|
✓ |
✓ |
✓ |
| Carrion et al27 (2013) |
✓ |
✓ |
✓ |
✓ |
| Carrion et al28 (2013) |
✓ |
✓ |
✓ |
|
| Epstein et al50 (2015) |
✓ |
✓ |
✓ |
|
| Johnson et al41 (2017) |
✓ |
|
✓ |
|
| Michael et al38 (2014) |
✓ |
✓ |
✓ |
✓ |
| Barnes et al42 (2012) |
✓ |
✓ |
✓ |
|
| Chiang et al43 (2021) |
✓ |
✓ |
✓ |
✓ |
| Lipnick et al44 (2020) |
✓ |
✓ |
✓ |
✓ |
| Agarwal et al9 (2020) |
|
✓ |
✓ |
|
| Zwakman et al12 (2020) |
|
|
✓ |
|
| Huepenbecker et al54 (2022) |
✓ |
|
|
|
| Anaka et al53 (2022) |
✓ |
|
|
|
| Martina et al52 (2022) |
|
|
|
✓ |
Patients and Family Caregivers’ Values and Belief on ACP
Twenty-six studies discussed values and beliefs related to ACP. We divided into two components: Spirituality (religious influence) and the power of belief. Three studies discussed the role of spirituality and religious influence on ACP discussion.12,28,45 ADs were found slightly more common among patients with moderate spirituality than among those with low spirituality.45 The power of belief was discussed in many included studies. Three studies from the USA found that faith or belief helped patients remain strong, feel supported, and enabled them to openly discuss treatment options with their physicians, including whether to accept or reject care.9,28,49
Patients and Family Caregivers’ Culture and Ethnic on ACP
Thirteen studies reported that patients’ and family caregivers’ cultural and ethnic backgrounds influenced their perspectives on ACP. For example, a study found that modern Chinese people who live in cities and have received Western education tended to participate more in the AD discussion, while patients living in villages tended to follow the traditional Chinese culture and preferred to die in their family temples.23 One study in Singapore showed that among elderly patients and caregivers ACP had limited value because the relatives were often the key decision-makers.48
Discussion
This study provides a comprehensive review of the research evidence on multiple components of ACP particularly among patients with cancer. To the best of our knowledge, it is the first review to offer a multicomponent perspective on ACP among patients with cancer and their families as caregivers. The study classified these components into key domains: knowledge, attitudes and behavior, values and beliefs, and cultural and ethnic perspectives of patients with cancer.
The evidence shows that lack of awareness and understanding of ACP is one of the main barriers among patients. This is consistent with a review by Crooks et al57 which found that lack of knowledge is a principal barrier to ACP in minorityy ethnic groups. Furthermore, another study found that a lack of ACP knowledge was a key factor influencing outpatients’ unwillingness to engage in ACP.30 These findings are also in line with one study reporting that both lack of knowledge and procrastination were the strongest barriers to completing ADs.22 Similarly, patients who have less knowledge due to lower educational level tended to refuse treatment and against healthcare professionals’ recommendations.23 These patients often did not feel ready to discuss ACP, as their limited understanding of their disease led to increased worry and hesitation.28 Even though more than half of the participants expressed a desire to make decisions about their end-of-life (EOL) care and considered hospice care important. However, only a tenth of them were familiar with ACP and AD.21 When information was cognitively processed and accepted by patients, it was associated with higher completion rates of Do Not Resuscitate (DNR) orders and played a fundamental role in end-of-life decision-making and care.24 Undoubtedly, there are many patients and families had never heard of or considered ACP and AD prior to being admitted to hospital or palliative care unit facilities, resulting in a lack accurate knowledge about ACP.26 Additionally, many patients hold misperceptions about medical interventions and care at the end of life.22
Attitude among patients and families toward completing ACPvaried widely and were affected by their concerns, knowledge, values, and beliefs. There is evidence indicating that the most respondents considered ACP to be important or very important, of which 60% showed a high willingness to participate in ACP.30 Another study reported that patients’ expression regarding ACP predominantly included positive feelings (for example, relief, happiness), while the rest were negative feelings (for example, sadness, loneliness, fear, loss of control, frustration, concern, anger). In the United States and Germany, more than 80% of the patients mentioned negative feelings. In Japan, 17% of patients said they felt no emotions facing their future decision (different from the United States). Only 45% of Japanese patients had negative emotions toward their future decision, this percentage being lower than in the United States or Germany.29
African Americans generally held positive attitudes toward AD, although many did not trust formal documents. Some believed that completing an AD might compromise their care; however, they agreed that having a ‘living will’ would help maintain control over their end-of-life care. African Americans wanted more life sustaining treatment and less likely to complete a living will.32 Additional motivations for completing ADs included: Enhancing autonomy, improving communication with caregivers and surrogates, fear of overtreatment, avoiding burdening others, and ensuring that personal preferences would be respected, a desire to pursue all available measures to prolong life, maintain cognitive function even if accompanied by pain, avoid dying alone, and designate proxies to be present during the dying process.33
Values and beliefs were found to frequently impact the acceptability of ACP. For some participants, the end of life was pre-ordained by God, planning for the end of life was perceived to undermine God’s authority, or to be unnecessary as their end of life had already been planned by a higher being. Consequently, some faith-centred ethnic groups are choosing not to engage with ACP. Although religion was not specifically measured in this study, previous research often considers ethnicity and religion to be closely intertwined.57 Although religion and spirituality were not significantly associated with the presence of a DNR order, ACP and AD were slightly more accepted among patients with moderate levels of spirituality.45 A study reported that religion has direct consequences for patients’ medical decisions. This subset of patients felt that ACP was the most powerful way to prevent others from infringing upon their values.46
Further, personal values helped shape patients’ preferences. Patients expressed not wanting extreme measures or interventions if they were not getting better but still wanted to be kept comfortable. Patients emphasized quality of life as a key reason for avoiding extreme life-prolonging interventions. Patients also valued being at home and surrounded by loved ones rather than being in a hospital or a nursing home.39 Many participants perceived ACP as having limited value, as decisions were often made by relatives rather than the patients themselves. This was especially so for elderly patients as well as patients and caregivers.49,48
The role of a patient’s family was found to vary within and across ethnicities: some individuals preferred to make decisions alone and avoid burden to their family, while others placed importance on collaborative familial decision-making. The position of individuals and their families regarding familial or self-expression of end-of-life preferences may impact the perceived relevance and importance of ACP, in turn impacting engagement with ACP conversations and documentation.
Chinese family members often protected the patients from hearing their end-of-life message. Patients with a multigenerational family position presented an increased tendency to be involved in their AD discussion. When AD discussions occurred, patients in rural areas tended to adhere to traditional Chinese values and preferred to pass away in family temples. Thus, they more actively accepted the concept of ADs and spent the last days of their lives at home.23 Confucianism has deeply influenced the Chinese culture, and thus, consideration of the family is a significant ethical consideration in medical decision making.30 In contrast, in Western culture such as in Belgium, family members took different positions in the end-of-life care planning for the older patient with a limited prognosis. Family members in this position did not want to be responsible for decision-making but strongly felt the expectation of the patient for them to make decisions. This responsibility caused them to feel burdened, and consequently they experienced considerable tension. All family members in this position were non-spousal relatives, predominantly daughters.26
Mexican women acknowledged the precarious nature of their cancer diagnosis and informally discussed after death plans with family members, trusting that their desires would be fulfilled.27 The relationship between preferences against life-prolonging care and increased likelihood of advance care planning is consistent across racial/ethnic groups.20
It is the first scoping review to investigate and map the components of ACP provision for patients with cancer, enabling it to inform ACP policy-making in various countries, particularly those with multicultural and multi-faith populations. No specific findings were identified regarding ACP within particular religious groups. Therefore, it cannot be concluded that ACP is related to religion, although it is related to values and beliefs. Thus, ACP should be viewed from a spiritual perspective.
Table 3.
Category findings
|
No.
|
Component/ Sub-component
|
Resources
|
|
|
Knowledge and perception
|
| 1 |
Lack of knowledge |
Tsai et al (2022),30 McDonald et al (2017),22 van Eechoud et al (2014),26 Carrion et al (2013b),28Berkowitz et al (2021),6 Carrion et al (2013)27 |
| Variety of perception of ACP |
Park et al (2019),19 Hu et al (2021),21 Abu Al Hamayel et al (2019),39 van Eechoud et al (2014),26 Michael et al (2014),38 Agarwal et al (2020)9 |
| Education on ACP and its impact |
Berkowitz et al (2021),6 Garrido et al (2014),20 Falzarano et al (2021),24 Agarwal et al (2020)9 |
|
|
Patient’s attitude and behaviours on ACP
|
| 2 |
Openness and Acceptance of ACP |
Xing et al (2017),23 van Eechoud et al (2014),26Michael et al (2014),38 Barnes et al (2012),42 Chu et al (2018),51Tsai et al (2022),30 Zhang et al (2016),35 Chiang et al (2021),43 Carrion et al (2013a),27 Zheng et al (2016),47 Epstein et al (2015),50 Feng et al (2020)8 |
| Delay of decision |
Ermers et al (2019),5 Enguidanos & Ailshire (2017),31 Chiang et al (2021),43 Feng et al (2020)8 |
| Influencing factors to have ACP |
Kish et al (2000),32 Chiang et al (2021),43 Pautex et al (2010),33 Sahm et al (2005),34 Hou et al (2021),37 McMahan et al (2013)25 |
|
|
Value and belief
|
| 3 |
Spiritually (religious influence) |
Karches et al (2012),45 Carrion et al (2013),27 Zwakman et al (2020)12 |
| The power of belief |
Shen et al (2020),49 Zwakman et al (2020),12 Tsai et al (2022),30 Kish et al (2000),32 Hu et al (2021),21 Kubi et al (2020),46 McDonald et al (2016),22 Pautex et al (2010),33 Sahm et al (2005),34 Xing et al (2017),23 Zheng et al (2016),47 Falzarano et al (2021),24 Hou et al (2021),37 Menon et al (2018),48 Michael et al (2013),38 Abu Al Hamayel et al (2019),39 Andreassen et al (2015),40 Carrion et al (2013),27 Carrion et al (2013),28 Epstein et al (2015),50 Johnson et al (2017),41 Barnes et al (2012),42 Chiang et al (2021),43 Lipnick et al (2020),44 Agarwal et al (2020)9 |
|
|
Culture and ethnic
|
| 4 |
Culture influence |
Menon et al (2018),48 Karches et al (2012),45 Berkowietz (2021),6 Hu et al (2021),21 Kish et al (2000),32 Kubi et al (2020),46 McDonald et al (2017),22 Shen et al (2020),49 Andreassen et al (2017),40 Carrion et al (2013),27 Michael et al (2014),38 Chiang et al (2021)43 |
| Cultural conflict and boundaries |
Garrido et al (2014),20 Xing et al (2017),23 Martina et al (2022)52 |
Conclusion
Studies on ACP involving patients with cancer and their families were systematically searched and reviewed. The multiple components of the ACP were classified into four main domains: knowledge and perception, attitudes and behaviours, values and beliefs, and cultural and ethnic perspectives. Although the ACP has been widely accepted globally, several essential aspects require consideration, including values and beliefs, as well as cultural and ethnic factors.
Recommendation
This review informs us that applying ACP among patients with cancer and their families may require a slight adjustment to ensure it is delivered in a culturally respectful manner. Furthermore, this review also provides insightful findings and serves as a scientific resource for improving ACP guidelines within healthcare facilities. Various aspects are considered to support the implementation of ACP, including effective communication, addressing trust issues, and promoting awareness of patient preferences. Further research can focus on the implementation of ACP in multi-religious or multi-faith background settings.
Competing Interests
The authors declare that they have no conflict of interest.
Data Availability Statement
All data generated or analysed during this study are included in this article. The datasets are available from the corresponding author on reasonable request.
Ethical Approval
Not applicable.
Research Highlights
What is the current knowledge?
-
Advance care planning (ACP) is a structure decision-making process that aims to help patients establish their decisions, incorporating the sharing of values and preferences for medical care between the patients and healthcare professionals.
-
In a palliative care setting, ACP plays a crucial role in addressing patients’ end-of-life wishes, as a part of comprehensive care particularly for those with cancer.
What is new here?
-
This scoping review emphasizes the multifaceted nature of ACP, categorizing its essential elements into four domains: knowledge and perception, attitudes and behaviors, values and beliefs, and cultural and ethnic considerations.
-
Integrating ACP and religious among patients with cancer and their families is needed, in order to fulfill patients’ and families’ spiritual needs
-
This scoping review highlights the importance of effective communication, trust-building, and understanding patient preferences in delivering ACP
References
- Mullick A, Martin J, Sallnow L. An introduction to advance care planning in practice. BMJ 2013; 347:f6064. doi: 10.1136/bmj.f6064 [Crossref] [ Google Scholar]
- Zwakman M, Jabbarian LJ, van Delden J, van der Heide A, Korfage IJ, Pollock K. Advance care planning: a systematic review about experiences of patients with a life-threatening or life-limiting illness. Palliat Med 2018; 32(8):1305-21. doi: 10.1177/0269216318784474 [Crossref] [ Google Scholar]
- Brinkman-Stoppelenburg A, Rietjens JA, van der Heide A. The effects of advance care planning on end-of-life care: a systematic review. Palliat Med 2014; 28(8):1000-25. doi: 10.1177/0269216314526272 [Crossref] [ Google Scholar]
- Fritz L, Dirven L, Reijneveld JC, Koekkoek JA, Stiggelbout AM, Pasman HR. Advance care planning in glioblastoma patients. Cancers (Basel) 2016; 8(11):102. doi: 10.3390/cancers8110102 [Crossref] [ Google Scholar]
- Ermers DJ, van Bussel KJH, Perry M, Engels Y, Schers HJ. Advance care planning for patients with cancer in the palliative phase in Dutch general practices. Fam Pract 2019; 36(5):587-93. doi: 10.1093/fampra/cmy124 [Crossref] [ Google Scholar]
- Berkowitz CM, Wolf SP, Troy J, Kamal AH. Characteristics of advance care planning in patients with cancer referred to palliative care. JCO Oncol Pract 2021; 17(2):e94-100. doi: 10.1200/op.20.00657 [Crossref] [ Google Scholar]
- Serey K, Cambriel A, Pollina-Bachellerie A, Lotz JP, Philippart F. Advance directives in oncology and haematology: a long way to go-a narrative review. J Clin Med 2022; 11(5):1195. doi: 10.3390/jcm11051195 [Crossref] [ Google Scholar]
- Feng C, Wu J, Li J, Deng HY, Liu J, Zhao S. Advance directives of lung cancer patients and caregivers in China: a cross sectional survey. Thorac Cancer 2020; 11(2):253-63. doi: 10.1111/1759-7714.13237 [Crossref] [ Google Scholar]
- Agarwal R, Shuk E, Romano D, Genoff M, Li Y, O’Reilly EM. A mixed methods analysis of patients’ advance care planning values in outpatient oncology: Person-Centered Oncologic Care and Choices (P-COCC). Support Care Cancer 2020; 28(3):1109-19. doi: 10.1007/s00520-019-04910-1 [Crossref] [ Google Scholar]
- Tsuruwaka M, Ikeguchi Y, Nakamura M. When do physicians and nurses start communication about advance care planning? A qualitative study at an acute care hospital in Japan. Asian Bioeth Rev 2020; 12(3):289-305. doi: 10.1007/s41649-020-00135-1 [Crossref] [ Google Scholar]
- Chow J, Harley A, Chroinin DN, Kohler F, Harlum J, Jobburn K. Understanding of advance care planning in primary care: a gap analysis. Aust J Prim Health 2022; 28(4):344-9. doi: 10.1071/py21253 [Crossref] [ Google Scholar]
- Zwakman M, van Delden JJ, Caswell G, Deliens L, Ingravallo F, Jabbarian LJ. Content analysis of advance directives completed by patients with advanced cancer as part of an advance care planning intervention: insights gained from the ACTION trial. Support Care Cancer 2020; 28(3):1513-22. doi: 10.1007/s00520-019-04956-1 [Crossref] [ Google Scholar]
- Lasmarías C, Aradilla-Herrero A, Silva Fontana Rosa N, Trelis J. Perceptions and experiences of onco-haematology professionals in relation to advance care planning: a qualitative study. Support Care Cancer 2024; 32(3):180. doi: 10.1007/s00520-024-08371-z [Crossref] [ Google Scholar]
- Cheng SY, Lin CP, Chan HY, Martina D, Mori M, Kim SH. Advance care planning in Asian culture. Jpn J Clin Oncol 2020; 50(9):976-89. doi: 10.1093/jjco/hyaa131 [Crossref] [ Google Scholar]
- Sudore RL, Knight SJ, McMahan RD, Feuz M, Farrell D, Miao Y. A novel website to prepare diverse older adults for decision making and advance care planning: a pilot study. J Pain Symptom Manage 2014; 47(4):674-86. doi: 10.1016/j.jpainsymman.2013.05.023 [Crossref] [ Google Scholar]
- Kuusisto A, Saranto K, Korhonen P, Haavisto E. Accessibility of information on patients’ and family members’ end-of-life wishes in advance care planning. Nurs Open 2022; 9(1):428-36. doi: 10.1002/nop2.1081 [Crossref] [ Google Scholar]
- Jimenez G, Tan WS, Virk AK, Low CK, Car J, Ho AH. Overview of systematic reviews of advance care planning: summary of evidence and global lessons. J Pain Symptom Manage 2018; 56(3): 436-59.e25. 10.1016/j.jpainsymman.2018.05.016
- Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med 2018; 169(7):467-73. doi: 10.7326/m18-0850 [Crossref] [ Google Scholar]
- Park HY, Kim YA, Sim JA, Lee J, Ryu H, Lee JL. Attitudes of the general public, cancer patients, family caregivers, and physicians toward advance care planning: a nationwide survey before the enforcement of the life-sustaining treatment decision-making act. J Pain Symptom Manage 2019; 57(4):774-82. doi: 10.1016/j.jpainsymman.2018.12.332 [Crossref] [ Google Scholar]
- Garrido MM, Harrington ST, Prigerson HG. End-of-life treatment preferences: a key to reducing ethnic/racial disparities in advance care planning? Cancer 2014; 120(24): 3981-6. a key to reducing ethnic/racial disparities in advance care planning? Cancer 2014; 120(24):a key to reducing ethnic/racial disparities in advance care planning? Cancer 2014; 120(24). doi: 10.1002/cncr.28970 [Crossref] [ Google Scholar]
- Hu L, Chu Q, Fan Z, Chen Y. Discussion of advance care planning on end-of-life decisions with lung cancer patients in Wuhan, China: attitude, timing and future directions. Intern Med J 2021; 51(12):2111-8. doi: 10.1111/imj.14958 [Crossref] [ Google Scholar]
- McDonald JC, du Manoir JM, Kevork N, Le LW, Zimmermann C. Advance directives in patients with advanced cancer receiving active treatment: attitudes, prevalence, and barriers. Support Care Cancer 2017; 25(2):523-31. doi: 10.1007/s00520-016-3433-6 [Crossref] [ Google Scholar]
- Xing YF, Lin JX, Li X, Lin Q, Ma XK, Chen J. Advance directives: cancer patients’ preferences and family-based decision making. Oncotarget 2017; 8(28):45391-8. doi: 10.18632/oncotarget.17525 [Crossref] [ Google Scholar]
- Falzarano F, Prigerson HG, Maciejewski PK. The role of advance care planning in cancer patient and caregiver grief resolution: helpful or harmful? Cancers (Basel) 2021; 13(8): 1977. helpful or harmful? Cancers (Basel) 2021; 13(8):helpful or harmful? Cancers (Basel) 2021; 13(8). doi: 10.3390/cancers13081977 [Crossref] [ Google Scholar]
- McMahan RD, Knight SJ, Fried TR, Sudore RL. Advance care planning beyond advance directives: perspectives from patients and surrogates. J Pain Symptom Manage 2013; 46(3):355-65. doi: 10.1016/j.jpainsymman.2012.09.006 [Crossref] [ Google Scholar]
- van Eechoud IJ, Piers RD, Van Camp S, Grypdonck M, Van Den Noortgate NJ, Deveugele M. Perspectives of family members on planning end-of-life care for terminally ill and frail older people. J Pain Symptom Manage 2014; 47(5):876-86. doi: 10.1016/j.jpainsymman.2013.06.007 [Crossref] [ Google Scholar]
- Carrion IV, Nedjat-Haiem FR, Marquez DX. Examining cultural factors that influence treatment decisions: a pilot study of Latino men with cancer. J Cancer Educ 2013; 28(4):729-37. doi: 10.1007/s13187-013-0522-9 [Crossref] [ Google Scholar]
- Carrion IV, Nedjat-Haiem FR, Martinez-Tyson D, Castañeda H. Advance care planning among Colombian, Mexican, and Puerto Rican women with a cancer diagnosis. Support Care Cancer 2013; 21(5):1233-9. doi: 10.1007/s00520-012-1652-z [Crossref] [ Google Scholar]
- Voltz R, Akabayashi A, Reese C, Ohi G, Sass HM. End-of-life decisions and advance directives in palliative care: a cross-cultural survey of patients and health-care professionals. J Pain Symptom Manage 1998; 16(3):153-62. doi: 10.1016/s0885-3924(98)00067-0 [Crossref] [ Google Scholar]
- Tsai WT, Chen CM, Chung MC, Tsai PY, Liu YT, Tang FC. Important factors influencing willingness to participate in advance care planning among outpatients: a pilot study in central Taiwan. Int J Environ Res Public Health 2022; 19(9):5266. doi: 10.3390/ijerph19095266 [Crossref] [ Google Scholar]
- Enguidanos S, Ailshire J. Timing of advance directive completion and relationship to care preferences. J Pain Symptom Manage 2017; 53(1):49-56. doi: 10.1016/j.jpainsymman.2016.08.008 [Crossref] [ Google Scholar]
- Kish SK, Martin CG, Price KJ. Advance directives in critically ill cancer patients. Crit Care Nurs Clin North Am 2000; 12(3):373-83. [ Google Scholar]
- Pautex S, Notaridis G, Déramé L, Zulian GB. Preferences of elderly cancer patients in their advance directives. Crit Rev Oncol Hematol 2010; 74(1):61-5. doi: 10.1016/j.critrevonc.2009.04.007 [Crossref] [ Google Scholar]
- Sahm S, Will R, Hommel G. Attitudes towards and barriers to writing advance directives amongst cancer patients, healthy controls, and medical staff. J Med Ethics 2005; 31(8):437-40. doi: 10.1136/jme.2004.009605 [Crossref] [ Google Scholar]
- Zhang Q, Xie C, Xie S, Liu Q. the attitudes of Chinese cancer patients and family caregivers toward advance directives. Int J Environ Res Public Health 2016; 13(8):816. doi: 10.3390/ijerph13080816 [Crossref] [ Google Scholar]
- Driller B, Talseth-Palmer B, Hole T, Strømskag KE, Brenne AT. Cancer patients spend more time at home and more often die at home with advance care planning conversations in primary health care: a retrospective observational cohort study. BMC Palliat Care 2022; 21(1):61. doi: 10.1186/s12904-022-00952-1 [Crossref] [ Google Scholar]
- Hou XT, Lu YH, Yang H, Guo RX, Wang Y, Wen LH. The knowledge and attitude towards advance care planning among Chinese patients with advanced cancer. J Cancer Educ 2021; 36(3):603-10. doi: 10.1007/s13187-019-01670-8 [Crossref] [ Google Scholar]
- Michael N, O’Callaghan C, Baird A, Hiscock N, Clayton J. Cancer caregivers advocate a patient- and family-centered approach to advance care planning. J Pain Symptom Manage 2014; 47(6):1064-77. doi: 10.1016/j.jpainsymman.2013.07.009 [Crossref] [ Google Scholar]
- Abu Al Hamayel N, Isenberg SR, Sixon J, Smith KC, Pitts SI, Dy SM, et al. Preparing older patients with serious illness for advance care planning discussions in primary care. J Pain Symptom Manage 2019; 58(2): 244-51.e1. 10.1016/j.jpainsymman.2019.04.032
- Andreassen P, Neergaard MA, Brogaard T, Skorstengaard MH, Jensen AB. The diverse impact of advance care planning: a long-term follow-up study on patients’ and relatives’ experiences. BMJ Support Palliat Care 2017; 7(3):335-40. doi: 10.1136/bmjspcare-2015-000886 [Crossref] [ Google Scholar]
- Johnson SB, Butow PN, Kerridge I, Tattersall MH. What do patients with cancer and their families value most at the end of life? A critical analysis of advance care planning. Int J Palliat Nurs 2017; 23(12):596-604. doi: 10.12968/ijpn.2017.23.12.596 [Crossref] [ Google Scholar]
- Barnes S, Gardiner C, Gott M, Payne S, Chady B, Small N. Enhancing patient-professional communication about end-of-life issues in life-limiting conditions: a critical review of the literature. J Pain Symptom Manage 2012; 44(6):866-79. doi: 10.1016/j.jpainsymman.2011.11.009 [Crossref] [ Google Scholar]
- Chiang FM, Wang YW, Hsieh JG. How acculturation influences attitudes about advance care planning and end-of-life care among Chinese living in Taiwan, Hong Kong, Singapore, and Australia. Healthcare (Basel) 2021; 9(11):1477. doi: 10.3390/healthcare9111477 [Crossref] [ Google Scholar]
- Lipnick D, Green M, Thiede E, Smith TJ, Lehman EB, Johnson R. Surrogate decision maker stress in advance care planning conversations: a mixed-methods analysis from a randomized controlled trial. J Pain Symptom Manage 2020; 60(6):1117-26. doi: 10.1016/j.jpainsymman.2020.07.001 [Crossref] [ Google Scholar]
- Karches KE, Chung GS, Arora V, Meltzer DO, Curlin FA. Religiosity, spirituality, and end-of-life planning: a single-site survey of medical inpatients. J Pain Symptom Manage 2012; 44(6):843-51. doi: 10.1016/j.jpainsymman.2011.12.277 [Crossref] [ Google Scholar]
- Kubi B, Istl AC, Lee KT, Conca-Cheng A, Johnston FM. Advance care planning in cancer: patient preferences for personnel and timing. JCO Oncol Pract 2020; 16(9):e875-83. doi: 10.1200/jop.19.00367 [Crossref] [ Google Scholar]
- Zheng RJ, Fu Y, Xiang QF, Yang M, Chen L, Shi YK. Knowledge, attitudes, and influencing factors of cancer patients toward approving advance directives in China. Support Care Cancer 2016; 24(10):4097-103. doi: 10.1007/s00520-016-3223-1 [Crossref] [ Google Scholar]
- Menon S, Kars MC, Malhotra C, Campbell AV, van Delden JJM. Advance care planning in a multicultural family centric community: a qualitative study of health care professionals’, patients’, and caregivers’ perspectives. J Pain Symptom Manage 2018; 56(2): 213-21.e4. 10.1016/j.jpainsymman.2018.05.007
- Shen MJ, Manna R, Banerjee SC, Nelson CJ, Alexander K, Alici Y. Incorporating shared decision making into communication with older adults with cancer and their caregivers: development and evaluation of a geriatric shared decision-making communication skills training module. Patient Educ Couns 2020; 103(11):2328-34. doi: 10.1016/j.pec.2020.04.032 [Crossref] [ Google Scholar]
- Epstein AS, Shuk E, O’Reilly EM, Gary KA, Volandes AE. ‘We have to discuss it’: cancer patients’ advance care planning impressions following educational information about cardiopulmonary resuscitation. Psychooncology 2015; 24(12):1767-73. doi: 10.1002/pon.3786 [Crossref] [ Google Scholar]
- Chu D, Yen YF, Hu HY, Lai YJ, Sun WJ, Ko MC. Factors associated with advance directives completion among patients with advance care planning communication in Taipei, Taiwan. PLoS One 2018; 13(7):e0197552. doi: 10.1371/journal.pone.0197552 [Crossref] [ Google Scholar]
- Martina D, Kustanti CY, Dewantari R, Sutandyo N, Putranto R, Shatri H. Advance care planning for patients with cancer and family caregivers in Indonesia: a qualitative study. BMC Palliat Care 2022; 21(1):204. doi: 10.1186/s12904-022-01086-0 [Crossref] [ Google Scholar]
- Anaka M, Lee M, Lim E, Ghosh S, Cheung WY, Spratlin J. Changing rates of goals of care designations in patients with advanced pancreatic cancer during a multifactorial advanced care planning initiative: a real-world evidence study. JCO Oncol Pract 2022; 18(6):e869-76. doi: 10.1200/op.21.00649 [Crossref] [ Google Scholar]
- Huepenbecker SP, Lewis S, Valentine MC, Palisoul ML, Thaker PH, Hagemann AR. Gynecologic oncology patient perspectives and knowledge on advance care planning: a quality improvement intervention. Gynecol Oncol Rep 2022; 43:101060. doi: 10.1016/j.gore.2022.101060 [Crossref] [ Google Scholar]
- Misbah M, Saadat Al Husaini SM, Mujtaba S. An analysis of concept of suffering from a philosophical perspective. Journal of Hikmat-e-Islami 2015; 2(1): 9-31. [Persian].
- Zhang Y, Cui C, Wang Y, Wang L. Effects of stigma, hope and social support on quality of life among Chinese patients diagnosed with oral cancer: a cross-sectional study. Health Qual Life Outcomes 2020; 18(1):112. doi: 10.1186/s12955-020-01353-9 [Crossref] [ Google Scholar]
- Crooks J, Trotter S, Clarke G. How does ethnicity affect presence of advance care planning in care records for individuals with advanced disease? A mixed-methods systematic review. BMC Palliat Care 2023; 22(1):43. doi: 10.1186/s12904-023-01168-7 [Crossref] [ Google Scholar]