Journal of caring sciences. 13(1):36-43.
doi: 10.34172/jcs.2024.33055
Original Article
An Investigation of the Effectiveness of Distance Learning on Nutrition Quality of Hemodialysis Patients during the COVID-19 Pandemic: A Single-Blind Randomized Clinical Trial
Mahdieh Rafiee Conceptualization, Data curation, Methodology, Project administration, Resources, Project administration, Validation, Visualization, Writing – review & editing, 1 
Maryam Khandan Conceptualization, 1, *
Author information:
1Department of Nursing, School of Nursing and Midwifery, Kerman Branch, Islamic Azad University, Kerman, Iran
Abstract
Introduction:
The COVID-19 pandemic has limited hemodialysis patient’s attendance in healthcare centers and receiving diet education. This study was conducted to investigate the effectiveness of distance learning on the nutrition quality of hemodialysis patients during the COVID-19 pandemic.
Methods:
In the single-blind randomized clinical trial, 60 patients undergoing hemodialysis were randomly divided into control (n=30) and experimental (n=30) groups. Before and after the intervention, Dialysis Malnutrition Score (DMS), Malnutrition-Inflammation Score (MIS) (primary outcome), albumin, the total iron-binding capacity of the blood (TIBC), and body mass index (BMI) (Secondary outcome) were investigated. The experimental group received educational content through social networks for three months, whereas the control group received routine care and training.
Results:
There was no significant difference between the two groups in terms of the mean of DMS, MIS, albumin, and TIBC before the intervention. Pre-test BMI had a confounding effect; therefore, an analysis of covariance was performed to eliminate that effect. This analysis showed significant differences in the post-test mean DMS, MIS, TIBC, and BMI between the two groups. In the control group, significant differences were observed in MIS and BMI toward deterioration. The results also indicated a significant relationship between education level and age with TIBC and between marital status and albumin index.
Conclusion:
Distance learning can be considered by healthcare managers and police makers as a suitable alternative to the classic face-to-face learning method to enhance hemodialysis patients’ nutrition quality during the COVID-19 pandemic.
Keywords: Distance Learning, Nutrition, Patients, Hemodialysis, COVID-19
Copyright and License Information
© 2024 The Author(s).
This work is published by Journal of Caring Sciences as an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by-nc/4.0/). Non-commercial uses of the work are permitted, provided the original work is properly cited.
Funding Statement
None.
Introduction
Chronic kidney disease (CKD) is a progressive, irreversible disorder in kidney function and structure associated with various clinical and laboratory abnormalities. The prognosis and the high prevalence of comorbidities have made CKD a public health problem.1 In the past three decades, the world has faced a significant rise in the number of CKD patients, and 89 % of end-stage kidney disease (ESKD) need to be treated through hemodialysis.2 The prevalence of this disease in Iran has been reported to be 108 per million.3 Despite the advancement of dialysis technology, and the predominance of hemodialysis, the mortality rate due to malnutrition in these patients is high.4 Malnutrition causes a severe decrease in these patients’ quality of life and compels them to adopt a diet to control disease progress.5 It has been reported in some studies that the limited information about a healthy diet is one of the main reasons for patients’ non-adherence to it.4,6 Although it improves and prolongs the lifespan of patients, hemodialysis will not be highly effective without following the diet, fluid restriction, and proper drug treatment.7 Therefore, hemodialysis patients need to receive accurate information about their diet.8
The COVID-19 preventive measures, such as social distancing, have affected individuals’ daily activities. It has also shifted healthcare education to nontraditional methods.9 This sudden alteration from face-to-face to online education has become possible thanks to different technologies.10 During the COVID-19 pandemic, distance education has played a vital role and has provided the opportunity for flexible learning, both simultaneously and separately.11 Since CKD patients have a lifetime need to receive education, the COVID-19 pandemic limitations on transportation have had more damaging effects on their health.9
Many studies show that the routine and traditional training provided to CKD patients undergoing hemodialysis has had favorable effects on their diet and treatment adherence, blood factors, and prevention and control of malnutrition.12,13 On the other hand, some researchers believe nurses also benefit from electronic education as a user-friendly and suitable method for teaching and as a more practical form of available learning to improve the quality of education for patients since virtual education can store and retrieve information.14,15
In this study context, adults’ distance learning is defined as an education type that uses multimedia technologies based on computers, the internet, and social networks to transfer data or achieve specific learning goals. The use of social media has opened many doors for health professionals to educate patients at a distance.16 Additionally, studies have reported the effectiveness of this method alongside routine training.17,18 However, the fact that this type of training can be a suitable alternative for maintaining and improving health indicators during the coronavirus epidemic, travel restrictions, and reduced possibility of providing face-to-face and routine training have caused challenges.19 Due to the fact that the impact of educational methods can be affected by studies’ context, the effectiveness of distance learning on the nutrition quality of hemodialysis patients in the considered context during the COVID-19 outbreak was felt. Considering the importance of training a patient as one of the most important parts of healthcare and the nurse’s key role, the research team decided to investigate the effectiveness of distance learning on the nutrition quality of patients undergoing hemodialysis during the COVID-19 pandemic in southeastern Iran in 2020-2021.
Materials and Methods
This single-blind randomized controlled clinical trial investigated the effectiveness of distance learning methods on the nutritional quality of patients in the dialysis center affiliated with Jiroft University of Medical Sciences in southeastern Iran from December 2020 to February 2021 during the COVID-19 pandemic. Before the allocation, all the participants were notified that classifying would not harm them, and informed consent to participate in the study was obtained from all participants.
The sample size was calculated as 54 individuals using Başer et al12 study, considering the confidence level of 95%, the power of the test at 80%, the effect size of 14.4, and using the formula for the sample size (z0.975=1.96, z0.8=0.84, d=4.14, ϭ1=5.99, ϭ2=4.99). Considering a probability of 10 % sample attrition, the total size was determined to be 60.
The inclusion criteria included being a constant patient on hemodialysis, willingness to participate in the research, having access to a smartphone by oneself or a family member who directly takes care of the patient, and having the lowest literacy level. The exclusion criteria included the participant’s unwillingness to continue, diseases, disorders, unpredicted conditions, such as a change in the treatment type, hospital admission for reasons other than hemodialysis, and the patient’s death. First, 60 out of 70 patients in the dialysis center were selected by simple random method using a table of random numbers generated by the computer. The allocation sequence was concealed by sequentially numbered and stapled pockets. The second author assigned participants to interventions. Afterward, they were randomly assigned to experimental and control groups using a block of four methods by a statistical consultant who was not involved in implementing the intervention and evaluating the results (one-sided blind). Patients were assigned to two groups using Random Allocation Software based on the “CONSORT” guidelines. Figure 1 illustrates the flowchart of the recruitment of the participants in the study. To achieve this, the experimental and the control groups were labeled A and B, respectively. The participants were randomly assigned to groups A and B in blocks of four (ABAB, BAAB, and the like).
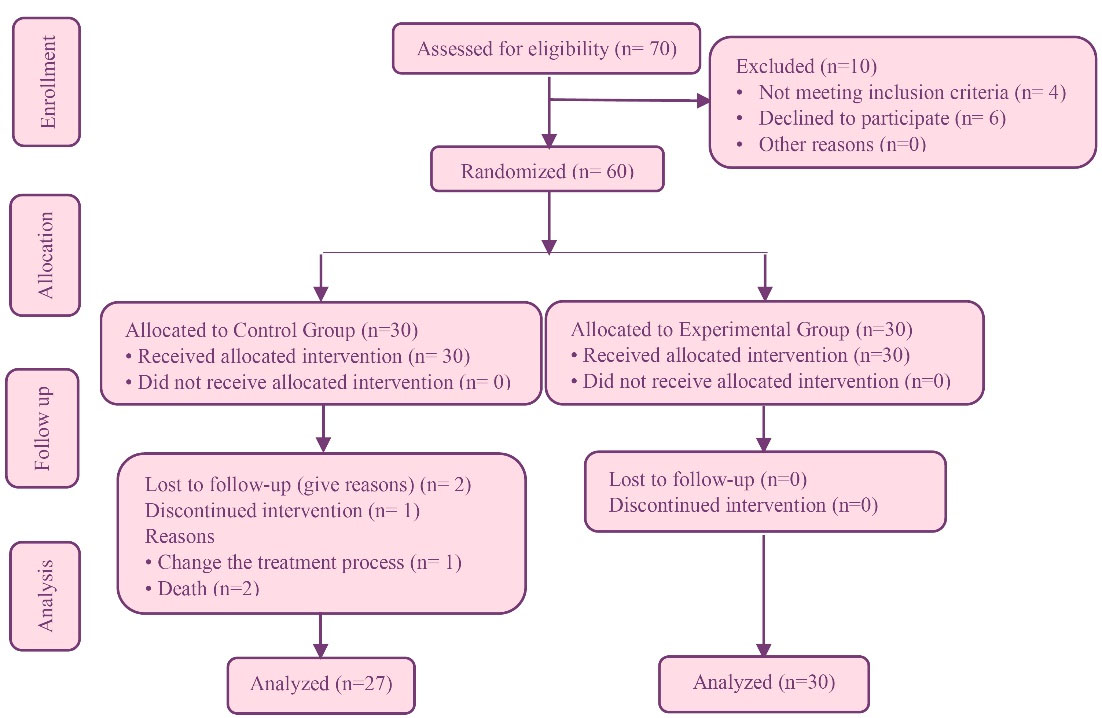
Figure 1.
Flowchart of the study
.
Flowchart of the study
The study involved collecting data from participants who were required to complete an informed consent form and attend the hospital with a family member at the appointed time and place. Blood samples were taken for albumin, total iron-binding capacity of the blood (TIBC) measurement were conducted after a 10-hour fasting period,20 and height and dry weight were measured using a calibrated digital medical scale with an accuracy (Camry, Iran) of 0.1 kg to calculate body mass index (BMI). All laboratory procedures were free of charge on the appointed day. Height was measured while standing without shoes, and weight was measured with the least amount of clothing using a calibrated scale with 100% accuracy and stability. The researchers then filled out questionnaires. After random allocation, the participants’ phone numbers were obtained to add them to a group on a social networking platform. At the end of the study, blood sampling, BMI calculation, and questionnaire completion were performed for both groups again.
The educational content topics were arranged based on the educational needs and nutritional literacy level of the participants in the experimental group. For this purpose, the Nutritional Knowledge Assessment Questionnaire for Hemodialysis, which includes six sections: fluid intake (4 questions), protein (4 questions), potassium (6 questions), sodium (2 questions), phosphorus (5 questions), and cooking methods (2 questions) was used. This instrument was psychometrically tested in the Persian language in the study by Montazeri and Sharifi.21 The educational content was arranged by the research team based on the qualitative assessment of patients’ nutritional knowledge. The prepared educational content was first approved by a nutritionist, a nephrology specialist, and a nursing professor and then processed for presentation in the virtual group (Table 1). During the study period, the control group received routine care and education, while the experimental group was provided with educational materials, including videos, images, and simple scientific texts, in addition to similar care and education for 12 weeks. In this way, over every week, educational materials were gradually added to the virtual group. For more interactions and according to the participants’ needs, online question-and-answer sessions and discussions were held between 30-40 minutes at the end of each week. At the end of the study, the educational content was provided to both experimental and control groups in the form of a handbook.
The primary outcomes were Dialysis Malnutrition Score (DMS) and Malnutrition Inflammation Score (MIS) in the intervention and control groups that were measured by the questionnaire. The data collection instrument consisted of three parts. The first part was demographic data, including gender, age, education, job, and marital status. The second part was the DMS, including seven questions, each with a score ranging from 1 (completely natural) to 5 (the most severe undesired status) and a range of 7-35. DMS between 7 and 13 were considered normal nutrition status, 14-23 moderate malnutrition, and 24-35 severe malnutrition. The third part of the questionnaire was related to MIS, including ten items, such as BMI, albumin concentration, and TIBC considered as secondary outcomes. Each question was scored between 0 (completely natural) and 3 (most severe). DMS between 0 and 30 were considered normal nutrition status, between 8 and 18 moderate malnutrition, and between 19 and 30 severe malnutrition. This instrument was psychometrically tested in the study by Tabibi et al22 in Persian.
The mean and standard deviation were used to analyze the data in the descriptive statistics section using SPSS version 13. Moreover, frequencies and percentages were used to describe the qualitative variables. Data normality was investigated through skewness and kurtosis, indicating that the DMS and MIS indices were in the ranges of ± 2 and ± 3, respectively, and the data were normally distributed.23 Therefore, the study utilized parametric tests in the inferential statistics section. Hence, the primary and secondary outcomes’ analyses were performed based on the study’s aims. An independent t test was used to compare the mean scores of MIS and DMS between the experimental and control groups before the intervention. Analysis of covariance was conducted for the pre-test scores, which showed significant differences between the groups. This approach allowed the researchers to investigate the effect of the intervention independently from the pre-test effect, revealing a significant difference between the adjusted group mean scores.24 The paired-samples t test was used to compare the mean DMS and MIS pre-test and post-test scores. Furthermore, a univariate covariance test was used to investigate the effect of demographic variables on these indices.
Table 1.
Topics and content covered in the virtual learning program
|
Sessions
|
The educational contents
|
| Week 1 |
Getting to know and introducing, communicating with the participants, creating an atmosphere of trust, repeating the purpose of the study and the educational intervention process, presenting some materials about the structure and function of the kidneys |
| Week 2 |
Explaining acute and chronic kidney failure, its causes, symptoms, and treatments |
| Week 3 |
Explaining the hemodialysis process, its benefits and complications, and the role of BMI in health |
| Week 4 |
Describing a healthy diet and its role in a healthy life |
| Week 5 |
Categorizing foods into carbohydrates, fats, proteins, vitamins, and minerals and their place in the food pyramid |
| Week 6 |
Introducing foods containing sodium, potassium, phosphorus, calcium, magnesium, protein, and fat and their allowed consumption level |
| Week 7 |
Describing dietary obligations and prohibitions, bad eating habits, liquids consumption limitations |
| Week 8 |
Presenting the right method of food preparation and cooking and introducing suitable substitutes for foods |
| Week 9 |
Adjusting a diet based on clinical results such as protein excretion rate and serum creatinine level |
| Week 10 |
Describing the role of vitamins and supplements in health enhancement and how to consume them. |
| Week 11 |
Describing the role of workout and activeness and its importance in improving nutritional status |
| Week 12 |
Summarizing the contents and answering the participants' questions |
Results
During the study, one participant in the control group due to kidney transplantation and two participants due to death were excluded, resulting in a 27-participant group. Data Analysis showed no statistically significant demographic difference between the two groups (P>0.05). The predominant gender, educational level, occupation status, and marital status were female, elementary, unemployed, and married, respectively. Other demographic characteristics are presented in (Table 2).
Table 2.
Demographics characteristics of Participants (n=57)
|
Variable
|
Experimental (n=30)
|
Control (n=27)
|
P
|
|
No. (%)
|
No. (%)
|
| Sex |
|
|
0.46 |
| Female |
16 (53.3) |
17 (63.0) |
|
| Male |
14 (46.7) |
10 (37.0) |
|
| Marital status |
|
|
0.99a |
| Single |
3 (10) |
3 (11.1) |
|
| Married |
27 (90.0) |
24 (88.9) |
|
| Education |
|
|
0.75b |
| Elementary |
14 (46.7) |
14 (51.9) |
|
| High school diploma |
12 (40.0) |
11 (40.7) |
|
| Higher education |
4 (13.3) |
2 (7.4) |
|
| Occupation |
|
|
0.99b |
| Unemployed |
22 (73.3) |
20 (74.1) |
|
| Employed |
7 (23.3) |
6 (22.2) |
|
| Self-employed |
1 (3.4) |
1 (3.7) |
|
| Age |
|
|
0.07c |
| Mean (SD) |
52.73 (16.70) |
60.77 (16.16) |
|
a Fisher's exact test, b Chi-square test, c Independent t test.
The two groups were measured for primary and secondary outcomes during the 12-week follow-up. The analysis revealed that before the intervention, the DMS was at a moderate level for more than half of the participants (68.42%), and the MIS was roughly equal at normal (49.12%) and moderate (50.87%) levels. No participant was at a severe level regarding these indices. The results also indicated no significant difference between the pre-test DMS and MIS in the two groups. In the primary outcome analyses, the results of covariance analysis (ANCOVA) showed significant differences between the post-test DMS and MIS of the two groups (P<0.001), with the experimental group being at a normal and the control group still at a moderate level. The results also showed that, according to the CONSORT, the effect size of the educational intervention was 0.487 based on DMS and 0.554 based on MIS, indicating a considerable difference among the study population. Other results showed that the pre-test TIBC and albumin mean scores between the experimental and control groups had no significant differences; however, the pre-test BMI mean scores between these two groups had a significant difference and were beyond the researcher’s control. To eliminate the effect of this variable with a probable confounding effect, Univariate ANCOVA was used. Therefore, the presumptions of the normal distribution of the data, homogeneity of variances, and regression slopes were first investigated and approved. In the secondary outcomes analyses, after eliminating the confounding effect of pre-test BMI, the ANCOVA results showed a significant difference between post-test TIBC and BMI between the two groups. The analysis revealed that the post-test mean scores of DMS and MIS in the experimental group significantly decreased compared to the pre-test scores. In the control group, a significant change was observed in the MIS index toward worsening. Another result showed that the post-test TIBC mean score in the experimental group significantly increased toward amelioration compared to the pre-test score; however, the increase in albumin and BMI mean score was not significant. There was no significant difference in the post-test mean score of TIBC and albumin in the control group compared to the pre-test score; however, there was a significant decrease in the post-test mean BMI score of this group compared to the pre-test score toward deterioration (Table 3).
Table 3.
DMS, MIS, TIBC, Albumin and BMI pre and post- test in experimental and control groups
|
Variable
|
Experimental (n=30)
|
Control (n=27)
|
t or f
|
P
|
ES
|
|
Mean (SD)
|
Mean (SD)
|
|
DMS
|
|
|
|
|
|
| Pre-test |
13.30 (3.30) |
15.03 (3.98) |
-1.79 |
0.07 |
|
| Post-test |
10.23 (1.97) |
14.81 (4.01) |
51.21 |
<0.001d |
0.48 |
| MD |
-3.06 |
-0.22 |
|
|
|
| t |
6.30 |
1.80 |
|
|
|
|
P
|
<0.001 |
0.08 |
|
|
|
|
MIS
|
|
|
|
|
|
| Pre-testa |
8.80 (3.65) |
10.59 (3.87) |
-1.79 |
0.07 |
|
| Post-testb |
5.70 (2.49) |
10.18 (3.48) |
67.01 |
< 0.001d |
0.55 |
| MD |
-3.10 |
-0.40 |
|
|
|
| tc |
7.30 |
2.18 |
|
|
|
|
P
|
<0.001 |
0.03 |
|
|
|
| TIBC |
|
|
|
|
|
| Pre-testa |
276.60 (39.94) |
282.66 (105.43) |
-0.29 |
0.771 |
|
| Post-testb |
316.10 (59.20) |
284.61 (49.12) |
4.82 |
0.032d |
0.08 |
| MD |
-36.5 |
-1.95 |
|
|
|
| tc |
-3.15 |
-0.09 |
|
|
|
|
P
|
0.004 |
0.92 |
|
|
|
| Albumin |
|
|
|
|
|
| Pre-testa |
4.06 (0.38) |
4.01 (0.31) |
0.46 |
0.64 |
|
| Post-testb |
4.15 (0.32) |
4.05 (0.34) |
0.95 |
0.33 |
0.01 |
| MD |
-0.08 |
-0.03 |
|
|
|
| tc |
-1.58 |
-0.65 |
|
|
|
|
P
|
0.12 |
0.51 |
|
|
|
| BMI |
|
|
|
|
|
| Pre-test |
23.08 (5.89) |
19.32 (3.17) |
2.94 |
0.005d |
|
| Post-test |
316.10 (59.20) |
284.61 (49.12) |
4.82 |
0.03d |
0.08 |
| MD |
0.33 |
0.38 |
|
|
|
| tc |
1.17 |
5.08 |
|
|
|
|
P
|
0.25 |
< 0.001 |
|
|
|
Abbreviations: DMS, Dialysis malnutrition score; MIS, Malnutrition inflammation scores; TIBC, Total iron binding capacity; BMI, Body mass index; MD, Mean
difference; ES, Effect size.
a Independent t test, b ANCOVA, c Paired t test; d Statistically significant.
The results of Univariate ANCOVA showed no significant relationship between demographic variables and DMS and MIS (P<0.05). Among these variables, a significant relationship was observed between TIBC and educational level (f=4.279, P=0.026) and age (f=12.074, P=0.002), as TIBC was lower in illiterate individuals (255/997) compared to patients with a high school diploma (339/390) and a university degree (353/848). Besides, TIBC increased with age. These differences were significant based on the Bonferroni Adjustment Test (P=0.032). There was also a significant relationship between marital status and albumin index (f=6.062, P=0.022). The mean albumin score in single patients (4.776) was higher than that of married ones (4.128). This difference was also significant based on the Bonferroni adjustment test. No significant relationship was observed between other demographic variables and albumin index or BMI.
Discussion
This study aimed to investigate the effectiveness of distance learning on hemodialysis patients’ nutrition quality during the COVID-19 pandemic in southeastern Iran in 2020. The data analysis showed that providing educational content virtually improved hemodialysis patients’ quality of nutrition and could successfully substitute traditional methods in distinct conditions, such as the COVID-19 pandemic, where access to face-to-face services is limited. Some studies show that in low- and middle-income countries, e-learning can reduce the impact of the severe shortage of health workers and provide high-quality education.25 A study has reported that hemodialysis patients’ adherence to a nutritional diet and treatment regimens was weak, and nutrition education through social networks significantly enhanced their electrolyte status.15 Based on the results of a study, a significant reduction was observed in hemodialysis patients’ non-adherence to diet in the experimental group receiving the educational intervention compared to that of the control group.12 Another study investigating the effect of education through text messages on hemodialysis patients’ acceptance of treatment regimens reported a positive effect of technology on treatment regimens acceptance. It also revealed that providing the necessary information improved their self-care.14 Accordingly, educational interventions and technology-based strategies have a great potential to maintain the long-term treatment adherence of ESKD patients undergoing dialysis and improve clinical outcomes in these patients.26 Consequently, Nurses can also help improve CKD patients’ health by integrating educational programs and providing diet information.27
Another result from the present study was that both DMS and MIS of more than half of the participants were at a moderate level before the educational intervention. Other studies conducted in Iran investigating the nutritional status of hemodialysis patients proved similar reports on poor nutritional status.6,28 In similar studies in South Africa, Egypt, and Palestine, the malnutrition status of hemodialysis patients was significant.29-31 Hence, to achieve the 2030 sustainable development goals, including health and, specifically, welfare and quality education, low- and middle-income countries need effective and affordable educational strategies due to the lack of qualified health workers. Therefore, e-learning can widely help achieve these goals.32
According to our findings, DMS and MIS indices in the experimental group improved significantly after the intervention, and in the control group, the MIS index increased significantly toward deterioration. Another study supports these results, reporting an improvement in dietary adherence among patients who received a training program.33 Similar results were reported; hemodialysis patients needed an educational program to provide them with the necessary information about diet.34 In contrast, in another study, no significant effect was observed on the nutrition status of hemodialysis patients. It was suggested that brief nutrition counseling was necessary for those patients, and the nutritional care program needed to be updated continuously for patients suffering from malnutrition.35 Lancet global commissioners also believe that, in this century, e-learning is a revolution that can improve the quality of providing educational services by strengthening health workers’ practical and continuous training.36
The study revealed that the experimental group exhibited a significant improvement in their TIBC score post-test, whereas no significant improvements were observed in the albumin index and BMI. On the other hand, the control group’s BMI score post-test showed a significant decrease, indicating a worsening of their condition. The researchers stress the importance of maintaining normal levels of serum albumin, TIBC, and BMI in hemodialysis patients, as these indicators provide valuable insights into their overall nutrition status.37 In the study by Pérez-Torres et al serum albumin and BMI of hemodialysis patients in the experimental group improved after the educational intervention.38 In a clinical trial, the patients’ mean weight decreased significantly after the educational intervention.39 The results of a study revealed no significant difference was observed in the albumin of the experimental group before and after the intervention.40 The study suggests that comprehensive nutrition services and counseling should be incorporated into the treatment plan for hemodialysis patients, particularly those with lower BMI, as measuring albumin and BMI is a simple and cost-effective means of assessing patients’ nutrition status. This approach can aid in identifying malnutrition in these patients and facilitating timely treatment.28
The study found no significant correlation between demographic variables and DMS and MIS scores. Previous studies have reported a higher prevalence of malnutrition in older and unmarried patients due to factors such as decreased mobility, decreased appetite, and difficulty in supplying and preparing meals.30 A study has revealed a direct relationship between malnutrition and age.31 One of the reasons for these differences is the emphasis on family support for sick people, especially the older people, in Iranian culture, which gives family caregivers an essential role in improving the health of sick family members.41
The study found that illiterate hemodialysis patients had lower TIBC levels compared to patients with higher education levels, and TIBC levels increased with age. Single patients had higher mean albumin values than married patients. These results differ from other studies, possibly due to differences in study contexts. Another study found no significant relationship between education and phosphate consumption in the diet regarding weight.42 A study has reported higher malnutrition among patients with lower education level.31 According to some researchers, variations in the prevalence of malnutrition and related factors in different studies may be attributed to several factors, including differences in malnutrition assessment methods, age, duration of illness, comorbidities, socio-economic factors, literacy, knowledge, patients’ awareness of kidney failure, and family support. Additionally, access to food, eating habits, and regional culture can also significantly impact the nutrition status of hemodialysis patients,28 which are suggested to be considered in future studies.
The study’s limitations include a small sample size and a short intervention duration, which might restrict the generalizability of the findings. Furthermore, the study did not explore the influence of patients’ social, cultural, and economic differences on the primary variables. To address these limitations and investigate additional factors that may impact the outcomes, the authors recommend conducting further studies with longer durations and larger sample sizes.
Conclusion
The results of the present study showed that during the COVID-19 pandemic, distance learning could be used as a suitable and reliable alternative to the traditional method to reduce hemodialysis patients’ malnutrition. Therefore, nursing managers and planners are suggested to consider distance learning methods to educate patients, improve their nutrition quality, and provide the necessary infrastructure for such services.
Acknowledgments
This article is the result of the MSc thesis by the first author (MR). The authors would like to appreciate the Vice-Chancellor for Research of the Islamic Azad University of Kerman brunch, staff of dialysis centers and the Patients undergoing hemodialysis who sincerely cooperated in this study. We wish to express our appreciation of Dr. Mohammadraza Kordbagheri, PhD in statistics, Faculty of Mathematical Sciences, Shahid Beheshti University, for his statistical consultation and valuable input.
COI-statement
The authors declare no conflict of interest.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Ethical Approval
The study protocol and all experiments comply with the Declaration of Helsinki and were approved by the Ethics Committee of the Islamic Azad University Kerman Branch (registration code IR.IAU.KERMAN.REC.1399.012) and received a clinical trial code (IRCT20210424051067N1) on 12/12/2020. The participants were ensured of voluntary participation in the study, data confidentiality, the anonymity of the questionnaires, and the right to withdraw from the study at any stage.
Research Highlights
What is the current knowledge?
What is new here?
References
- de Souza W, de Abreu LC, da Silva LG, Bezerra IMP. Incidence of chronic kidney disease hospitalisations and mortality in Espírito Santo between 1996 to 2017. PLoS One 2019; 14(11):e0224889. doi: 10.1371/journal.pone.0224889 [Crossref] [ Google Scholar]
- Liyanage T, Ninomiya T, Jha V, Neal B, Patrice HM, Okpechi I. Worldwide access to treatment for end-stage kidney disease: a systematic review. Lancet 2015; 385(9981):1975-82. doi: 10.1016/s0140-6736(14)61601-9 [Crossref] [ Google Scholar]
- Bouya S, Balouchi A, Rafiemanesh H, Hesaraki M. Prevalence of chronic kidney disease in Iranian general population: a meta-analysis and systematic review. Ther Apher Dial 2018; 22(6):594-9. doi: 10.1111/1744-9987.12716 [Crossref] [ Google Scholar]
- Sahathevan S, Khor BH, Ng HM, Abdul Gafor AH, Mat Daud ZA, Mafra D. Understanding development of malnutrition in hemodialysis patients: a narrative review. Nutrients 2020; 12(10):3147. doi: 10.3390/nu12103147 [Crossref] [ Google Scholar]
- Vanholder R, Fouque D, Glorieux G, Heine GH, Kanbay M, Mallamaci F. Clinical management of the uraemic syndrome in chronic kidney disease. Lancet Diabetes Endocrinol 2016; 4(4):360-73. doi: 10.1016/s2213-8587(16)00033-4 [Crossref] [ Google Scholar]
- Sohrabi Z, Eftekhari MH, Eskandari MH, Rezaeianzadeh A, Sagheb MM. Malnutrition-inflammation score and quality of life in hemodialysis patients: is there any correlation? Nephrourol Mon 2015; 7(3): e27445. is there any correlation? Nephrourol Mon 2015; 7(3):is there any correlation? Nephrourol Mon 2015; 7(3). doi: 10.5812/numonthly.7(3)2015.27445 [Crossref] [ Google Scholar]
- Tayebi A, Rahimi A, Einollahi B, Mirsadeghi A, Hashemi S. The effect of continues care model on adherence to treatment in hemodialysis patients. J Crit Care Nurs 2019; 12(2): 42-7. [Persian].
- Cupisti A, D’Alessandro C, Fumagalli G, Vigo V, Meola M, Cianchi C. Nutrition and physical activity in CKD patients. Kidney Blood Press Res 2014; 39(2-3):107-13. doi: 10.1159/000355784 [Crossref] [ Google Scholar]
- Kalantar-Zadeh K, Moore LW. Impact of nutrition and diet on COVID-19 infection and implications for kidney health and kidney disease management. J Ren Nutr 2020; 30(3):179-81. doi: 10.1053/j.jrn.2020.03.006 [Crossref] [ Google Scholar]
- Brown M, McCormack M, Reeves J, Brook DC, Grajek S, Alexander B, et al. 2020 Educause Horizon ReportTM | Teaching and Learning Edition [Internet]. Louisville, CO: Educause; 2020. Available from: https://library.educause.edu/resources/2020/3/2020-educause-horizon-report-teaching-and-learning-edition. Accessed September 20, 2023.
- Marshall AL, Wolanskyj-Spinner A. COVID-19: challenges and opportunities for educators and generation Z learners. Mayo Clin Proc 2020; 95(6):1135-7. doi: 10.1016/j.mayocp.2020.04.015 [Crossref] [ Google Scholar]
- Başer E, Mollaoğlu M. The effect of a hemodialysis patient education program on fluid control and dietary compliance. Hemodial Int 2019; 23(3):392-401. doi: 10.1111/hdi.12744 [Crossref] [ Google Scholar]
- Hernández Morante JJ, Sánchez-Villazala A, Cutillas RC, Fuentes MC. Effectiveness of a nutrition education program for the prevention and treatment of malnutrition in end-stage renal disease. J Ren Nutr 2014; 24(1):42-9. doi: 10.1053/j.jrn.2013.07.004 [Crossref] [ Google Scholar]
- Estaji Z, Hejazi S, Tabarraie Y, Saedi M. The effects of training through text messaging via cell phones on the compliance of patients undergoing hemodialysis. J North Khorasan Univ Med Sci 2016; 8(2):203-13. doi: 10.18869/acadpub.jnkums.8.2.203 [Crossref] [ Google Scholar]
- Naseri-Salahshour V, Sajadi M, Nikbakht-Nasrabadi A, Davodabady F, Fournier A. The effect of nutritional education program on quality of life and serum electrolytes levels in hemodialysis patients: a single-blind randomized controlled trial. Patient Educ Couns 2020; 103(9):1774-9. doi: 10.1016/j.pec.2020.03.021 [Crossref] [ Google Scholar]
- Proaño GV, Papoutsakis C, Lamers-Johnson E, Moloney L, Bailey MM, Abram JK. Evaluating the implementation of evidence-based kidney nutrition practice guidelines: the AUGmeNt study protocol. J Ren Nutr 2022; 32(5):613-25. doi: 10.1053/j.jrn.2021.09.006 [Crossref] [ Google Scholar]
- Helm J, Jones RM. Practice paper of the Academy of Nutrition and Dietetics: social media and the dietetics practitioner: opportunities, challenges, and best practices. J Acad Nutr Diet 2016; 116(11):1825-35. doi: 10.1016/j.jand.2016.09.003 [Crossref] [ Google Scholar]
- Yoon S, Wee S, Lee VSY, Lin J, Thumboo J. Patterns of use and perceived value of social media for population health among population health stakeholders: a cross-sectional web-based survey. BMC Public Health 2021; 21(1):1312. doi: 10.1186/s12889-021-11370-y [Crossref] [ Google Scholar]
- Biruete A, Kistler BM, Kalantar-Zadeh K, Moore LW. Kidney nutrition in the era of social media: bridging the gap of nutrition education and kidney health literacy by leveraging resources of social networking. J Ren Nutr 2022; 32(6):629-32. doi: 10.1053/j.jrn.2022.09.002 [Crossref] [ Google Scholar]
- Dukkipati R, Spatola L, Kalantar-Zadeh K, Shah A, Kopple JD. Nutritional management of maintenance hemodialysis patients. In: Kopple JD, Massry SG, Kalantar-Zadeh K, Fouque D, eds. Nutritional Management of Renal Disease. 4th ed. Academic Press; 2022. p. 557-91. 10.1016/b978-0-12-818540-7.00027-6
- Montazeri RS, Sharifi N. Evaluation of nutritional knowledge in terms of dietary sources of protein, phosphorous, potassium and fluids restriction in hemodialysis patients. Jentashapir J Cell Mol Biol 2014; 5(4):e21878. doi: 10.5812/jjhr.21878 [Crossref] [ Google Scholar]
- Tabibi H, Ashabi A, Nozari B, Mahdavi-Mazdeh M, Hedayati M, Abdollahi M. Comparison of various methods for determination of protein-energy malnutrition with subjective global assessment in hemodialysis patients. Iran J Nutr Sci Food Technol 2011; 5(4): 13-22. [Persian].
- Hancock GR, Mueller RO, Stapleton LM. The Reviewer’s Guide to Quantitative Methods in the Social Sciences. 2nd ed. Great Britain: Routledge; 2018.
- Pallant J. SPSS Survival Manual: A Step by Step Guide to Data Analysis Using IBM SPSS. 7th ed. Great Britain: Routledge; 2020.
- Barteit S, Guzek D, Jahn A, Bärnighausen T, Jorge MM, Neuhann F. Evaluation of e-learning for medical education in low- and middle-income countries: a systematic review. Comput Educ 2020; 145:103726. doi: 10.1016/j.compedu.2019.103726 [Crossref] [ Google Scholar]
- Murali KM, Lonergan M. Breaking the adherence barriers: strategies to improve treatment adherence in dialysis patients. Semin Dial 2020; 33(6):475-85. doi: 10.1111/sdi.12925 [Crossref] [ Google Scholar]
- Lim KA, Lee JH. Factors affecting quality of life in patients receiving hemodialysis. Iran J Public Health 2022; 51(2):355-63. doi: 10.18502/ijph.v51i2.8688 [Crossref] [ Google Scholar]
- Ghorbani A, Hayati F, Karandish M, Sabzali S. The prevalence of malnutrition in hemodialysis patients. J Renal Inj Prev 2020; 9(2):e15. doi: 10.34172/jrip.2020.15 [Crossref] [ Google Scholar]
- Agboton BL, Agueh VD, Vigan J, Sourou BA, Ahoui S, Agboton CG. Assessing the nutritional status of hemodialysis patients in a sub-Saharan country. J Kidney 2017; 3(2):145. doi: 10.4172/2472-1220.1000145 [Crossref] [ Google Scholar]
- Omari AM, Omari LS, Dagash HH, Sweileh WM, Natour N, Zyoud SH. Assessment of nutritional status in the maintenance of haemodialysis patients: a cross-sectional study from Palestine. BMC Nephrol 2019; 20(1):92. doi: 10.1186/s12882-019-1288-z [Crossref] [ Google Scholar]
- Zaki DS, Mohamed RR, Mohammed NA, Abdel-Zaher RB. Assessment of malnutrition status in hemodialysis patients. Clin Med Diagn 2019; 9(1):8-13. doi: 10.5923/j.cmd.20190901.02 [Crossref] [ Google Scholar]
- Al-Shorbaji N, Atun R, Car J, Majeed A, Wheeler EL, Beck D, et al. eLearning for Undergraduate Health Professional Education: A Systematic Review Informing a Radical Transformation of Health Workforce Development [Internet]. World Health Organization (WHO); 2015. Available from: https://www.who.int/publications/i/item/9789241508261. Accessed September 20, 2023.
- Nadri A, Khanoussi A, Hssaine Y, Chettati M, Fadili W, Laouad I. [Effect of a hemodialysis patient education on fluid control and dietary]. Nephrol Ther 2020; 16(6):353-8. doi: 10.1016/j.nephro.2020.03.011 [Crossref] [ Google Scholar]
- Kim S, Lim H. Level of nutrition knowledge, diet practice and education demands in dialysis patients with chronic renal failure. J Korean Diet Assoc 2018; 24(2):117-40. doi: 10.14373/jkda.2018.24.2.117 [Crossref] [ Google Scholar]
- Jo IY, Kim WJ, Park HC, Choi HY, Lee JE, Lee SM. Effect of personalized nutritional counseling on the nutritional status of hemodialysis patients. Clin Nutr Res 2017; 6(4):285-95. doi: 10.7762/cnr.2017.6.4.285 [Crossref] [ Google Scholar]
- Frenk J, Chen L, Bhutta ZA, Cohen J, Crisp N, Evans T. Health professionals for a new century: transforming education to strengthen health systems in an interdependent world. Lancet 2010; 376(9756):1923-58. doi: 10.1016/s0140-6736(10)61854-5 [Crossref] [ Google Scholar]
- Yu AS, Chertow GM, Luyckx V, Marsden PA, Skorecki K, Taal MW. Brenner and Rector’s the Kidney. 11th ed. Netherlands: Elsevier; 2019.
- Pérez-Torres A, González García ME, Ossorio-González M, Álvarez García L, Bajo MA, Del Peso G. The effect of nutritional interventions on long-term patient survival in advanced chronic kidney disease. Nutrients 2021; 13(2):621. doi: 10.3390/nu13020621 [Crossref] [ Google Scholar]
- Jafari F, Hashemi N, Reisi M. The effect of diet training on variations in blood pressure, weight, and some biochemical factors in hemodialysis patients: a clinical trial. J Clin Nurs Midwifery 2015; 3(4): 13-9. [Persian].
- Ebrahimi H, Sadeghi M. The effect of dietary regimen education on the laboratory variables in hemodialysis patients. J Nurs Educ 2014; 2(4): 12-22. [Persian].
- Tehranineshat B, Rakhshan M, Torabizadeh C, Fararouei M. Patient dignity in Iranian clinical care settings as perceived by physicians, caregivers, and patients. J Multidiscip Healthc 2020; 13:923-33. doi: 10.2147/jmdh.s258962 [Crossref] [ Google Scholar]
- Lim E, Hyun S, Lee JM, Kim S, Lee MJ, Lee SM. Effects of education on low-phosphate diet and phosphate binder intake to control serum phosphate among maintenance hemodialysis patients: a randomized controlled trial. Kidney Res Clin Pract 2018; 37(1):69-76. doi: 10.23876/j.krcp.2018.37.1.69 [Crossref] [ Google Scholar]