Journal of caring sciences.15(1) :20-29.
doi: 10.34172/jcs.026.33370
Original Article
Advancing the Theory of Communion-in-Caring: Framework, Pragmatic Utility, and Future Directions
Cyruz P. Tuppal 1, 2, * 
Author information:
1Institute of Nursing, University of Makati, Makati, Philippines
2Faculty of Nursing, Diponegoro University, Semarang, Indonesia
Abstract
Introduction:
Technological advancements in healthcare have greatly enhanced patient care but may overshadow essential elements like empathy and compassion. The Theory of Communion-in-Caring (TCIC) addresses this concern by focusing on the relational and communicative dimensions of care, thereby promoting deep, empathetic connections between nurses and patients. This study explores the framework, pragmatic utility, and future direction of TCIC within contemporary healthcare.
Methods:
This study employs a qualitative theory-building approach that incorporates conceptual analysis, framework development, and pragmatic utility assessment. Existing caring theories, including Watson’s Human Caring, Leininger’s Culture Care, and Boykin & Schoenhofer’s Nursing as Caring, are examined to examine theoretical foundations. Pragmatic utility is evaluated through case studies of healthcare professionals who applied TCIC principles in clinical settings, with a focus on patient outcomes and satisfaction.
Results:
TCIC offers a transformative framework for patient care, prioritizing human connection and shared understanding. Nurses who applied TCIC principles reported enhanced patient relationships, increased patient satisfaction, and improved health outcomes. The theory’s emphasis on relational and communicative aspects of care distinguishes it from other caring models, offering a more holistic approach to nursing that addresses physical, emotional, and spiritual needs.
Conclusion:
TCIC with its unique focus on compassionate care, not only advocates for a shift from task-oriented nursing to a more relational and person-centered approach but also has the potential to revolutionize healthcare. As healthcare professionals increasingly recognize the value of empathy and human connection, TCIC can promote more holistic, compassionate, and patient-centered care.
Keywords: Communion, Communion-in-Caring, Caring theory, Relational care, Empathy, Nursing theory
Copyright and License Information
© 2025 The Author(s).
This work is published by Journal of Caring Sciences as an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/). Non-commercial uses of the work are permitted, provided the original work is properly cited.
Funding Statement
No funding was provided for this study.
Introduction
Caring, as a foundational construct in holistic nursing practice, has been widely examined for its significance in influencing patient well-being. Over time, numerous caring theories have emerged, each contributing to the development of nursing knowledge and practice.1
In the world of healthcare, where advancements in technology and medical interventions often take center stage, empathy and compassion can sometimes be overlooked.2-11 However, with the TCIC, there is a renewed focus on the power of human connection in patient care that emphasizes the need for nurses to go beyond treating physical ailments and truly connect with their patients on a deeper emotional level. It recognizes that healing involves the body, mind, and spirit.12,13
At its core, TCIC promotes a culture of compassion and empathy in healthcare settings.12 It encourages nurses to view their patients as unique individuals with stories, fears, and hopes. Nurses can adopt a more holistic, person-centered approach by acknowledging and addressing the emotional aspects of care. This theory draws on the belief that genuine human connection profoundly impacts the healing process. When patients feel seen, heard, and understood, they are more likely to participate in their care and engage meaningfully, which contributes to enhanced health outcomes.1,12 TCIC advocates for nurses to be attentive and responsive to their patient’s emotional needs, creating a therapeutic environment promoting healing and well-being.12 Implementing TCIC requires a shift in mindset and a commitment to fostering a caring culture within healthcare organizations. It involves recognizing every patient’s inherent worth and dignity and treating them with respect, kindness, and compassion.
While TCIC holds immense potential, it is essential to acknowledge its current limitations as a theory. One limitation is the lack of widespread awareness and understanding of this concept. Many individuals and organizations are unfamiliar with the theory or its implications, which slows its adoption and practical application. Another limitation lies in the difficulty of measuring and quantifying the impact of TCIC, a concept rooted in emotions and human connection, using traditional research methods. This limitation hampers the ability to gather empirical evidence and convince sceptics of its value.
Advancing the TCIC is crucial for several reasons. Firstly, in a world that often feels disconnected and fragmented, this theory offers hope and reminds us of the importance of fostering true communion with others. We can cultivate more meaningful, fulfilling, and supportive relationships by deepening our understanding of this concept. Secondly, advancing the TCIC allows us to explore new dimensions of empathy and compassion. As our society evolves, we must develop innovative approaches that address our complex challenges. By expanding our understanding of TCIC, we can uncover new ways to heal divisions and bridge gaps in our communities.
The TCIC emerges from this backdrop as a critical framework that emphasizes the importance of genuine human connection, empathy, and relational care in nursing practice. Accumulated evidence within nursing science has consistently demonstrated that empathy and compassion are decisive factors in shaping patient outcomes. Across decades of scholarship, numerous caring theories have informed nursing knowledge and practice. Despite their contributions, these frameworks often fail to encompass the profound relational and communicative dynamics required for authentic healing.
The TCIC stands out because it focuses explicitly on the inherent relational nature of caring. Unlike traditional task-oriented models of care, the TCIC advocates for nurses to engage with patients not merely as healthcare recipients but as human beings with unique stories, emotions, and existential experiences. It posits that healing involves the body, mind, and spirit and that the most profound form of care can only be achieved through authentic, compassionate relationships between nurse and patient. This theory thus proposes a shift in how care is conceptualized away from viewing nursing as a set of clinical tasks and toward understanding it as a profound interpersonal connection that enriches both the caregiver and the patient.
The theoretical foundation of the TCIC is deeply rooted in existing caring models, beginning with Katie Eriksson’s Caritative Caring, which foregrounds caritas, compassion, and the ethical obligation to alleviate suffering. Building on this foundation, the TCIC also draws from Jean Watson’s Theory of Human Caring, particularly its emphasis on human connection and the carative factors that guide therapeutic relationships. Yet, TCIC distinguishes itself by integrating Gabriel Marcel’s concept of communion, which highlights being-with another person in a manner that transcends presence and opens the possibility for deeper relational encounter. In this sense, TCIC extends both Eriksson’s and Watson’s contributions by more explicitly articulating the relational, communicative, and dialogical dimensions of care. While Eriksson and Watson offer profound insights into caring as an ethical and humanistic practice, their models give limited attention to the sustained relational dialogue and communion that unfold in healing environments. TCIC advances this discourse by emphasizing empathetic presence and relational communication, essential for fostering trust, affirming dignity, and promoting patient well-being.
Additionally, TCIC incorporates key insights from Madeleine Leininger’s Culture Care Diversity and Universality Theory, which underscores the centrality of cultural context in shaping human experiences and affirms that authentic, meaningful care must be delivered in ways that are culturally congruent and responsive. However, TCIC extends beyond cultural competence, proposing that true healing occurs when nurses engage with patients on a deeper, more emotional and spiritual level, acknowledging their inherent dignity and value as individuals.
Further, TCIC integrates Boykin & Schoenhofer’s Nursing as Caring Theory, which positions caring as central to nursing practice.3 While Nursing as Caring focuses on nurturing the human spirit, the TCIC adds a new dimension by addressing nurses’ moral and emotional responsibilities, promoting a shared connection that encourages both the nurse and the patient in a reciprocal, communion-based relationship. TCIC underscores the moral probity of caring, urging nurses to foster a soul-felt connection in every patient interaction, transforming healthcare into a more compassionate and holistic experience.
What makes TCIC distinctive is its explicit focus on the communicative and relational aspects of care that are often underrepresented or treated as secondary in other theories. TCIC introduces the concept of communion-in-caring, which stresses the importance of being present with patients and emotionally and spiritually attuned to them, creating a deep, therapeutic bond. This theory promotes communion as a way of being, in which nurses engage with their patients to enrich both parties’ well-being, fostering a healing environment grounded in mutual respect, empathy, and shared humanity.
Moreover, TCIC addresses the limitations of earlier caring models by introducing a multidimensional framework that integrates physical, emotional, psychological, and spiritual aspects of human existence. It advocates for integrating moral sensitivity and ethical care as essential elements of patient-nurse interactions, thereby creating a more comprehensive and humane approach to healthcare. In doing so, TCIC sets a new direction in caring sciences by foregrounding the relational essence of nursing and offering a framework for cultivating person-centered care that is both compassionate and contextually relevant.
The main purpose of this paper is to introduce the emergence and current progress of TCIC. It discusses the principles and key components of TCIC’s benefits and applications in various settings, case studies and real-life examples in action, criticisms and challenges, training and success stories, and testimonials from those who have embraced TCIC.
Research Highlights
What is the current knowledge?
Existing caring theories (Watson, Leininger, Eriksson, Boykin & Schoenhofer, Roach) emphasize empathy, cultural sensitivity, human connection, and the moral-ethical dimensions of caring.
Traditional caring models acknowledge relationality but often underdevelop the communicative, dialogical, and spiritual depth required for holistic healing.
Contemporary healthcare advancements risk overshadowing empathy and compassion, reinforcing task-oriented rather than relationally grounded care practices.
There is increasing recognition that patient satisfaction, adherence, and outcomes improve when nurses engage in authentic, compassionate, person-centered relationships.
What is new here?
This article presents an advanced and systematized articulation of the Theory of Communion-in-Caring (TCIC), refining its assumptions, principles, and relational essence.
TCIC introduces communion-in-caring as a distinct concept that deepens existing caring theories by foregrounding spiritual attunement, emotional presence, and moral sensitivity.
The study provides a structured theory-building process using conceptual analysis, imaginative-reflective-creative synthesis, and pragmatic utility assessment.
It offers pragmatic evidence from case-based applications showing improved therapeutic relationships, patient satisfaction, and health outcomes when TCIC principles are implemented.
TCIC proposes a multidimensional framework that addresses physical, emotional, psychological, spiritual, and cultural dimensions of care, offering a more holistic and context-responsive model.
The article outlines future directions for TCIC, including its integration in training, policy, and technologically mediated care (e.g., telehealth).
Materials and Methods
This research employs a theory-building approach grounded in qualitative methods and scholarly dialogues with experts in nursing theory development. The study integrates three critical methodologies: conceptual analysis, framework development, and pragmatic utility assessment. Critical reviews provided the analytic basis for each step of the theory development process and supported the interpretation of caring theories in real-world healthcare contexts (see Figure 1).
Conceptual Analysis: The foundation of the Theory of Communion-in-Caring (TCIC) was established through in-depth analysis of previous caring theories, including Jean Watson’s Human Caring, Madeleine Leininger’s Culture Care, and Boykin & Schoenhofer’s Nursing As Caring. The study aimed to identify gaps in current caring theories, explicitly focusing on care’s relational and communicative aspects in contemporary healthcare settings. The philosophical underpinning draws from Gabriel Marcel’s concept of communion, which emphasizes being with and having an empathetic presence in relationships. The analysis critically reviewed theoretical assumptions, principles, and constructs that differentiate TCIC from other theories, thereby clarifying its distinctive contributions.
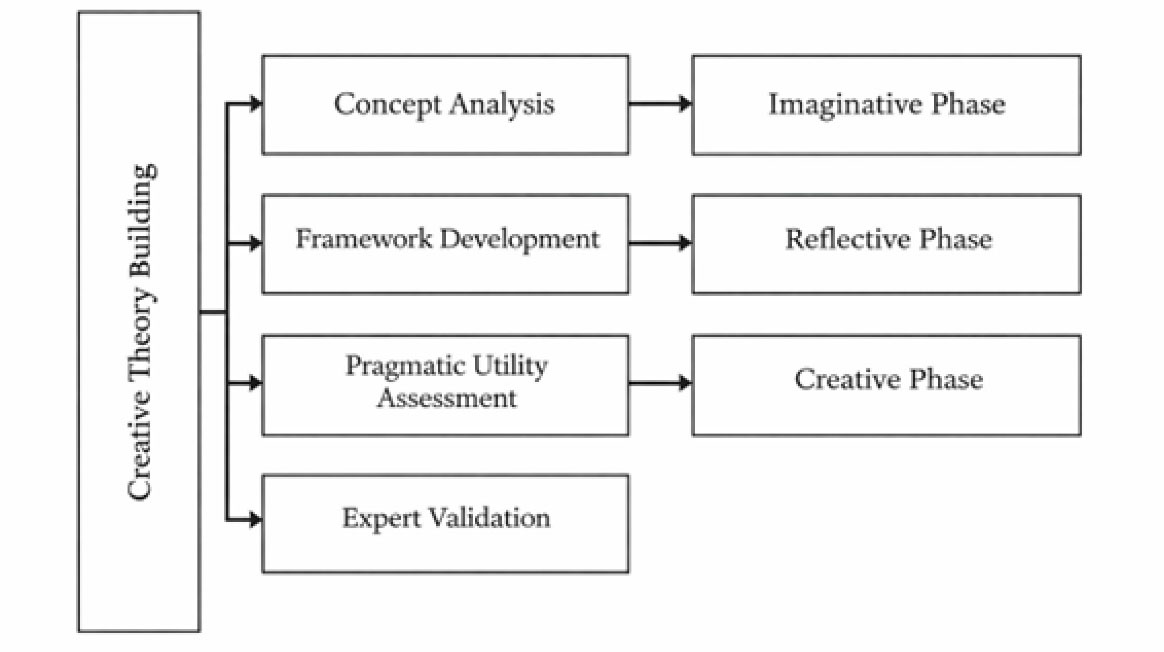
Figure 1.
The creative process in theory development
.
The creative process in theory development
Also, conceptual dialogue was employed as a primary methodological strategy to support the development and refinement of the TCIC. In the context of caring science, conceptual dialogue refers to a series of structured yet informal philosophical conversations among scholars who share a common interest in nature, meaning, and expression of caring. Rather than functioning as formal interviews, workshops, or data-gathering encounters, these dialogues serve as reflective spaces where theoretical assumptions are interrogated, clarified, and expanded.
At the Anne Boykin Institute for the Advancement of Caring in Nursing, conceptual dialogue involved exchanges with caring scholars who have extensive grounding in Nursing As Caring, caritative traditions, relational ethics, and humanistic philosophy. These dialogues were iterative, occurring over multiple sessions, and were guided by three central aims:
To examine foundational assumptions related to being, human connection, and the relational nature of caring;
To explore the ontological and epistemological commitments of emerging theoretical insights; and
To collaboratively refine the meaning and operationalization of key constructs within the developing theory.
Although not analyzed through empirical coding, conceptual dialogue follows a disciplined interpretive process. Insights generated from each dialogue were documented through reflective memos and analytic notes. These written reflections were then synthesized to identify points of convergence, theoretical tension, and emerging conceptual patterns. This iterative movement between dialogue, reflection, and synthesis served as the analytic mechanism through which the theory was shaped.
Framework Development: Building on conceptual analysis, this study employed an imaginative-reflective-creative synthesis method to develop the theory. This iterative process involved three stages. First, the imaginative phase explored new perspectives on empathy, human connection, and relational care in contemporary nursing. Second, the reflective phase evaluates how these new perspectives could address gaps in caring theories and align with the goals of holistic, person-centered care. Lastly, the creative phase entails integrating these insights into a coherent theoretical framework that defines the critical components of the TCIC and its intersection with other relevant theories in healthcare and psychology.
Pragmatic Utility Assessment: The utility of TCIC was assessed through case studies and practical applications across diverse healthcare settings, including hospital-based nursing, long-term care, and community health services. The evaluation employed a multi-method approach. Semi-structured interviews were conducted with healthcare professionals who implemented TCIC principles in their practice, enabling in-depth exploration of their experiences regarding patient satisfaction, therapeutic relationships, and perceived changes in health outcomes. These interview data were analyzed using thematic analysis to identify recurring patterns that demonstrated the theory’s practical relevance and effectiveness in fostering compassionate care. Additionally, field observations and practitioner narratives were examined to validate the contextual applicability of TCIC in real-world settings. Document reviews of clinical reports and reflective journals further supported the assessment by providing corroborative evidence. This comprehensive methodology accounted for the cultural competence required in diverse healthcare environments and underscored the adaptability and relevance of TCIC across various contexts.
Expert Validation: The final framework and its applications were validated through peer dialogues and expert reviews. This step ensured that the novel aspects of the TCIC were grounded in scholarly discourse and addressed critical needs in modern nursing theory. Peer-reviewed feedback from other nursing scholars helped refine the theory’s assumptions and applications.
Discussion
Development of TCIC
The TCIC resulted from a series of dialogues with other caring scholars at the Anne Boykin Institute for the Advancement of Caring in Nursing. Specifically, Boykin & Schoenhofer inspired the development of this theory, which is grounded in Nursing As Caring. One of the assumptions is that persons are caring by virtue of their humanness,3 which served as a prelude to a creative theory development process.
The creative process in theory development involves a series of iterative steps that allow for the synthesis of ideas and concepts12. In the case of TCIC, this process can be described as an imaginative-reflective-creative synthesis. It begins with the imaginative phase, in which researchers explore different perspectives and possibilities to enhance the quality of care. Subsequently, a reflective phase ensued, during which the researchers conducted a critical examination of the implications of the emerging perspectives and identified areas of conceptual ambiguity and gaps in existing knowledge. Finally, in the creative phase, the emergent insights were systematically integrated, resulting in the formulation of a novel and comprehensive theory of communion-in-caring. The conceptualization of caring in nursing and theory development requires transcending task-oriented views to address the relational and existential dimensions of human connection and compassion. This approach recognizes that caring is not limited to the physical aspects of nursing but extends to the patient’s emotional, psychological, and spiritual well-being.
Caring Theories and Marcel’s Philosophy as Interwoven Framework
Caring theories serve as lenses through which nurses can view and interpret the needs and experiences of those they care for. They provide a framework for understanding the fundamental principles and values that underpin effective caring practices. Caring theories acknowledge that each individual has a unique identity, shaped by various factors such as culture, values, beliefs, and personal experiences. By understanding and respecting these identities, nurses can establish a deeper connection with care recipients and create an environment of trust and understanding. Caring theories, such as Jean Watson’s Theory of Human Caring, Madeleine Leininger’s Theory of Culture Care Diversity and Universality, Katie Eriksson’s Caring Communion, Boykin & Schoenhofer’s Nursing As Caring, Sister Simone Roach Concept of Caring, and Gabriel Marcel’s Philosophy of Communion are interwoven into the Theory of Communion-in-caring.
The Theory of Nursing As Caring, by Boykin & Schoenhofer, emphasizes the centrality of caring in nursing practice. According to Boykin & Schoenhofer,3 the core of nursing is nurturing and sustaining the human spirit through caring relationships.Nursing As Caring focuses on the idea that caring is the essence of nursing and is foundational to the nurse-patient relationship. Caring involves being fully present with the patient, listening attentively, and responding with empathy and compassion. It also involves recognizing and honoring the uniqueness and dignity of each individual. TCIC and the Theory of Nursing As Caring emphasizes the centrality of caring in nursing practice and the significance of creating a caring environment. By integrating the concepts of caring communion and Nursing As Caring, nurses can provide compassionate, holistic care that promotes healing and enhances the overall well-being of their patients.3,8,12
Jean Watson’s Theory of Human Caring emphasizes the transformative power of caring in healthcare.14 Watson believed that caring is a fundamental component of nursing and that it has the potential to promote healing and enhance the overall well-being of patients. According to Watson, caring involves being present with the patient, acknowledging their humanity, and connecting with them on a deep emotional level.11,14 The Theory of Human Caring consists of ten carative factors that guide nurses to provide compassionate care.9 These factors include cultivating a caring relationship, promoting a positive and supportive environment, and integrating the mind, body, and spirit in the healing process. Nurses can create a caring environment that fosters trust, empathy, and holistic healing by incorporating these factors into their practice. The TCIC and Watson’s Theory of Human Caring both emphasize the transformative power of caring in healthcare and the importance of fostering meaningful connections with patients. They recognize the significance of empathy, compassion, and trust in the nurse-patient relationship.11,12,14,15 By integrating the concepts of caring communion and the carative factors of Watson’s theory, nurses can create a caring environment that promotes healing and enhances the overall well-being of patients.12
Madeleine Leininger’s Theory of Culture Care Diversity and Universality is a nursing theory that focuses on the integration of cultural values and practices in healthcare. Leininger believed that culture plays a significant role in shaping how individuals perceive and experience health and illness. According to Leininger,4cultural care is an essential component of nursing care. She defines cultural care as the values, beliefs, and practices that influence how individuals from different cultures perceive and respond to healthcare. Leininger’s theory also emphasizes the concept of cultural competence.4,16 Cultural competence refers to the ability of nurses to work with individuals from diverse cultural backgrounds effectively.16 It involves being aware of one’s cultural biases, developing cultural knowledge and skills, and providing care sensitive to patients’ cultural needs and preferences. The TCIC also intersects with Madeleine Leininger’s Theory of Culture Care Diversity and Universality. Both theories emphasize the importance of cultural competence and integrating cultural values and practices in healthcare. By embracing the concepts of caring communion and cultural care, nurses can provide care that is sensitive to the cultural needs and preferences of their patients, leading to improved patient satisfaction and better health outcomes.4,12,17
Katie Eriksson’s caring communion is a concept central to the TCIC. It refers to fostering meaningful connections and compassionate relationships in healthcare. According to this theory, caring communion is essential for creating an environment of trust, empathy, and understanding between nurses and patients.18-20 Eriksson19 surmised that caring communion involves actively listening to patients, acknowledging their emotions and concerns, and responding with empathy and compassion. It requires nurses to be present in the moment and to engage in genuine, authentic interactions with their patients. By establishing a caring communion, nurses can create a safe and supportive space for patients to express their needs and concerns, leading to improved patient satisfaction and better health outcomes and extend to the relationships among nurses.20 Eriksson’s caring communion theory emphasizes the importance of empathy and compassion in healthcare interactions. Nurses must recognize each patient’s unique experiences and needs and approach their care with genuine care and understanding, empathy and compassion into their practice. Nurses can create a therapeutic relationship that fosters healing and well-being.
Sister Simone Roach’s work on caring has been construed as essential for the well-being of both patients and nurses. Roach emphasizes creating a caring environment that fosters trust, empathy, and open communication.6,21 One of the critical concepts in Roach’s theory is the idea of moral distress. Roach believes that nurses who cannot provide care that aligns with their values and ethics experience moral distress.22,23 This distress can significantly impact the well-being of both the provider and the patient. Roach argues that by creating a caring environment, nurses can prevent moral distress and promote ethical decision-making. Roach also emphasizes the importance of self-care for nurses. She believes that to care for others effectively, nurses must first care for themselves. This includes taking time for rest and relaxation, engaging in activities that bring joy and fulfillment, and seeking support when needed. The TCIC and Sister Simone Roach’s Caring as a human mode share a common goal of promoting caring and compassionate relationships in healthcare.
Gabriel Marcel, a renowned philosopher, had had a significant influence on the concept of caring in nursing.24 Marcel’s philosophy emphasizes the importance of human relationships and the role of empathy and compassion in cultivating genuine connections. Marcel’s concept of caring centers around the idea of “being with” others.25 He believed that true caring involves being fully present with another person, listening attentively, and responding with empathy and compassion. Marcel argues that through genuine caring relationships, individuals can experience a sense of community and belonging, which is essential for their well-being. In nursing, Marcel’s philosophy has been applied to the nurse-patient relationship. Nurses who embrace Marcel’s philosophy strive to be authentic in their interactions with patients, treating them as unique individuals with their own experiences and needs. When applying Marcel’s concept of communion in healthcare settings, nurses are encouraged to be fully present and engaged in their interactions with patients. This involves actively listening, empathizing, and creating a safe space for patients to express their concerns and emotions. By being present, nurses can establish a genuine connection that promotes trust and healing.
Drawing inspiration from and building upon existing caring theories, the TCIC recognizes individuals’ inherent caring nature and emphasizes the importance of human connection in providing holistic person-centered care. By embracing the principles of communion-in-caring, nurses can truly make a difference in their patients’ lives, creating a healing environment where patients feel valued.
Theoretical Assumptions
The TCIC has the following assumptions12:
Caring is inherent to all persons
12
: The first theoretical assumption of TCIC is that caring is not limited to healthcare professionals but is an inherent quality in all individuals. This assumption recognizes that everyone has the capacity to care, and nurses are responsible for nurturing and fostering this innate caring nature in themselves and others.
Persons are relational beings
12
: TCIC acknowledges that human beings are inherently relational and that connections with others play a vital role in our well-being. This assumption emphasizes the importance of building meaningful relationships with patients, families, and colleagues, as these relationships form the foundation of compassionate care.
Communion is a way of being that enriches and sustains moral sensitivity towards persons
12
: The third assumption of TCIC highlights the significance of communion, a deep sense of connectedness and understanding, in the provision of caring. This assumption recognizes that communion-in-caring enhances nurses’ moral sensitivity towards patients, enabling them to respond to their needs with compassion and empathy.
Communion-in-caring professes oneness in belonging-being-becoming where the mind, heart, and soul meet
12
: TCIC posits that communion-in-caring involves a profound sense of oneness, where the mind, heart, and soul converge. This assumption reflects the holistic nature of nursing. It emphasizes the need for nurses to engage with patients not only on a physical level but also on an emotional and spiritual level.
Love, hope, faith, and charity are foundational acts—motives of caring
12
: TCIC recognizes that love, hope, faith, and charity are fundamental motivations for caring. These acts of compassion and kindness form the core of nursing practice and guide nurses in their interactions with patients.
Communion-in-caring epitomizes the practice of nursing, the phenomenon of caring, and perspicuity in human conditions
12
: This assumption underscores the central role of communion-in-caring in nursing practice. It acknowledges that communion-in-caring is not only a way of being for individual nurses but also a fundamental aspect of the nursing profession as a whole. It encompasses the phenomenon of caring and enables nurses to gain perspicuity in understanding and addressing human conditions.
Communion-in-caring embodies a profound relational attunement that develops within a nurturing caring environment and is influenced by the meaning, essence, and cultural context of caring.
12
: TCIC recognizes the importance of creating a nurturing environment that fosters communion-in-caring. This assumption emphasizes the need for nurses to establish a deep sense of connection with their patients, colleagues, and the broader healthcare system. It also acknowledges the influence of cultural dynamics on the expression and experience of caring.
Caring is the purest essence of nursing, where communion-in-caring is grounded
12
: TCIC asserts that caring is the purest essence of nursing and that communion-in-caring serves as the foundation for this essential aspect of the profession. This assumption highlights the centrality of caring in nursing practice and emphasizes the need for nurses to ground their actions and decisions in a deep sense of communion.
A relational caring practice affirms nursing as a distinct and collaborative discipline whose work is shaped by a caring ontology and upheld by moral responsibility across all practice contexts.
12
: TCIC recognizes that a relational caring practice sets nursing apart as a distinct and unique discipline. This assumption emphasizes the collaborative nature of nursing, where caring is infused in all aspects of practice. It also highlights the importance of moral probity, ethical decision-making, and the integration of caring principles across all domains of nursing.
Lifeworld constitutes the known, knowable, and unknown phenomenon
12
: The final assumption of TCIC acknowledges that the lifeworld of individuals encompasses both the known and the unknown. This assumption recognizes the complexity and diversity of human experiences and emphasizes the need for nurses to approach each patient with an open mind and a willingness to explore the unknown.
TCIC and Other Theories and Approaches in Psychology and Healthcare
TCIC is not an isolated theory but aligns with other psychology and healthcare theories and approaches. This alignment further strengthens the case for incorporating TCIC principles into healthcare practice. One area where TCIC aligns is with person-centered care. Person-centered care is an approach that recognizes the importance of treating patients as individuals with unique needs, preferences, and values.26,27 It emphasizes the active involvement of patients in their care and the importance of building a collaborative relationship between nurses and patients. TCIC complements person-centered care by emphasizing the emotional aspects of care and the need for human connection. Another area where TCIC aligns is with the biopsychosocial model of healthcare. The biopsychosocial model recognizes biological, psychological, and social factors influence health and illness. It highlights the importance of addressing not only the physical aspects of health but also the psychological and social dimensions.28 TCIC aligns with this model by emphasizing the need to address patients’ emotional and social needs in addition to their physical health. Furthermore, TCIC aligns with theories and approaches in psychology that emphasize the importance of empathy and compassion in therapeutic relationships.29 For example, Carl Rogers’ person-centered therapy30 and Martin Seligman’s positive psychology31 both emphasize the importance of empathy, compassion, and human connection in promoting emotional well-being and growth. By aligning with these theories and approaches, TCIC strengthens its foundation and further validates its potential for transforming healthcare practice.1
Principles of TCIC
The TCIC rests on a set of foundational principles and essential components that support its application in nursing practice. Together, these elements establish a patient-centered model of care that emphasizes empathy, compassion, and human connection.1,12,32 TCIC emphasizes seeing patients with unique needs, preferences, and experiences. Nurses can provide personalized care that considers the whole person by acknowledging and respecting their uniqueness. Creating a safe and supportive environment fosters trust and open communication between nurses and patients.33 This involves actively listening to patients, addressing their concerns, and ensuring their physical and emotional well-being. Active and reflective listening is a fundamental component of TCIC. It involves being fully present in the moment and giving patients your undivided attention.34,35 Nurses can better understand their needs and provide appropriate support by truly listening to patients’ concerns and fears. Empathy and compassion are at the heart of TCIC. Nurses are encouraged to put themselves in their patients’ shoes, to understand their emotions, and to respond in a compassionate and empathetic manner.36 This helps to build trust and strengthen therapeutic relationships. Self-awareness is crucial for nurses practicing TCIC. It involves recognizing one’s biases, emotions, and limitations and consciously working to overcome them. By cultivating self-awareness, nurses can better connect with their patients and provide genuinely person-centric care.37 TCIC promotes shared decision-making between nurses and patients. It involves actively involving patients in their care by providing them with information, options, and support to make informed decisions about their treatment. By embracing these principles and critical components, nurses can create a caring and compassionate environment that improves patient experiences and improves health outcomes.1,12
Pragmatic Utility of Communion-in-Caring in Various Settings
The application of TCIC is not limited to a specific healthcare setting but can be implemented in various healthcare contexts. Whether in hospitals, clinics, long-term care facilities, or even home healthcare, the principles of TCIC can have numerous benefits for both patients and nurses. One of the key benefits of implementing TCIC is improving patient satisfaction. When patients feel heard, understood, and cared for emotionally, they are more likely to report higher levels of satisfaction with their healthcare experience.38 This can increase patient loyalty, positive word-of-mouth referrals, and a reputation for healthcare organizations. In addition to improved patient satisfaction, TCIC can lead to better health outcomes. When nurses actively engage with patients on an emotional level, patients are more likely to adhere to their treatment plans, make necessary lifestyle changes, and actively participate in their care.39 This can result in improved patient outcomes, reduced hospital readmissions, and overall better health for the patient.40
Success Stories of TCIC in Action
The impact of TCIC can best be understood through the stories and testimonials of nurses and patients who have embraced this theory and experienced its transformative power. One healthcare professional shared her experience implementing TCIC in her primary care practice. She described how actively listening to patient’s concerns and fears enabled her to understand their needs better and provide appropriate support. She noted that by incorporating empathy and compassion into her practice, she was able to build stronger relationships with her patients and witness positive changes in their health outcomes.1
Another success story comes from a patient, who was diagnosed with a chronic illness. He shared how his healthcare team embraced TCIC and made him feel like an active participant in his own care. He described how their compassionate approach helped him navigate the challenges of his illness and provided him with the emotional support he needed. The patient credited Communion-in-caring with not only improving his physical health but also his overall well-being.1 These success stories highlight TCIC’s transformative impact on nurses and patients. By embracing empathy, compassion, and human connection, nurses can create a caring and supportive environment that leads to improved patient experiences and better health outcomes.41
To truly understand the impact of TCIC, it is helpful to examine real-life examples and case studies where this theory has been successfully implemented. One such example is the case of a hospital that decided to adopt the principles of TCIC in its oncology department.1 The nurses in this department underwent training in active listening, empathy, and compassionate communication. They learned how to create a safe and supportive environment for their patients and make them feel valued and heard. The results were remarkable - patients reported feeling more supported, understood, and cared for, leading to increased patient satisfaction and improved health outcomes. Another public hospital implemented TCIC as part of its person-centred care approach. By incorporating the principles of empathy, compassion, and collaboration, the facility saw a significant reduction in incidents of agitation and improved overall well-being among residents. The staff reported feeling more connected to the patients and better equipped to address their emotional and psychosocial needs. These success stories demonstrate the transformative power of TCIC in healthcare settings.1 By prioritizing empathy, compassion, and human connection, nurses can create an environment that improves patient experiences and leads to better health outcomes.
Training and Resources for Implementing TCIC
Implementing TCIC requires a commitment to change and a willingness to embrace new approaches to patient care. To support nurses in this endeavor, various training programs and resources are available to help them develop the necessary skills and knowledge. Training programs focused on empathy, active listening, and compassionate communication can give nurses the tools to implement TCIC effectively. These programs often include workshops, role-playing exercises, and case studies that allow nurses to practice and refine their communication skills in a supportive environment. Furthermore, mentoring and peer support can be invaluable resources for nurses seeking to implement TCIC. Connecting with colleagues who have already embraced this approach can provide guidance, inspiration, and a sense of community. By investing in training and utilizing available resources, healthcare organizations can empower their staff to embrace the principles of TCIC and create a culture of compassion and empathy.
Criticisms and Challenges
While TCIC has gained recognition and support, it is not without its criticisms and challenges. Some may argue that the theory places too much emphasis on the emotional aspects of care, potentially detracting from the importance of evidence-based medicine. They say that nurses should prioritize medical interventions and treatments over emotional support. Another criticism is that implementing TCIC may require additional time and resources, which could burden already overworked nurses. Skeptics question whether healthcare organizations can realistically allocate the necessary resources to fully embrace this theory and provide the level of care it demands. However, some argue that nurses should maintain a certain level of detachment and objectivity to ensure that they can make unbiased medical decisions.42 Some may question whether the emotional connection fostered by TCIC may compromise these professional boundaries.43These criticisms and challenges highlight the need for ongoing dialogue and exploration of the theory. While TCIC has shown promise in improving patient experiences and health outcomes, it is essential to address these concerns and ensure that its implementation is practical and beneficial.
The Future of TCIC-based Approaches in Nursing and Healthcare
The TCIC holds immense potential for the future of nursing and healthcare. As we continue to recognize the importance of holistic care and patient-centered approaches, TCIC provides a framework that aligns with these evolving needs. It is crucial to explore the applications of TCIC in diverse healthcare settings and populations. By conducting rigorous research and gathering empirical evidence, we can strengthen the foundation of TCIC and expand its reach. Moreover, the integration of TCIC principles into healthcare policies and guidelines will ensure that caring practices are prioritized at the organizational level.1 By embedding TCIC into the fabric of healthcare systems, we can foster a culture of compassion and empathy that promotes healing and well-being. The increasing recognition of the importance of patient-centered care and holistic well-being has paved the way for integrating these theories into healthcare practice. Advancements in technology also provide opportunities for fostering communion in healthcare settings. Telehealth and remote monitoring platforms can facilitate meaningful interactions between nurses and patients, overcoming geographical barriers and enhancing accessibility to care.44
By applying TCIC in healthcare settings, nurses can create therapeutic relationships that foster healing, well-being, and personal growth.1 Although challenges and critiques exist, the future of communion-based approaches in healthcare is promising, with advancements in technology and ongoing research contributing to the development of effective interventions.45-47 As we navigate an increasingly disconnected world, the exploration and application of communion-based approaches become even more crucial. We can build a society rooted in compassion, understanding, and shared humanity by fostering genuine connections and meaningful interactions. As we move forward, let us remember the words of Dr. Cyruz Polero Tuppal, who said,
Nursing is not just about treating ailments but also about nurturing the human spirit. Communion-in-caring reminds us that at the heart of healthcare is the need for human connection, empathy, and compassion. We can create a future where care is truly person-centric, transformative, and healing through a soul-felt, in-synch connection.1
Conclusion
The TCIC offers a fresh perspective on the importance of empathy and compassion in healthcare. By emphasizing the significance of human connection in patient care, TCIC challenges traditional notions of healthcare and paves the way for a more patient-centric approach. The benefits of implementing TCIC are evident- improved patient satisfaction, better health outcomes, and strengthened therapeutic relationships. By fostering a caring culture and embracing empathy and compassion, nurses can create a transformative healthcare experience that encompasses patients’ physical, emotional, and spiritual needs. Nurses are encouraged to embrace TCIC and cultivate a caring mindset in their practice. The advancement of TCIC is happening through ongoing research, dialogue, and practical application. While limitations exist, the focus is on refining its framework, exploring diverse contexts, and integrating technology, positioning it for further development and potential transformation of healthcare practices.
Acknowledgments
The research team would like to thank the nurses for being part of a communion-based dialogic inquiry.
Competing Interests
The authors declare no competing interests.
Data Accessibility
Data supporting the findings of a study are available from the authors upon reasonable request.
Ethical Approval
Not applicable in this paper.
References
- Tuppal CP. The Theory of Communion-in-caring: A soul-felt, in-synch connection. in press.
- Boykin A, Parker ME, Schoenhofer SO. Aesthetic knowing grounded in an explicit conception of nursing. Nurs Sci Q 1994; 7(4):158-61. doi: 10.1177/089431849400700407 [Crossref] [ Google Scholar]
- Boykin A, Schoenhofer S. Nursing as caring: a model for transforming practice. New York, NLN Publ. 1993.
- Leininger MM. Leininger’s theory of nursing: cultural care diversity and universality. Nurs Sci Q 1988; 1(4):152-60. doi: 10.1177/089431848800100408 [Crossref] [ Google Scholar]
- Ray MA. Caring inquiry: The esthetic process in the way of compassion. In: Smith MC, Turkel MC, Wolf ZR, editors. Caring in Nursing Classics: An Essential Resource. New York, USA: Springer 1991. 339-45.
- Roach MS. Caring from the Heart: The Convergence of Caring and Spirituality: Paulist Press; 1997.
- Schoenhofer S. Love, beauty, and truth: fundamental nursing values. J Nurs Educ 1989; 28(8):382-4. doi: 10.3928/0148-4834-19891001-13 [Crossref] [ Google Scholar]
- Schoenhofer SO. Philosophical underpinnings of an emergent methodology for nursing as caring inquiry. Nurs Sci Q 2002; 15(4):275-80. doi: 10.1177/089431802320559173 [Crossref] [ Google Scholar]
- Sitzman K, Watson J. Caring science, mindful practice: Implementing Watson’s human caring theory: Springer Publishing Company; 2018.
- Sprecher S, Fehr B. Compassionate love for close others and humanity. Journal of Social and Personal Relationships 2005; 22(5):629-51. doi: 10.1177/0265407505056439 [Crossref] [ Google Scholar]
- Watson J. Caring theory as an ethical guide to administrative and clinical practices. Nurs Adm Q 2006; 30(1):48-55. doi: 10.1097/00006216-200601000-00008 [Crossref] [ Google Scholar]
- Tuppal CP, Vega PD, Tuppal SMP. Towards a theory of communion-in-caring. Scand J Caring Sci 2022; 36(2):524-35. doi: 10.1111/scs.13049 [Crossref] [ Google Scholar]
- Bailey DN. Caring Defined: A Comparison and Analysis. Int J Hum Caring. 2009(1):16-31. 10.20467/1091-5710.13.1.16
- Watson J. The theory of Human Caring: retrospective and prospective. Nurs Sci Q 1997; 10(1):49-52. doi: 10.1177/089431849701000114 [Crossref] [ Google Scholar]
- Dokecki PR, Newbrough JR, O’Gorman RT. Toward a community-oriented action research framework for spirituality: Community psychological and theological perspectives. Journal of Community Psychology 2001; 29(5):497-518. [ Google Scholar]
- Leininger M. Culture care theory, research, and practice. Nurs Sci Q 1996; 9(2):71-8. doi: 10.1177/089431849600900208 [Crossref] [ Google Scholar]
- Epner DE, Baile WF. Patient-centered care: the key to cultural competence. Ann Oncol 2012; 23 Suppl 3:33-42. doi: 10.1093/annonc/mds086 [Crossref] [ Google Scholar]
- Bergbom I, Nåden D, Nyström L. Bergbom I, Nåden D, Nyström LKatie Eriksson’s caring theoriesPart 1The caritative caring theory, the multidimensional health theory and the theory of human suffering. Scand J Caring Sci 2022; 36(3):782-90. doi: 10.1111/scs.13036 [Crossref] [ Google Scholar]
- Eriksson K. Eriksson KCaring paradigmsA study of the origins and the development of caring paradigms among nursing students. Scand J Caring Sci 1989; 3(4):169-76. doi: 10.1111/j.1471-6712.1989.tb00288.x [Crossref] [ Google Scholar]
- Eriksson K. Caring Science in a New Key. Nursing Science Quarterly 2002; 15(1):61-5. doi: 10.1177/089431840201500110 [Crossref] [ Google Scholar]
- Roach MS. Caring, the human mode of being: A blueprint for the health professions. Ottawa: Canadian Healthcare Association Press. Copy from Archives of Caring in Nursing, Christine E. Lynn College of Nursing, Florida Atlantic Univesity, ARC-005 Sister M. Simone Roach Papers, 1958-2005, used by permission; 2002.
- Roach MS. Caring Ontology: Ethics and the Call of Suffering. Int J Hum Caring (2):30–4. 10.20467/1091-5710.2.2.30
- Villeneuve MJ, Tschudin V, Storch J, Fowler MD, Peter E. A very human being: Sister Marie Simone Roach, 1922-2016. Nurs Inq 2016; 23(4):283-9. doi: 10.1111/nin.12168 [Crossref] [ Google Scholar]
- Doona ME, Haggerty LA, Chase SK. Nursing presence: an existential exploration of the concept. Sch Inq Nurs Pract 1997; 11(1):3-16; discussion 7. [ Google Scholar]
- Murchland BG. The Philosophy of Gabriel Marcel. The Review of Politics 1959; 21(2):339-56. doi: 10.1017/S0034670500022427 [Crossref] [ Google Scholar]
- Morgan S, Yoder LH. A concept analysis of person-centered care. J Holist Nurs 2012; 30(1):6-15. doi: 10.1177/0898010111412189 [Crossref] [ Google Scholar]
- Håkansson Eklund J, Holmström IK, Kumlin T, Kaminsky E, Skoglund K, Höglander J. “Same same or different?” A review of reviews of person-centered and patient-centered care. Patient Educ Couns 2019; 102(1):3-11. doi: 10.1016/j.pec.2018.08.029 [Crossref] [ Google Scholar]
- Lehman BJ, David DM, Gruber JA. Rethinking the biopsychosocial model of health: Understanding health as a dynamic system. Social and Personality Psychology Compass 2017; 11(8):e12328. [ Google Scholar]
- Percy M, Richardson C. Introducing nursing practice to student nurses: How can we promote care compassion and empathy. Nurse Educ Pract 2018; 29:200-5. doi: 10.1016/j.nepr.2018.01.008 [Crossref] [ Google Scholar]
- Rogers CR. Carl Rogers on the development of the person-centered approach. PCJ 1986; 1(3):257-9. [ Google Scholar]
- Seligman ME, Steen TA, Park N, Peterson C. Positive psychology progress: empirical validation of interventions. Am Psychol 2005; 60(5):410-21. doi: 10.1037/0003-066x.60.5.410 [Crossref] [ Google Scholar]
- Tuppal CP, C Reñosa MD, G Ninobla MM, Ruiz MG, Loresco RC. Amo Ergo Sum—I love, Therefore, I am–Emotional Synchrony: A Norris’ Method of Concept Clarification. Nurse Media Journal of Nursing 2019; 9(2):176-196. doi: 10.14710/nmjn.v0i0.23261 [Crossref] [ Google Scholar]
- McCabe C. Nurse-patient communication: an exploration of patients’ experiences. J Clin Nurs 2004; 13(1):41-9. doi: 10.1111/j.1365-2702.2004.00817.x [Crossref] [ Google Scholar]
- Arnold K. Behind the Mirror: Reflective Listening and its Tain in the Work of Carl Rogers. The Humanistic Psychologist 2014; 42(4):354-69. doi: 10.1080/08873267.2014.913247 [Crossref] [ Google Scholar]
- Sundararajan L. Echoes after Carl Rogers: “Reflective listening” revisited. The Humanistic Psychologist 1995; 23(2):259-71. doi: 10.1080/08873267.1995.9986828 [Crossref] [ Google Scholar]
- Bramley L, Matiti M. How does it really feel to be in my shoes? Patients’ experiences of compassion within nursing care and their perceptions of developing compassionate nurses. J Clin Nurs 2014; 23(19-20):2790-9. doi: 10.1111/jocn.12537 [Crossref] [ Google Scholar]
- Scheick DM. Developing self-aware mindfulness to manage countertransference in the nurse-client relationship: an evaluation and developmental study. J Prof Nurs 2011; 27(2):114-23. doi: 10.1016/j.profnurs.2010.10.005 [Crossref] [ Google Scholar]
- Edelen MO, Rodriguez A, Huang W, Gramling R, Ahluwalia SC. A novel Scale to Assess Palliative Care Patients’ Experience of Feeling Heard and Understood. J Pain Symptom Manage 2022;63(5):689–97.e1. 10.1016/j.jpainsymman.2022.01.002
- Forbat L, Cayless S, Knighting K, Cornwell J, Kearney N. Engaging patients in health care: an empirical study of the role of engagement on attitudes and action. Patient Educ Couns 2009; 74(1):84-90. doi: 10.1016/j.pec.2008.07.055 [Crossref] [ Google Scholar]
- Pomey MP, Ghadiri DP, Karazivan P, Fernandez N, Clavel N. Patients as partners: a qualitative study of patients’ engagement in their health care. PLoS One 2015; 10(4):e0122499. doi: 10.1371/journal.pone.0122499 [Crossref] [ Google Scholar]
- Reynolds W, Scott PA, Austin W. Nursing, empathy and perception of the moral. J Adv Nurs 2000; 32(1):235-42. doi: 10.1046/j.1365-2648.2000.01440.x [Crossref] [ Google Scholar]
- Solomon M. The rhetoric of dehumanization: an analysis of medical reports of the Tuskegee syphilis project. West J Speech Commun 1985; 49(4):233-47. doi: 10.1080/10570318509374200 [Crossref] [ Google Scholar]
- Halpern J. From detached concern to empathy: humanizing medical practice: Oxford University Press; 2001.
- Hartasanchez SA, Heen AF, Kunneman M, García-Bautista A, Hargraves IG, Prokop LJ. Remote shared decision making through telemedicine: A systematic review of the literature. Patient Educ Couns 2022; 105(2):356-65. doi: 10.1016/j.pec.2021.06.012 [Crossref] [ Google Scholar]
- Locsin RC. Technologic competence as caring in critical care nursing. Holist Nurs Pract 1998; 12(4):50-6. doi: 10.1097/00004650-199807000-00008 [Crossref] [ Google Scholar]
- Locsin RC. Technological competency as caring in nursing: A model for practice: Sigma Theta Tau International Indianapolis, IN; 2005.
- Locsin RC. The Co-Existence of Technology and Caring in the Theory of Technological Competency as Caring in Nursing. J Med Invest 2017;64(1.2):160–4. 10.2152/jmi.64.160