Journal of caring sciences. 14(4):217-225.
doi: 10.34172/jcs.025.33829
Original Article
Predictors of Family Caregivers Burden across Palliative Settings in the South of Thailand
Yuwadee Wittayapun Conceptualization, Data curation, Formal analysis, Methodology, Project administration, Resources, Supervision, Visualization, Writing – original draft, Writing – review &editing, 1 
Ueamporn Summart Conceptualization, Data curation, Formal analysis, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing, 2, *
Orathai Pongkaew Data curation, Investigation, Validation, Writing – original draft, Writing – review & editing, 2
Suchittra Saengkhum Data curation, Investigation, Resources, Validation, Writing – review & editing, 3
Yasuko Inaba Investigation, Methodology, Supervision, Writing – review & editing, 4
Author information:
1School of Allied Health Sciences, Walailak University, Nakhon Si Thammarat, Thailand
2Faculty of Nursing, Roi-Et Rajabhat University, Roi-Et, Thailand
3Chaiya Hospital, Surat Thani, Thailand
4School of Nursing and Rehabilitation Sciences, Showa Medical University, Yokohama-shi 226-8555, Kanagawa, Japan
Abstract
Introduction:
Caring for palliative care (PC) patients can impose a high level of burden on family caregivers (FCs). However, little is known about predictors of burden among this population. This study aims to determine the prevalence and factors predicting a high level of FCs burden in those who care for PC patients.
Methods:
This cross-sectional study recruited FCs of individuals with advanced or terminal illness from the PC settings of two health service networks in the south of Thailand. The data were collected using self-administered questionnaires. The prevalence of burden was estimated. Binary logistic regression was employed to identify factors predicting FC burden, and the area under the ROC curve was used to assess model discrimination.
Results:
Of 305 FCs met the eligibility criteria, and 42.3% (95% CI: 36.4-47.7) of them reported experiencing a high level of burden. Factors significantly predicting high burden were severe anxiety (OR=2.19; 95% CI: 1.19-4.01), severe depression (OR=2.17; 95% CI 1.10-4.27), FCs with illness (OR=2.13; 95% CI: 1.23-3.70), decreased quality of life (QOL) by 1 point (OR=1.04; 95% CI: 1.02-1.06), respectively. Likewise, the final model was statistically significant (area under ROC curve=0.79; 95% CI: 0.63-0.74, P<0.001), indicating that this model could differentiate between FCs who reported a high burden and those who did not.
Conclusion:
The burden is high among FCs of palliative care patients. Mental illness affected both functional capacity and QOL and raised FC burden. Preventing and treating such disorders are crucial. Therefore, further studies should investigate strategies for alleviating FC burden in this population.
Keywords: Caregivers burden, Caregivers, Palliative care, Predictors
Copyright and License Information
© 2025 The Author(s).
This work is published by Journal of Caring Sciences as an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/). Non-commercial uses of the work are permitted, provided the original work is properly cited.
Funding Statement
The study has no funding.
Introduction
The rapid increase in the aging population and the effects of epidemiologic transition have resulted in a rise in life-limiting diseases worldwide, thus requiring the enhancement of palliative care (PC).1,2PC is a an approach to care that enhances the quality of life (QOL) for patients and their families confronting life-threatening illnesses by preventing and alleviating suffering through the early identification, accurate assessment, and treatment of pain and other issues, encompassing physical, psychosocial, or spiritual dimensions.3In 2022, Thailand officially transitioned into a fully aged society, which will elevate the number of dependent individuals and the demand for caregivers within households.4 Moreover, the chronic condition of many illnesses means care has transitioned from medical centers to community settings, resulting in an extraordinary need for family caregivers (FCs) assistance. This situation has impacted numerous FCs of individuals with advanced or terminal illnesses, leading to a significant burden.5Due to shifting demographics, informal home-based caregiving is expected to become more demanding, thereby intensifying the problem of FCs burden.6
FCs, primarily relatives or friends, must frequently navigate complex healthcare systems and carry out medical or nursing duties.7 They serve as crucial reference individuals for patients, significantly influencing their wellbeing and QOL; concurrently, they experience the effects of the patients’ illnesses and their own burdens and needs. Research indicates that FCs face varying mental, social, physical, and economic burdens. They also perform medical or nursing duties.8The burden of FCs encompasses both objective aspects, such as caregiving tasks and the time dedicated to caregiving, and subjective aspects, including the caregivers’ experiences and emotions regarding their role.9 Therefore, the issue of FCs in Thailand requires attention. Research indicates that 40–70% of FCs report experiencing a burden.10
Risk factors influencing caregiving burden include female gender, lower educational attainment, cohabitation with the care recipient, extended caregiving hours, anxiety, depression, social isolation, financial strain, caregiver physical health, and lack of choice in caregiving responsibilities.7,8,11-13 In addition, FC burden is associated with poorer self-rated health and reduced QOL.6,14
According to the literature, there are both positive and negative factors associated with the burden of FCs. Previous research that investigated the emotional burden of FCs and related factors was not always consistent. This is because the studies used different measures, and looked at FCs with different illnesses, at different times, and in different care settings.8Because study of PC requires dealing with both QOL and the burden on FCs at the same time, there are few studies that have examined the link between QOL and caregiver burden in PC settings.15 Many studies in Thailand have investigated FC burden in different populations, such as senior citizens with and without physical disabilities,13,16,17 cancer patients,18 and dementia patients.19 The prevalence of burden among these populations varied across studies. For instance, while more than half of FCs of older individuals with physical disabilities reported no or low-moderate burden,17 another study revealed a high level of burden among FCs of older individuals.16 Factors associated with their burdens included being older, being female, caring for more than 8 hours per day, and having physiological or psychological health problems.16,17
Despite the growing interest in PC research, there have been very few analytical studies on the factors predicting burden among FCs in the Thai population.16,17Currently, there is a lack of evidence identifying the predictive factors of care burden among FCs of PC setting. Moreover, current evidence suggests that culture influences caregiving experiences and outcomes, with Asian caregivers reporting different levels of burden compared to their Western counterparts.6 Therefore, this study aims to determine the prevalence and factors predicting a high level of FCs burden in those who care for PC patients.
Materials and Methods
This is a cross-sectional study utilizing data from the research project entitled “Palliative Care Outcomes and Factors Associated with Quality of Life of Caregivers of Palliative Care Patients,” conducted across two district health service networks, comprising two district hospitals and 24 sub-district health promoting hospitals. Data collection took place from December 26, 2023, to March 5, 2024, from all eligible primary FCs who provided informed consent to participate in the study.
Primary FCs who met the specified criteria were invited to participate in the study, including those providing care for patients with advanced or terminal illnesses such as cancer or cerebrovascular disease. The inclusion criteria for this study were being the primary FCs who included friends, family members, and individuals involved in PC, through patients receiving treatment in medical institutions or at home through two district health service networks. They were Thai nationals, aged 18 or older, who had provided care for a minimum of 3 days a week for at least 3 months without compensation. The exclusion criteria were FCs with mental disorders such as schizophrenia, psychosis, or dementia. Thai FCs of patients receiving PC from two primary PC settings of two district health services in the south of Thailand were included in the study population. The sample size was calculated according to the primary research question of this study, which attempted to assess prevalence of high FC burden using an infinite population proportion formula.20Intense burden was observed in 41.6% of the population (P = 0.42),12 e = 0.05, and Zα/2 = 1.96. A minimum sample size of 192 was necessary. Based on the basic guideline for determining sample size in logistic regression, the number of cases should exceed 50 plus eight times the number of independent variables (m), where “m” denotes the number of IVs included in the analysis.21 In total, 15 IVs were used in this investigation. As a result, the 305 cases who met the inclusion criteria exceeded the 170-case threshold.
The data was collected using self-administered questionnaires. This questionnaire comprised two sections: 1) Socio-demographic variables including age, gender, education level, religion, occupation, household income and 2) Psycho-social variables, which are described as follows.
The Thai version of the 12-item Zarit Burden Interview (ZBI-12) has 12 items assessed on a 5-point Likert scale, ranging from 0 (never) to 4 (very often), yielding a total score range of 0 to 48. A higher total score indicates a greater burden, with a score of 20 or more considered a significant burden.22The Cronbach’s alpha coefficient for the Thai version of the ZBI was 0.88.23
The Thai version of DASS-21 is a combination of three self-reported scales used to evaluate depression, anxiety, and stress. It has 21 items separated into three subscales (items 3, 5, 10, 13, 16, 17, and 21 for the ‘depression’ sub-scale, items 2, 4, 9, 15, 19, and 20 for the ‘anxiety’ sub-scale, and items 1, 6, 8, 11, 12, 14, and 18 for the stress sub-scale). This scale can be scored on a 4-point basis. The scale produces scores for each of the three subscales, with higher scores indicating greater symptom intensity. According to the DASS manual, subscale scores are categorized as normal, mild, moderate, severe, or extremely severe. Moreover, a recent study in Thailand has validated this tool and reported a good psychometric property.24
The Thai version of the World Health Organization Quality of Life Brief (WHOQOL-BREF-THAI) is a questionnaire with 26 items, including two items about QOL and general health and 24 items about levels of satisfaction across a range of aspects, including physical health (seven items), psychological health (six items), social relationships (three items), and environmental (eight items). Each item is rated on a 5-point Likert scale (1 to 5). The mean score of items within each domain is used to calculate the domain score, which is then transformed into 4-10 and 0-100 scores in accordance with the questionnaire guidelines. Higher scores indicate a higher QOL.25The WHOQOL-BREF’s reliability has been officially acknowledged by the WHO, with a Cronbach’s alpha value of 0.84 and a content validity score of 0.65.
The Palliative Outcome Scale (POS) is an 11-item assessment tool used to measure perceptions of FCs. Ten items are employed to evaluate bodily symptoms, psychological symptoms, social issues, and spirituality. The 11thitem is an open-ended inquiry regarding other issues. The Cronbach’s alpha coefficient for the Thai version of the POS was found to be 0.90.26
The Family, Adaption, Partnership, Growth, Affection and Resolve (APGAR) Scale, is a scale used by participants to evaluate their level of disagreement or agreement with each statement on a 5-point Likert scale, ranging from 1 (never) to 5 (always). The individual scores are aggregated to calculate the total score. A high score signifies that the individual has received advantageous familial assistance. The Cronbach’s alpha coefficient for this tool was found to be 0.82.27
To describe the demographic characteristics of the participants and the psychological manifestations exhibited among FCs of PC patients, descriptive statistics, means (SD) for continuous variables, and counts and percentages for categorical data were utilized. Logistic regression models were developed in the following manner: 1) Potential influencing factors of a high level of FC burden were identified. 2) All significant variables, including those deemed significant in the included demographic characteristics, and psychosocial factors were selected by using univariate analysis. 3) All significant variables, including those deemed significant based on previous studies,7,8,11-13,17 were included in the bivariate analysis. 4) To assess the multivariate model fit, we employed backward elimination and the Wald statistic to determine each factor’s contribution to the model. 5) The likelihood ratio test was used for comparing the new model versus the previous model. 6) We tested the final model for linearity and interactions after it was completed. Finally, the adjusted odds ratio (AOR) with a 95% confidence interval (95% CI) was used for measuring the association in the final model. STATA 14.0 (Stata Corp, 2015, College Station, Texas) was used for statistical analysis, and a two-tailed test was performed at a significance of 0.05. Moreover, the area under the ROC curve (C-statistic with a 95% CI) was utilized to assess model discrimination. Backward elimination and the Hosmer-Lemeshow goodness-of-fit statistic were applied for validating the model calibration, with a p-value of more than 0.05 suggesting adequate calibration.28
The research adhered to the ethical standards and principles established in the Declaration of Helsinki. The study protocol received ethical clearance from the Walailak University Institutional Review Board (Reference No. WUEC-23-344-01). All study participants provided informed written consent for this investigation. Additionally, each participant was guaranteed the confidentiality of their personal information.
Results
Of the 305 participants, (79.4%) were female, and the mean (SD) age was 54.18 (13.52) years. The majority of the participants (71.4%) had a secondary level of education and were married (68.2%). Approximately 48.8% of the participants were the children of the patients. The most common diagnosis among the PC patients was cerebrovascular disease (32.8%). Table 1 summarizes the details of the participant characteristics.
Most of the FCs reported receiving a high level of social support (83.5%) and receiving mild PC outcomes (67.2%). The results of this study indicated the prevalence of psychosocial manifestations among FCs. The most common psychological manifestation among these FCs includes depression, with 230 (75.4%) reporting moderate intensity, severe anxiety (57.4%), and mild stress symptoms (41.3%), respectively. In addition, more than half of the FCs (60%) reported a moderate QOL (Table 2).
The mean (SD) ZBI-12 score among the FCs was 20.42 (7.68), suggesting moderate to high burden. Interestingly, we found that all individuals in the study reported experiencing some degree of FC burden. The majority, numbering 176 individuals, experienced a moderate level of burden (57.7%; 95% CI: 51.3-62.7), while 129 individuals were affected by a high level of burden (42.3%; 95% CI: 36.4-47.7) (Table 3).
Based on the univariate analysis of factors significantly predicted a high level of burden among palliative FCs. The results showed that seven out of 15 potential factors associated with this outcome were FCs with illness, social support, depression, anxiety, stress, PC outcome, and decreased QOL, respectively (Table 4).
We conducted multiple logistic regression on variables that were significant after univariate analysis to determine their independent association with a high level of burden among palliative FCs, while adjusting for confounding effects from other factors. FCs with illness, depression, anxiety, and decreased QOL were the four independent variables in the logistic model. The strongest predictor of the four variables was found to be anxiety. FCs who reported severe anxiety were 2.19 times more likely to develop a high level of burden than those reporting moderate anxiety, with an AOR of 2.19 (95% CI: 1.19-4.01). Depression came in second place, with an AOR of 2.17 (95% CI: 1.10-4.27), indicating that FCs with symptoms of severe depression were 2.17 times more likely to experience a high level of burden. FCs with illness came in third place, with an AOR of 2.13 (95% CI: 1.23-3.70), indicating that they were 2.13 times more likely to experience a high level of burden. The final predictor was decreased QOL, with an AOR of 1.04 (95% CI: 1.02-1.06), indicating that the FCs whose QOL had decreased by 1 point were 1.04 times more likely to experience a high level of burden. Moreover, the final model, including four predictors, was statistically significant (p-value < 0.001), indicating the disparity between FCs who reported a high level of burden and those who did not as shown in Table 5.
The final model was significant (area under the ROC curve = 0.79, 95% CI: 0.63-0.74, P < 0.001). The area under the ROC curve close to 1 indicates that this model could differentiate between FCs who reported high levels of burden and those who did not (Figure 1).
Table 1.
Demographic characteristics of family caregivers (N = 305)
|
Baseline characteristics
|
N (%)
|
| Gender |
|
| Male |
63 (20.6) |
| Female |
242 (79.4) |
| Age group |
|
| Below 60 years of age |
197 (64.6) |
| 60 years of age or older |
108 (35.4) |
| Mean (SD) |
54.18 (13.52) |
| Median (min: max) |
54 (30:86) |
| Education level |
|
| Primary |
3 (1.0) |
| Secondary |
218 (71.4) |
| Bachelor’s or higher |
84 (27.6) |
| Religion |
|
| Buddhism |
255 (83.6) |
| Islam |
50 (16.4) |
| Occupation |
|
| Full-time employed |
193 (63.3) |
| Part-time employed |
47 (15.4) |
| Unemployed |
65 (21.3) |
| Household income (Thai baht) |
|
| Not specified |
10 (3.3) |
| Less than 5000 |
89 (29.2) |
| 5,000-9,999 |
74 (24.3) |
| 10,000-14,999 |
47 (15.4) |
| 15,000-19,999 |
25 (8.2) |
| ≥ 20,000 |
60 (19.7) |
| Mean (SD) |
12600.58 (19725.27) |
| Median (min: max) |
9000 (0-30,000) |
| Marital status |
|
| Single |
51 (16.7) |
| Married |
208 (68.2) |
| Divorced/ separated |
46 (15.1) |
| Caregiver with illness |
|
| No |
192 (62.9) |
| Yes |
113)37.1) |
| Relationship status of caregiver |
|
| Parent |
34 (11.2) |
| Spouse |
50 (16.4) |
| Children |
149 (48.8) |
| Other relative |
72 (23.6) |
| Family members |
|
| Fewer than 5 |
199 (65.3) |
| ≥ 5 |
106 (34.7) |
| Duration of care (h) |
|
| Less than 8 |
108 (35.4) |
| ≥ 8 |
197 (64.6) |
| Mean (SD) |
17.72 (7.66) |
| Median (min: max) |
24 (1: 24) |
| Duration of caregiving (y) |
|
| Less than 5 |
227 (74.4) |
| ≥ 5 |
78 (25.6) |
| Diagnosis of the relative |
|
| Cancer |
36 (11.8) |
| Cerebrovascular disease |
100 (32.8) |
| Cardiovascular disease |
17 (5.6) |
| Others (pediatric disease, multiple injuries) |
152 (49.8) |
Table 2.
Psychosocial factors effecting the burden in family caregivers of palliative care patients
|
Factors
|
N (%)
|
| Social support (Family APGAR scale) |
|
| Low |
6 (2.0) |
| Moderate |
44 (14.5) |
| High |
255 (83.5) |
| Mean (SD) |
19.91 (5.67) |
| Palliative care outcome (according to the POS) |
|
| Mild |
205 (67.2) |
| Moderate |
84 (27.5) |
| High/severe |
16 (5.3) |
| Mean (SD) |
7.89 (6.64) |
| Stress symptoms (DASS-S) |
|
| Mild |
126 (41.3) |
| Moderate |
78 (25.6) |
| Severe |
101 (33.1) |
| Mean (SD) |
11.65 (4.11) |
| Anxiety symptoms (DASS-A) |
|
| Moderate |
130 (42.6) |
| Severe |
175 (57.4) |
| Mean (SD) |
9.19 (3.19) |
| Depression symptoms (DASS-D) |
|
| Moderate |
230 (75.4) |
| Severe |
75 (24.6) |
| Mean (SD) |
9.32 (3.27) |
| Quality of life (WHOQOL-BREF) |
|
| Bad |
12 (3.9) |
| Moderate |
183 (60.0) |
| Good |
110 (36.1) |
| Mean (SD) |
89.45 (15.71) |
Table 3.
ZBI-12 scores (N = 305)
|
ZBI-12 level of burden (score)
|
N (%)
|
95% CI
|
| None-mild burden (0-10) |
0 (0.0) |
0.0 |
| Moderate burden (11-20) |
176 (57.7) |
51.3-62.7 |
| High burden ( > 20) |
129 (42.3) |
36.4-47.7 |
| Mean (SD) |
20.42 (7.68) |
|
Table 4.
Association between significant factors and high level of burden in palliative caregivers
|
Factors
|
N
|
% Of high burden
|
Crude OR
|
95%CI
|
P
value
*
|
| Caregiver with illness |
| No |
192 |
31.3 |
1 |
2.12-5.61 |
< 0.001 |
| Yes |
113 |
61.1 |
3.45 |
|
| Social support |
|
|
|
|
|
| Low |
6 |
66.7 |
1 |
|
0.001 |
| Moderate |
44 |
65.9 |
0.96 |
0.64-1.33 |
| High |
255 |
37.6 |
0.31 |
0.14-0.55 |
| Depression symptoms |
| Moderate |
230 |
32.2 |
1 |
|
< 0.001 |
| Severe |
75 |
73.3 |
5.8 |
3.24-10.37 |
| Anxiety symptoms |
|
|
|
|
|
| Moderate |
130 |
20.8 |
1 |
|
< 0.001 |
| Severe |
175 |
58.3 |
5.33 |
3.17-8.96 |
| Stress symptoms |
|
|
|
|
|
| Mild |
126 |
19.8 |
1 |
|
< 0.001 |
| Moderate |
78 |
39.7 |
2.66 |
1.42-5.00 |
| Severe |
101 |
72.3 |
10.53 |
5.68-19.53 |
| Palliative care outcome (according to the POS) |
|
| Mild |
205 |
29.8 |
1 |
|
< 0.001 |
| Moderate |
84 |
67.9 |
4.99 |
2.88-8.61 |
| High/severe |
16 |
68.8 |
5.19 |
1.73-15.58 |
| Quality of life decreased by 1 point |
305 |
- |
1.06 |
1.04-1.07 |
< 0.001 |
*Simple logistic regression; Bold values indicate statistically significance association; OR = Odds Ratio; CI = Confidence interval.
Discussion
This study assessed the burden of FCs of PC patients at the commencement of PC, thereby reflecting the FCs’ circumstances prior to their initial engagement with PC services. Data on previous PC settings reveals that for the majority of patients, specifically 80%, this was their first encounter with any type of specialist PC.
It is important to note that all FCs providing PC reported experiencing some degree of burden, with nearly half indicating a high level, as evidenced by a mean ZBI-12 score of 20.42. The mean ZBI-12 score of this sample is comparable to that found in prior research employing a similar tool with FCs of patients with advanced cancer.29The enrollment of FCs through PC patients in our study, compared to the enrollment of FCs through both curative and PC patients in another study, may explain the increased caregiving burden.30 Kondeti et al carried out a study involving FCs of patients with advanced cancer receiving only PC services.29 They noted a high burden in 44.1% of this sample, with mild-to-moderate stress found in 51.7% of FCs. The results correspond with our study’s findings, suggesting a heightened caregiving burden among FCs in PC contexts relative to curative settings. Furthermore, a study in Thailand looked at the prevalence of FC burden among senior citizens using Caregiver Burden Inventory and found that more than 40% of them fell into the category of having a high caregiving burden.18Another research investigation has reported that the FC burden varied between 23.0% and 59.2%.6This prevalence aligns with the prevalence reported by other studies conducted outside Thailand that employed a comparable ZBI-22 scale.29,31-33
Psychological manifestations frequently occur among FCs. Researchers identified FCs exhibiting depressive symptoms as two times more likely to experience caregiver burden within this demographic. The majority of FCs experiencing burdens and displaying symptoms of depression reported moderate intensity. The psychological manifestations of FCs directly impact the care recipients. Numerous studies have linked depression among FCs to neglect.12,32,34 The inherent traits of depression, wherein individuals typically endure profound weariness and inhibition, can explain this occurrence.35 Furthermore, a prior systematic review and meta-analysis encompassing 56 independent comparisons and 9,847 caregivers from 20 countries indicate that subjective caregiver burden significantly correlates with depressive symptoms in caregivers of older adults and may lead to clinical depression.34
There are identified predictive factors that can be analyzed with a high level of FC burden, providing insight into their relationship and its strength. The strongest predictor of FC burden was anxiety. In this group of participants, it was shown that FCs exhibiting anxiety symptoms were 2.19 times more susceptible to FC burden. FCs facing burdens and exhibiting anxiety symptoms reported a moderate-to-severe intensity. A prior study of FCs in the most specialized PC facility revealed that FCs experiencing anxiety were three times more likely to exhibit abusive risk characteristics toward care recipients.32 Anxiety can take the form of tension, which can lead to aggressive behavior towards the elderly, and it is known to intensify over time. The results of our study were comparable to other reports about PC caregivers.12,36 Moreover, it is important to acknowledge that depression and anxiety often coexist and are not mutually exclusive.32
FCs with illness were 2.13 times more likely to develop a high level of burden. Compared to those without health issues, FCs with health issues had higher caregiver burden scores, indicating that personal health challenges increase FC burden. Over 50 percent of caregivers in a previous study reported having at least one chronic health condition.37 Caregiving creates a physical and mental burden that adversely affects the health of caregivers, and poor personal health disrupts personal QOL.9 Chronic illness among FCs often results in significant deficits in physical health and diminishes their physical strength, which is required to fulfill patient demands and caregiving responsibilities. This situation subsequently contributes to an increased burden on these caregivers. A study conducted on women caring for relatives found a significant association between chronic illnesses and caregiving burden.9This finding aligns with prior studies indicating that health issues are significant risk factors for FC burden.9,37,38
Interestingly, our results showed that there was a strong negative correlation between FC burden and QOL. FCs whose QOL had decreased by 1 point had a 1.04 times higher likelihood of experiencing a high level of burden. The quantitative results indicated that caregivers with lower QOL are much more likely to experience a high level of burden. Generally, FCs with higher levels of developmental burden show a decrease in QOL.39This finding aligns with research evaluating outcomes associated with caregiver load. An elevated caregiver burden associated with reduced QOL and rising depressive symptoms.6,35 Furthermore, we argue that the long-lasting nature of PC and the high care needs of PC patients make it so that FCs must deal with providing a lot of care, which lowers their QOL. In this context, FCs of PC patients require essential support, and we should extend various governmental and non-governmental resources and benefits to them.
Finally, regarding the predictive factors of a high level of FC burden in PC patients, four significant predictors were identified. The overall model successfully predicted FC burden 79.0% of the time, demonstrating its ability to distinguish between FCs who reported high levels of burden and those who did not. Depression and anxiety have a significant impact on FC burden. This aligns with prior research indicating that psychological discomfort, marked by elevated depression and anxiety, is directly associated with caregiver burden. Therefore, these characteristics can currently predict the emergence of burden syndrome in FCs.12
Even though this study used a sufficient sample size from two district health service networks, encompassing two district hospitals and 24 sub-district health-promoting hospitals in the south of Thailand, the study encountered limitations. First, a cross-sectional design was used to evaluate functional results at a specific point in a patient’s disease progression; however, the levels of pressure and satisfaction fluctuate over time. Therefore, we recommend conducting longitudinal investigations, such as prospective cohort studies to validate the patterns found in this research. Moreover, physical or psychological conditions in FCs were identified as potential confounding factors that could influence the results of caregiving burden.
Table 5.
Multiple logistic regression for the association between high level of burden and predictive variables among palliative caregivers
|
Factors
|
N
|
% Of high burden
|
Crude OR
|
Adjusted OR
|
95%CI
|
P
value
*
|
| Caregiver with illness |
|
|
|
|
|
0.007
|
| No |
192 |
31.3 |
1 |
1 |
|
|
| Yes |
113 |
61.1 |
3.45 |
2.13 |
1.23-3.70 |
|
| Depression symptoms |
|
|
|
|
|
0.025
|
| Moderate |
230 |
32.2 |
1 |
1 |
|
|
| Severe |
75 |
73.3 |
5.80 |
2.17 |
1.10-4.27 |
|
| Anxiety symptoms |
|
|
|
|
|
0.011
|
| Moderate |
130 |
20.8 |
1 |
1 |
|
|
| Severe |
175 |
58.3 |
5.33 |
2.19 |
1.19-4.01 |
|
| Quality of life decreased by 1 point |
305 |
- |
1.06 |
1.04 |
1.02-1.06 |
<0.001
|
*Binary logistic regression; Bold values indicate statistically significance association; OR = Odds Ratio; CI = Confidence interval.
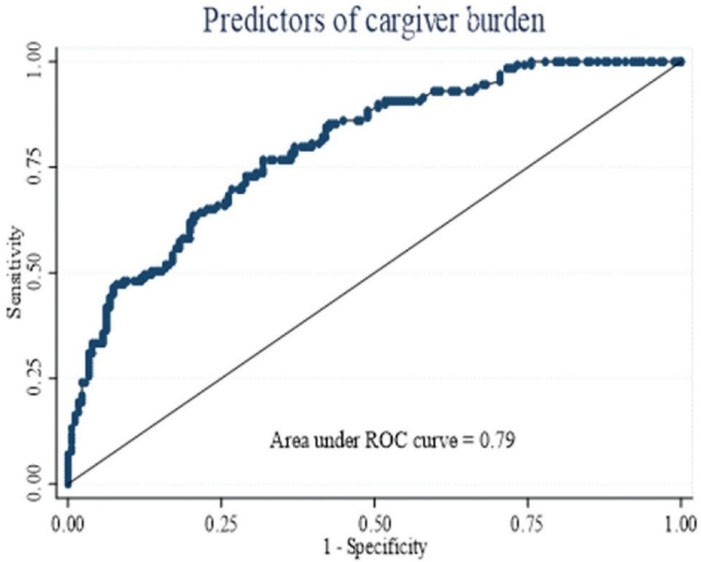
Figure 1.
Receiver operating characteristic curve of factors predicting a high level of caregiver burden. (The area under ROC curve = 0.79; 95% CI: 0.63-0.74 )
.
Receiver operating characteristic curve of factors predicting a high level of caregiver burden. (The area under ROC curve = 0.79; 95% CI: 0.63-0.74 )
Conclusion
FCs of patients receiving PC frequently experience a high level of burden. Mental health problems, particularly symptoms of depression and anxiety, diminished functional capacity, and poorer QOL, are associated with increased FC burden. Moreover, psychological manifestations such as feelings of anxiety and depression are prevalent in this population, and there is a strong correlation between these conditions and increased FC burden. Our findings highlight the need to support both the mental and physical health of FCs in order to advance the Sustainable Development Goals (SDGs), particularly in reducing mortality from noncommunicable diseases and promoting mental health. Preventive measures to prevent the emergence of such symptoms should be implemented. Hence, future research should investigate strategies designed to mitigate FC burden in this population, and the burden of FCs should receive greater emphasis in PC management and be incorporated into the development of local policies.
Competing Interests
The authors declare that they have no competing interests.
Data Availability Statement
The datasets produced and/or examined in this study are not publicly accessible due to university policies regarding data ownership; however, they can be obtained from the corresponding author upon reasonable request.
Ethical Approval
The research adhered to the ethical standards and principles established in the Declaration of Helsinki. The study protocol received ethical clearance from the Walailak University Institutional Review Board (Reference No. WUEC-23-344-01).
Research Highlights
What is the current knowledge?
-
Caregiver burden among FCs of cancer or elderly patients was prevalent in Thailand.
-
PC is predominantly provided at home as most patients prefer to remain close to their family members, particularly their children.
-
The reliance on FCs often leads to limitations in receiving professional healthcare assistance, creating gaps in comprehensive care for both patients and caregivers.
What is new here?
-
The predictive model of a high level of burden among FCs of Thai PC patients identified four significant predictors, which were depression symptoms, anxiety symptoms, caregivers with their own health problems, and reduced QOL. The overall model successfully predicted FC burden 79.0% of the time, indicating that this model could differentiate between FCs who reported a high level of burden and those who did not.
-
The results emphasize the growing awareness of the emotional and psychological challenges experienced by FCs, particularly in home care environments.
Acknowledgements
The authors express their gratitude to Dr. Orawan Silpakit for granting permission to use the Thai version of the 12-item ZBI, as well as all the caregivers who participated in this study. We value the participants’ readiness to furnish their personal information for the purpose of this research.
References
- World Health Organization (WHO). Strengthening of Palliative Care as a Component of Integrated Treatment Within the Continuum of Care. Geneva: WHO; 2014. p. 6.
- Ribé JM, Salamero M, Pérez-Testor C, Mercadal J, Aguilera C, Cleris M. Quality of life in family caregivers of schizophrenia patients in Spain: caregiver characteristics, caregiving burden, family functioning, and social and professional support. Int J Psychiatry Clin Pract 2018; 22(1):25-33. doi: 10.1080/13651501.2017.1360500 [Crossref] [ Google Scholar]
- World Health Organization (WHO). Global Atlas of Palliative Care. 2nd ed. London, UK: Worldwide Hospice and Palliative Care Alliance; 2020.
- Phetsitong R, Vapattanawong P, Sunpuwan M, Völker M. State of household need for caregivers and determinants of psychological burden among caregivers of older people in Thailand: an analysis from national surveys on older persons. PLoS One 2019; 14(12):e0226330. doi: 10.1371/journal.pone.0226330 [Crossref] [ Google Scholar]
- Sheehan OC, Leff B, Ritchie CS, Garrigues SK, Li L, Saliba D. A systematic literature review of the assessment of treatment burden experienced by patients and their caregivers. BMC Geriatr 2019; 19(1):262. doi: 10.1186/s12877-019-1222-z [Crossref] [ Google Scholar]
- Loo YX, Yan S, Low LL. Caregiver burden and its prevalence, measurement scales, predictive factors and impact: a review with an Asian perspective. Singapore Med J 2022; 63(10):593-603. doi: 10.11622/smedj.2021033 [Crossref] [ Google Scholar]
- Lee M, Williams IC. Predictive factors on caregiver burden in caregivers of individuals with cognitive impairment. Int J Care Coord 2022; 26(1):34-43. doi: 10.1177/20534345221148281 [Crossref] [ Google Scholar]
- Oechsle K, Ullrich A, Marx G, Benze G, Heine J, Dickel LM. Psychological burden in family caregivers of patients with advanced cancer at initiation of specialist inpatient palliative care. BMC Palliat Care 2019; 18(1):102. doi: 10.1186/s12904-019-0469-7 [Crossref] [ Google Scholar]
- Al-Daken LI, Ahmad MM. Predictors of burden and quality of sleep among family caregivers of patients with cancer. Support Care Cancer 2018; 26(11):3967-73. doi: 10.1007/s00520-018-4287-x [Crossref] [ Google Scholar]
- Sittironnarit G, Emprasertsuk W, Wannasewok K. Quality of life and subjective burden of primary dementia caregivers in Bangkok, Thailand. Asian J Psychiatr 2020; 48:101913. doi: 10.1016/j.ajp.2019.101913 [Crossref] [ Google Scholar]
- Guerriere D, Husain A, Zagorski B, Marshall D, Seow H, Brazil K. Predictors of caregiver burden across the home-based palliative care trajectory in Ontario, Canada. Health Soc Care Community 2016; 24(4):428-38. doi: 10.1111/hsc.12219 [Crossref] [ Google Scholar]
- Perpiñá-Galvañ J, Orts-Beneito N, Fernández-Alcántara M, García-Sanjuán S, García-Caro MP, Cabañero-Martínez MJ. Level of burden and health-related quality of life in caregivers of palliative care patients. Int J Environ Res Public Health 2019; 16(23):4806. doi: 10.3390/ijerph16234806 [Crossref] [ Google Scholar]
- Aung TNN, Aung MN, Moolphate S, Koyanagi Y, Supakankunti S, Yuasa M. Caregiver burden and associated factors for the respite care needs among the family caregivers of community dwelling senior citizens in Chiang Mai, Northern Thailand. Int J Environ Res Public Health 2021; 18(11):5873. doi: 10.3390/ijerph18115873 [Crossref] [ Google Scholar]
- Zhang Y, Li J, Zhang Y, Chen C, Guan C, Zhou L. Mediating effect of social support between caregiver burden and quality of life among family caregivers of cancer patients in palliative care units. Eur J Oncol Nurs 2024; 68:102509. doi: 10.1016/j.ejon.2024.102509 [Crossref] [ Google Scholar]
- Krug K, Miksch A, Peters-Klimm F, Engeser P, Szecsenyi J. Correlation between patient quality of life in palliative care and burden of their family caregivers: a prospective observational cohort study. BMC Palliat Care 2016; 15:4. doi: 10.1186/s12904-016-0082-y [Crossref] [ Google Scholar]
- Watanabe O, Chompikul J, Kawamori M, Pimpisan N, Visanuyothin S. Predictors of family caregiver burden in caring for older people in the urban district of Nakhon Ratchasima province, Thailand. Kokusai Hoken Iryo (J Int Health) 2019; 34(4):217-28. doi: 10.11197/jaih.34.217 [Crossref] [ Google Scholar]
- Tuttle D, Griffiths J, Kaunnil A. Predictors of caregiver burden in caregivers of older people with physical disabilities in a rural community. PLoS One 2022; 17(11):e0277177. doi: 10.1371/journal.pone.0277177 [Crossref] [ Google Scholar]
- Fumaneeshoat O, Ingviya T. Quality of life and burden of lung cancer patients’ caregivers: a cross-sectional study from southern Thailand. J Health Sci Med Res 2020; 38(3):177-92. doi: 10.31584/jhsmr.2020736 [Crossref] [ Google Scholar]
- Chaobankrang C, Anothaisintawee T, Kittichai K, Boongird C. Predictors of depression among Thai family caregivers of dementia patients in primary care. Int J Gerontol Geriatr Res 2019; 3(1):7-13. [ Google Scholar]
- Daniel WW, Cross CL. Biostatistics: A Foundation for Analysis in the Health Sciences. John Wiley & Sons; 2018.
- Tabachnick BG, Fidell LS, Ullman JB. Using Multivariate Statistics. Boston, MA: Pearson; 2013.
- Bédard M, Molloy DW, Squire L, Dubois S, Lever JA, O’Donnell M. The Zarit Burden Interview: a new short version and screening version. Gerontologist 2001; 41(5):652-7. doi: 10.1093/geront/41.5.652 [Crossref] [ Google Scholar]
- Silpakit O, Silpakit C, Chomchuen R. Psychometric study of the Thai version of Zarit Burden Interview in psychiatric caregivers. J Ment Health Thai 2015; 23(1):12-24. [ Google Scholar]
- Wittayapun Y, Summart U, Polpanadham P, Direksunthorn T, Paokanha R, Judabood N. Validation of depression, anxiety, and stress scales (DASS-21) among Thai nursing students in an online learning environment during the COVID-19 outbreak: a multi-center study. PLoS One 2023; 18(6):e0288041. doi: 10.1371/journal.pone.0288041 [Crossref] [ Google Scholar]
- Gholami A, Moosavi Jahromi L, Zarei E, Dehghan A. Application of WHOQOL-BREF in measuring quality of life in health-care staff. Int J Prev Med 2013; 4(7):809-17. [ Google Scholar]
- Pukrittayakamee P, Sapinum L, Suwan P, Harding R. Validity, reliability, and responsiveness of the Thai palliative care outcome scale staff and patient versions among cancer patients. J Pain Symptom Manage 2018; 56(3):414-20. doi: 10.1016/j.jpainsymman.2018.05.025 [Crossref] [ Google Scholar]
- Campo-Arias A, Caballero-Domínguez CC. Confirmatory factor analysis of the family APGAR questionnaire. Rev Colomb Psiquiatr (Engl Ed) 2021; 50(4):234-7. doi: 10.1016/j.rcpeng.2021.10.002 [Crossref] [ Google Scholar]
- Hosmer DW Jr, Lemeshow S, Sturdivant RX. Applied Logistic Regression. New Jersey: John Wiley & Sons; 2013.
- Kondeti AK, Yadala A, Rajya Lakshmi N, Prakash CSK, Palat G, Varthya SB. Assessment of caregiving burden of family caregivers of advanced cancer patients and their satisfaction with the dedicated inpatient palliative care provided to their patients: a cross-sectional study from a tertiary care centre in South Asia. Asian Pac J Cancer Prev 2021; 22(7):2109-15. doi: 10.31557/apjcp.2021.22.7.2109 [Crossref] [ Google Scholar]
- Kong SV, Guan NC. Burden in family caregivers of cancer patients: the association with depression, religiosity and religious coping. Asian Pac J Cancer Care 2019; 4(4):171-82. doi: 10.31557/apjcc.2019.4.4.171-182 [Crossref] [ Google Scholar]
- Palacio C, Krikorian A, Limonero JT. The influence of psychological factors on the burden of caregivers of patients with advanced cancer: resiliency and caregiver burden. Palliat Support Care 2018; 16(3):269-77. doi: 10.1017/s1478951517000268 [Crossref] [ Google Scholar]
- Ahmad Zubaidi ZS, Ariffin F, Oun CT, Katiman D. Caregiver burden among informal caregivers in the largest specialized palliative care unit in Malaysia: a cross sectional study. BMC Palliat Care 2020; 19(1):186. doi: 10.1186/s12904-020-00691-1 [Crossref] [ Google Scholar]
- Cengiz Z, Turan M, Olmaz D, Erce Ç. Care burden and quality of life in family caregivers of palliative care patients. J Soc Work End Life Palliat Care 2021; 17(1):50-63. doi: 10.1080/15524256.2021.1888844 [Crossref] [ Google Scholar]
- Del-Pino-Casado R, Rodríguez Cardosa M, López-Martínez C, Orgeta V. The association between subjective caregiver burden and depressive symptoms in carers of older relatives: a systematic review and meta-analysis. PLoS One 2019; 14(5):e0217648. doi: 10.1371/journal.pone.0217648 [Crossref] [ Google Scholar]
- Orfila F, Coma-Solé M, Cabanas M, Cegri-Lombardo F, Moleras-Serra A, Pujol-Ribera E. Family caregiver mistreatment of the elderly: prevalence of risk and associated factors. BMC Public Health 2018; 18(1):167. doi: 10.1186/s12889-018-5067-8 [Crossref] [ Google Scholar]
- Öksüz E. Investigation of caregiver burden, anxiety, and depression in caregivers of the palliative patients according to certain variables. Int J Caring Sci 2022; 15(1):352-60. [ Google Scholar]
- Bekdemir A, Ilhan N. Predictors of caregiver burden in caregivers of bedridden patients. J Nurs Res 2019; 27(3):e24. doi: 10.1097/jnr.0000000000000297 [Crossref] [ Google Scholar]
- Yigitalp G, Arda Sürücü H, Gumus F, Evinc E. Predictors of caregiver burden in primary caregivers of chronic patients. Int J Caring Sci 2017; 10(3):1168-77. [ Google Scholar]
- Marsack-Topolewski CN, Church HL. Impact of caregiver burden on quality of life for parents of adult children with autism spectrum disorder. Am J Intellect Dev Disabil 2019; 124(2):145-56. doi: 10.1352/1944-7558-124.2.145 [Crossref] [ Google Scholar]